
Rib osteomyelitis is a very rare entity. In this case, acute osteomyelitis of rib occurred with a previous history of mediocre trauma. Presentation of rib osteomyelitis is very non-specific, so, it may be included as a possible differential diagnosis in children with chest wall pain.
Dr. Virendra Kumar Verma, Department of Orthopaedics, All India Institute of Medical Sciences, Bhopal - 462 020, Madhya Pradesh, India. E-mail: vkverma0505@gmail.com
Abstract
Introduction: The rib osteomyelitis is a very rare entity and it hardly accounts for 1% of all cases of osteomyelitis. In this case report, we are presenting a case of acute osteomyelitis of rib in a very young child, with a previous history of mediocre trauma over the chest wall.
Case Report: It is a case report of a young boy, who had sustained the blunt injury over the chest wall. The X-ray was unremarkable. After sometime, he presented to the hospital with the pain over the chest wall. Now, the X-ray showed the signs of rib osteomyelitis.
Conclusion: In children, the clinical presentation of rib osteomyelitis is very non-specific. Sometimes, the injury while playing, which is very usual in this age group may create the confusion. Hence, it may need high index of suspicion by the physician to include is as a possible diagnosis.
Keywords: Rib, osteomyelitis, chest wall.
Osteomyelitis of rib is supposed to be a very rare entity in both, temperate as well tropical region. The incidence of rib osteomyelitis is very less and it hardly accounts for 1% of all cases of osteomyelitis [1,2].
Literature suggests that etiology of rib osteomyelitis is associated with the tuberculosis or through hematogenous spread [3,4]. Rib osteomyelitis very commonly presents with fever and local sign of inflammation in the chest wall. On the contrary, in our case, the patient had only complaint of localized tenderness over chest wall which could have off targeted to the wrong suppositions. In this case report, we are presenting a case of acute osteomyelitis of rib in a very young child, which had a previous history of mediocre trauma over the chest wall. In this case, osteomyelitis of rib could have been due to hematogenous spread to the previously organized hematoma. Yet, we could not get, any primary source of infection in child.
A 5-year-old male child visited to outpatient department with his father with complaint of the pain over the lower and outer part of the left side of the chest for 1 week. Pain was continuous, vague in nature, and localized to the posterolateral part of lower part of the left side of chest, which increases on the exertion like playing and running. On examination, there was no any obvious swelling, no local rise of temperature, but the tenderness was present over the posterolateral part of chest, corresponding to the 8th, 9th, and 10th rib. On deep breathing, the pain was increasing.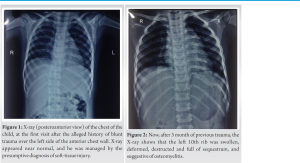
As stated by the father, 3 month back, his son has sustained the blunt trauma of chest over the same area while playing. For that he visited to the emergency department where the X-ray was done and he was managed symptomatically with presumptive diagnosis of soft-tissue injury of left side of chest wall (Fig. 1). The child remained apparently asymptomatic for the 3 month and now he presented with the localized pain over the same area of the chest.
On general examination, the patient was afebrile, heart rate of 122 beats per minute, respiratory rate of 20 per minute, and peripheral oxygen saturation was 96% on room air. The cardiac and pulmonary examination was within normal limit. On anteroposterior chest X-ray, the whole of the 10th rib (left side) was expanded, destructed and the sequestrum was seen (Fig. 2). The magnetic resonance imaging revealed that the 10th rib was deformed, and the medullary cavity was filled with the lobulated thin walled abscess. There was periosseous extension of abscess into the superior and inferior intercostal space (Fig. 3).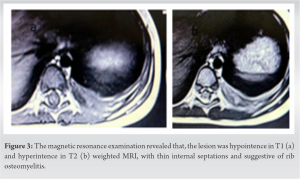
The hematological test showed the hemoglobulin of 11.5%, white blood count of 10300/microliter (neutrophils 45, lymphocytes 50, monocytes 03, eosinophils 02, and basophils 02), erythrocyte sedimentation rate (Westergren method) of 70 mm and C-Reactive protein (Nepholometry method) was 0.82. Liver function test and renal function test were unremarkable. Patient was examined thoroughly, but there was no any primary site of infection. Hence, the echocardiogram was done to rule out suspicion of endocarditis and it was also unremarkable.
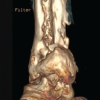
Since, there was the sequestrumand evident periosseous abscess, so the pus drainage and sequstrectomy was planned. Broad spectrum antibiotics were started (piperacillin/tazobactam) and the informed consent was obtained for the surgical intervention. In the right lateral position, the incision started posteriorly near the midline of the back, and thereafter the incision followed the course of the 10th rib as far as the costal cartilage. The sequestrum was removed and the pus pockets were drained, extending from the costovertebral angle to the costochondral junction and sent for the culture (Figs. 4 and 5). There was a minor breach of the pleura and it was repaired, so the chest tube was not placed. The wound was closed under negative suction. The Staphylococcus aureus was isolated from the pus, which was sensitive to piperacillin/tazobactam. The sensitive antibiotic was given for 4 weeks by parenteral route. At the end of 1 year of follow-up (Fig. 6), the child is happy and free from the disease .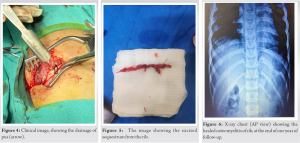
When was the last follow up visit? Post-X-ray of last follow-up?
Although the osteomyelitis of rib is a strange entity, the radiological findings such as fever, raised inflammatory markers, and local sign of inflammation in the chest wall should raise the high degree of suspicion for this rare disease. Osinowo et al. in his series (16 cases of rib osteomyelitis) found that the empyema thoracis was the most common cause of osteomyelitis of rib, which occurred at the site of chest tube insertion. They found that the wider and stiffer chest tube was a major causative factor for rib osteomyelitis. In his series, the second most common cause was the blunt trauma to the chest wall. After chest trauma, the organized hematoma diminishes the blood supply to rib. Furthermore, the subsequent hematogenous spread ensue the osteomyelitis of rib [5].
Rib osteomyelitis may present as a chronic discharging sinus, but in the most of the cases, the localized swelling is an early presenting feature [6,7]. In our case, the patient also presented with tender and localized swelling. Best of knowledge, only 61 case of rib osteomyelitis in children have been reported [8]. Usually, the common location of rib osteomyelitis is costochondral junction or costovertebral angle [9]. In our case, the costochondral junction and the whole rib were involved.
Rib osteomyelitis can be readily diagnosed, radiologically by the presence of expansion and destruction of the rib, extra pleural periosseous extension of abscess and sequestrum. However, sometime, it is rare presentation, as well as the subtle sign and symptom may be responsible for the delayed clinical diagnosis. In our case, only the pain was the presenting complaints, and which could have a strayed the diagnosis.
The most common cause of blood born rib osteomyelitis is S. aureus [10]. The preferred treatment of rib osteomyelitis is surgical intervention and the antibiotics [11]. In our case, the S. aureus was also the cause of rib osteomyelitis. Sequestrectomy and the proper antibiotics in our case provided the complete cure to the patient.
Although the guidelines regarding, at which duration the parenteral therapy to be switched to oral route are unavailable, but the duration of standard antimicrobial therapy is unanimously accepted for 4–6 weeks [12].
This case report shows the importance of rare presentation of post-traumatic rib osteomyelitis in children. In children, the clinical presentation of rib osteomyelitis may be very non-specific, so it may need high index of suspicion by the physician.
Uncommon and rare cause like rib osteomyelitis can be easily misdiagnosed, so it can be conceded as a differential diagnosis, while evaluating the pediatric patients, presenting with the abdominal pain, with the previous history of trauma.
References
- 1.Dich VQ, Nelson JD, Haltalin KC. Osteomyelitis in infants and children. A review of 163 cases. Am J Dis Child 1975;129:1273-8. [Google Scholar | PubMed]
- 2.Peltola H, Pääkkönen M. Acute osteomyelitis in children. N Engl J Med 2014;370:352-60. [Google Scholar | PubMed]
- 3.Kashyap NK, Jindal A, Borkar NK, Wasnik M. Primary tuberculotic osteomyelitis of rib in a child. J Clin Diagn Res 2017;11:D08-9. [Google Scholar | PubMed]
- 4.Annen MJ, Johnston MJ, Gormley JP, Silverman E. Acute hematogenous osteomyelitis presenting as a “Cold” rib in a child. World J Nucl Med 2017;16:160-2. [Google Scholar | PubMed]
- 5.Osinowo O, Adebo OA, Okubanjo AO. Osteomyelitis of the ribs in Ibadan. Thorax 1986;41:58-60. [Google Scholar | PubMed]
- 6.Komolafe F. Pyogenic osteomyelitis of the rib in children. Pediatr Radiol 1982;12:245-8. [Google Scholar | PubMed]
- 7.Crone AM, Wanner MR, Cooper ML, Fox TG, Jennings SG, Karmazyn B. Osteomyelitis of the ribs in children: A rare and potentially challenging diagnosis. Pediatr Radiol 2020;50:68-74. [Google Scholar | PubMed]
- 8.Nibley PD, Kraus CK. Rib osteomyelitis in a pediatric patient: Case report and review of the literature. Clin Pract Cases Emerg Med 2018;2:294-6. [Google Scholar | PubMed]
- 9.Raffaeli G, Borzani I, Pinzani R, Giannitto C, Principi N, Esposito S. Abdominal mass hiding rib osteomyelitis. Ital J Pediatr 2016;42:37. [Google Scholar | PubMed]
- 10.Goergens ED, McEvoy A, Watson M, Barrett IR. Acute osteomyelitis and septic arthritis in children. J Paediatr Child Health 2005;41:59-62. [Google Scholar | PubMed]
- 11.Guest JL Jr., Anderson JN. Osteomyelitis involving adjacent ribs. JAMA 1978;239:133. [Google Scholar | PubMed]
- 12.Harik NS, Smeltzer MS. Management of acute hematogenous osteomyelitis in children. Expert Rev Anti Infect Ther 2010;8:175-81. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report
July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series
July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature
June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature- May 1, 2026 Tibial Osteomyelitis due to Burkholderia pseudomallei in a Non-diabetic Patient: A Case Report