
To gain adequate knowledge to effectively manage complex fractures of the acromion process with adjacent soft tissue injuries.
Dr. Shreya D Gaware, Resident Doctor, Department of Orthopaedics, B. J. Government Medical College, Pune, Maharashtra, India. E-mail: sgaware96@gmail.com
Abstract
Introduction: Isolated acromion fractures are rare and in that too, orthopaedicians rarely come across open acromial fractures. Hence literature regarding their management, outcome and any associated complications is obscure. In an extensive search for literature related to our case we found very few articles. We hereby report a case of Gustilo IIIA open acromial fracture with associated supraspinatus, deltoid and capsular injury managed with tension band wiring (TBW) and soft tissue repair with 6 month follow up.
Case Report: A 21-year-old male was admitted in our hospital for wound of right shoulder with pain and inability to move this arm with a history of direct trauma with sharp object 3 days back. On examination, a wound 15 cm in length on the superior aspect of the right shoulder with its depth extending up to the glenohumeral joint was noted. The glenohumeral joint was exposed with a Gustilo Anderson type IIIA acromion fracture and injury of supraspinatus and capsule with no associated vascular or neurological injury. Wound was thoroughly irrigated and was used to approach the fracture site for repair. Capsule of shoulder was carefully closed with absorbable suture followed by suturing of supraspinatus with non-absorbable suture. Our initial plan to fix the acromial fracture to spinous process of scapula with 2 4 mm cannulated cancellous screw placed orthogonal to fracture site was modified intraoperative due to screw cut out and we went ahead with TBW with 1 screw and 1 Kirschner wire to prevent further fragmentation of the fragment. Wound was healing and healthy. Patient was started on a passive pendular exercises after 4 weeks and active exercises at 6 weeks. Six months postoperatively patient had complete range of shoulder rotation with forward flexion of 80° and abduction possible till 45°. Patient was able to do most of his activities of daily living barring overhead activities.
Conclusion: As there are very limited cases of this sort of injury, this case report will cast a light on management options and outcomes of such injuries. We received fair results in our study with good healing and painless functional shoulder joint. However, long term and multi centric studies are required for further information pertaining to such scenarios.
Keywords: Open acromial fracture, open supraspinatus tear, tension band wiring.
Scapular fractures comprise <1% of all fractures with acromion fractures being only 8–9% of these [1,2,3]. Open fractures of acromion are usually seen in direct trauma with sharp object based on the all the case reports available on this topic [4,5]. These often occur in conjugation with other injuries to the shoulder girdle [6]. The degree of soft tissue injury and site of fracture largely depends on site of trauma and force applied. Such open fractures are extremely rare owing to their location. This case report aims at studying the management of open displaced acromial fracture with rotator cuff injury in a young gentleman, all the hurdles we faced during management and the outcome of patient at 3 months.
A 21-year-old male, student, right-handed, without any medical or surgical history presented to the emergency department after a 3-day old direct trauma injury with sharp heavy object to his right shoulder. He was conscious, alert, oriented, and complaining of right shoulder pain and inability to move this arm. On examination, there was a sharply incised wound around 15 cm in length on the superior aspect of the right shoulder extending to the glenohumeral joint in its depth, with the glenohumeral articulation clearly visible (Fig. 1). 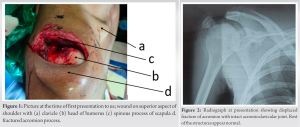 The acromion was sharply cleaved into two parts along its anteroposterior axis with incisional injury of supraspinatus and capsule. The wound was minimally contaminated. There was no active bleeding at presentation. There was no associated vascular or neurological injury. Passive and active range of movement of shoulder were painful and limited. Radiographs suggested a two-part displaced fracture of the acromion (type III Kuhn classification) with rest of the osseous structures appearing normal (Fig. 2). An magnetic resonance imaging (MRI) scan (which patient had already done prior to reporting to our hospital) confirmed a displaced fracture of acromion process of scapula, complete tear of supraspinatus at its musculotendinous junction (Fig. 3).
The acromion was sharply cleaved into two parts along its anteroposterior axis with incisional injury of supraspinatus and capsule. The wound was minimally contaminated. There was no active bleeding at presentation. There was no associated vascular or neurological injury. Passive and active range of movement of shoulder were painful and limited. Radiographs suggested a two-part displaced fracture of the acromion (type III Kuhn classification) with rest of the osseous structures appearing normal (Fig. 2). An magnetic resonance imaging (MRI) scan (which patient had already done prior to reporting to our hospital) confirmed a displaced fracture of acromion process of scapula, complete tear of supraspinatus at its musculotendinous junction (Fig. 3).  A linear sagittal unicortical fracture of the humeral head was also reported in the MRI images. In the emergency department, broad spectrum antibiotics, tetanus toxoid and analgesics were administered. Wash with pulsatile irrigation was given and patient was operated after 6 hours of arrival to the hospital. Regional anaesthesia with supraclavicular and axillary block was given and patient was placed in supine position with affected side elevated. Wound was thoroughly irrigated. Approach to the structures was through the wound itself. Capsule of shoulder was carefully closed with absorbable sutures followed by suturing of supraspinatus with non-absorbable suture by double row stitch technique (Fig. 4). Our initial plan was to fix the acromial fracture with 2 partially threaded 4 mm cannulated cancellous screws placed orthogonal to fracture site. However intraoperative there was 1 screw cut out through the superior cortex of acromion. We modified our plan and went ahead with tension band wiring (TBW) with 1 screw and 1 Kirschner wire to prevent further fragmentation of the fragment (Fig. 5). Post fixation the intraoperative shoulder mobilization revealed a stable fixation. The subcutaneous layers and skin closure was done as per the standard protocol. A radiograph was performed postoperatively (Fig. 6).
A linear sagittal unicortical fracture of the humeral head was also reported in the MRI images. In the emergency department, broad spectrum antibiotics, tetanus toxoid and analgesics were administered. Wash with pulsatile irrigation was given and patient was operated after 6 hours of arrival to the hospital. Regional anaesthesia with supraclavicular and axillary block was given and patient was placed in supine position with affected side elevated. Wound was thoroughly irrigated. Approach to the structures was through the wound itself. Capsule of shoulder was carefully closed with absorbable sutures followed by suturing of supraspinatus with non-absorbable suture by double row stitch technique (Fig. 4). Our initial plan was to fix the acromial fracture with 2 partially threaded 4 mm cannulated cancellous screws placed orthogonal to fracture site. However intraoperative there was 1 screw cut out through the superior cortex of acromion. We modified our plan and went ahead with tension band wiring (TBW) with 1 screw and 1 Kirschner wire to prevent further fragmentation of the fragment (Fig. 5). Post fixation the intraoperative shoulder mobilization revealed a stable fixation. The subcutaneous layers and skin closure was done as per the standard protocol. A radiograph was performed postoperatively (Fig. 6). 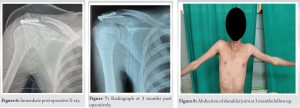 Patient completed his antibiotic course for 72 h and the shoulder was immobilized in abduction with an arm sling for 2 weeks. At the 2-week follow-up, patient came for suture removal. Wound was healing and healthy. Patient was started on a stepwise rehabilitation program with passive pendular exercises after 4 weeks and active exercises at 6 weeks. Three months postoperatively X-ray showed a uniting fracture (Fig. 7). Patient had complete internal and external rotation. However, forward flexion was limited to 80° with abduction possible till 45° (Figs. 8-11).
Patient completed his antibiotic course for 72 h and the shoulder was immobilized in abduction with an arm sling for 2 weeks. At the 2-week follow-up, patient came for suture removal. Wound was healing and healthy. Patient was started on a stepwise rehabilitation program with passive pendular exercises after 4 weeks and active exercises at 6 weeks. Three months postoperatively X-ray showed a uniting fracture (Fig. 7). Patient had complete internal and external rotation. However, forward flexion was limited to 80° with abduction possible till 45° (Figs. 8-11). However patient had no pain at all in his shoulder joint was able to carry out his daily activities with minimal discomfort. His Penn Shoulder Score at 3 months was 53.3%. The wound had healed well (Fig. 12).
However patient had no pain at all in his shoulder joint was able to carry out his daily activities with minimal discomfort. His Penn Shoulder Score at 3 months was 53.3%. The wound had healed well (Fig. 12).
The majority acromion fractures are managed non-operatively with success. However significant shoulder disability has been found in patients with displaced acromion fracture and should be operated, especially when they occur with a concurrent injury around the shoulder gridle [7,8]. Kuhn et al. [9] has classified acromial injury to help determine operative or non-operative management. Our fracture was type 3 with narrowing of subacromial space and required surgical management for fracture as well as debridement for wound and joint lavage. Wound was managed according to ideal principles of open fracture management that is pulsatile irrigation and good antibiotic coverage with 1st generation cephalosporins and aminoglycosides with metronidazole [10]. As per limited literature acromial fracture could be fixed with TBW, reconstruction plate, Kirschner wire, screw [7]. However as it was on open fracture we opted for minimal implantation and plate fixation was avoided. Our aim was to provide a stable reduction with prevention of infection and eventually stable, painless, mobile shoulder joint in this young male. At present even though our patient has limitation of forward flexion and abduction, he can perform most of his activities of daily living and thus this management can be considered for managing similar patients.
There is no case series or study showing evidence-based management options and possible complications of management of open acromial fractures. We reviewed similar case reports and found only two similar case reports. Such a complex injury is truly rare and it is important to plan the management adequately to ensure proper outcome for the patient. Adequate debridement and primary repair of supraspinatus tendon with TBW of the acromion is indeed a viable option for such cases. Other such case reports and series should be reported when available to show other possible conditions associated with this fracture entity. Long term and multi centric studies are required for further information pertaining to such scenarios.
Such open fractures of the acromion where the shoulder joint is exposed can be daunting to treat with the risk of infection and non-union being at the back of mind of any orthopaedic surgeon. But with proper planning and management of such injuries one can easily overcome these challenges and primary management can be easily achieved. Such rare cases should be reported more often in literature so that one can come to a consensus as to what the best line of management of the patient will be, leading to a satisfied surgeon and patient.
References
- 1.Noort AV. Scapular fractures. In: Rockwood CA, Green DP, Bucholz RW, editors. Rockwood and Green’s Fractures in Adults. 9th ed. Philadelphia, PA, USA: Wolters Kluwer Health, Lippincott Williams and Wilkins; 2020. p. 1144-64. [Google Scholar | PubMed]
- 2.McGahan JP, Rab GT, Dublin A. Fractures of the scapula. J Trauma 1980;20:880-3. [Google Scholar | PubMed]
- 3.Wilber MC, Evans EB. Fractures of the scapula. An analysis of forty cases and a review of the literature. J Bone Joint Surg 1977;59:358-62. [Google Scholar | PubMed]
- 4.Alawad MO, Alharthi S, Mahmoud J, Alanazi B, Surur S. Open fracture of the acromion: An isolated injury with oblique-type fracture. Case Rep Orthop 2018;2018:2107059. [Google Scholar | PubMed]
- 5.Lim MJ, Vegneeshswaran N, Kamalruzaman MA. Open fracture of acromion; management with open reduction and tension band wiring: A case report. Malays Orthop J 2023;In Print. [Google Scholar | PubMed]
- 6.Goss TP. The scapula: Coracoid, acromial, and avulsion fractures. Am J Orthop (Belle Mead NJ) 1996;25:106-15. [Google Scholar | PubMed]
- 7.Dukan R, Abboud J, Ouchrif Y. Isolated acromial fracture in a cyclist: A case report and review of the literature. JBJS Case Connect 2020;10:e2000079. [Google Scholar | PubMed]
- 8.Hess F, Zettl R, Welter J, Smolen D, Knoth C. The traumatic acromion fracture: Review of the literature, clinical examples and proposal of a treatment algorithm. Arch Orthop Trauma Surg 2019;139:651-8. [Google Scholar | PubMed]
- 9.Kuhn JE, Blaiser RB, Carpenter JE. Fractures of the acromion process: A proposed classification system. J Orthop Trauma 1994;8:6-13. [Google Scholar | PubMed]
- 10.Halawi MJ, Morwood MP. Acute management of open fractures: An evidence-based review. Orthopedics 2015;38:e1025-33. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 First Documented Hip Replacement in a Palestinian Patient with Ochronotic Alkaptonuria Arthropathy: A Case Report
March 1, 2025 First Documented Hip Replacement in a Palestinian Patient with Ochronotic Alkaptonuria Arthropathy: A Case Report May 10, 2023 Post-Traumatic Large Segmental Bone Loss – Does Bone Transport Obviate the Need for Successful Soft-Tissue Cover – A Case Report
May 10, 2023 Post-Traumatic Large Segmental Bone Loss – Does Bone Transport Obviate the Need for Successful Soft-Tissue Cover – A Case Report January 6, 2014 Acute Metallosis Following Total Knee Replacement − A Case Report
January 6, 2014 Acute Metallosis Following Total Knee Replacement − A Case Report March 1, 2025 Surgical Management Protocol of Hawkins Type 3 Comminuted Fracture Neck of Talus: Case Series
March 1, 2025 Surgical Management Protocol of Hawkins Type 3 Comminuted Fracture Neck of Talus: Case Series