
Isolated plantar plate rupture should be suspected as a differential diagnosis in patients with great toe injury.
Dr. Yasunari Ikuta, Department of Orthopaedic Surgery, Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima, Japan. E-mail: yikuta@hiroshima-u.ac.jp
Abstract
Introduction: Injuries of the great toe are common sports-related injuries; however, isolated traumatic plantar plate tears at the interphalangeal (IP) joint are relatively rare. Here, we present a pediatric case of a chronic plantar plate tear of the IP joint of the great toe that was difficult to diagnose definitively, which delayed surgical treatment.
Case Report: An 11-year-old girl was injured when she collided with her right great toe while using a jump box during gymnastics. She felt pain in her great toe that progressively worsened despite conservative treatment at an initial clinic, and she experienced hyperextension of the IP joint. She was referred to our outpatient clinic because of diagnostic difficulty and increased symptoms, such as pain and swelling of the plantar side of her right great toe. Physical examination revealed swelling and tenderness on the plantar aspect of the IP joint and the impossibility of active flexion of the IP joint. The passive range of motion was 35° during extension. Ultrasonography revealed a low-echoic area on the plantar plate on the phalangeal side. Thus, we diagnosed the patient with a chronic plantar plate tear of the IP joint of the right great toe and performed surgical treatment 8 months after its onset. The plantar plate ruptured at the insertion of the proximal phalanx; however, the insertion of the distal phalanx remained intact. The plantar plate was repaired using suture anchors, and excellent short-term postoperative results were obtained at the 1-year follow-up.
Conclusion: Isolated plantar plate rupture is difficult to diagnose definitively in the acute phase because of the lack of specific findings on physical and radiographic examinations. Plantar plate rupture should be suspected as a differential diagnosis in patients with great toe injuries due to axial load and hyperextension forces. Plantar plate repair using suture anchors may be a useful option for treating plantar plate tears of the IP joint of the great toe when its insertion into the distal phalanx is preserved, even during the chronic phase.
Keywords: Plantar plate tear, dislocation, interphalangeal joint, suture anchor, chronic phase.
Great toe injuries are common sports-related injuries in every age group and level of participation [1]. Regarding the interphalangeal (IP) joint, irreducible cases of dorsal dislocation of the great toe could present clinical problems because of the need for open reduction [2]. Although a plantar plate injury at the first metatarsophalangeal joint, turf toe, is a common foot injury in athletes [3,4], the isolated plantar plate tear at the IP joint is a relatively rare condition in the clinical context. Here, we present a pediatric case of a chronic plantar plate tear of the IP joint of the great toe that was difficult to diagnose definitively, which delayed surgical treatment. Excellent clinical results have been obtained with plantar plate repair using suture anchors, even during the chronic phase.
An 11-year-old girl was injured when she collided with her right great toe while using a jump box during gymnastics. She then started to feel pain in the right great toe and had difficulty wearing shoes. Five months later, the pain progressively worsened, and she experienced hyperextension of the IP joint. No specific diagnoses were made at an initial clinic. She was referred to our outpatient clinic because of diagnostic difficulty and increased symptoms, such as pain and swelling of the plantar side of her right great toe, despite conservative treatment. Physical examination at the initial visit revealed the impossibility of active flexion, swelling, and tenderness in the plantar aspect of the IP joint of the right great toe. The passive range of motion was 35° during extension (Fig. 1).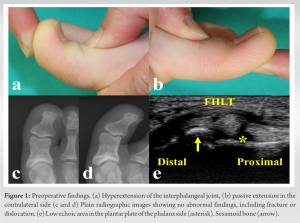 The score on the Japanese society for surgery of the foot (JSSF) hallux metatarsophalangeal-IP scale [5] was 58 points. Plain radiographs showed no obvious abnormal findings such as dislocation or fracture (Fig. 1). Ultrasonography revealed a low-echoic area on the plantar plate on the phalangeal side (Fig. 1). Moreover, there was no evidence of flexor hallucis longus (FHL) tendon rupture. Therefore, we diagnosed the patient with a chronic plantar plate tear of the IP joint of the right great toe and performed surgical treatment under general anesthesia 8 months after its onset. Intraoperatively, a plantar incision was made on the IP joint, and the FHL tendon was retracted. The plantar plate ruptured at the insertion of the proximal phalanx; however, the insertion of the distal phalanx remained intact (Fig. 2).
The score on the Japanese society for surgery of the foot (JSSF) hallux metatarsophalangeal-IP scale [5] was 58 points. Plain radiographs showed no obvious abnormal findings such as dislocation or fracture (Fig. 1). Ultrasonography revealed a low-echoic area on the plantar plate on the phalangeal side (Fig. 1). Moreover, there was no evidence of flexor hallucis longus (FHL) tendon rupture. Therefore, we diagnosed the patient with a chronic plantar plate tear of the IP joint of the right great toe and performed surgical treatment under general anesthesia 8 months after its onset. Intraoperatively, a plantar incision was made on the IP joint, and the FHL tendon was retracted. The plantar plate ruptured at the insertion of the proximal phalanx; however, the insertion of the distal phalanx remained intact (Fig. 2). 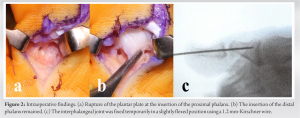 The distal phalanx is easily dislocated manually in the dorsal and plantar directions. The IP joint was temporarily fixed in a slightly flexed position using a 1.2 mm-Kirschner wire (Fig. 2). Two guide pins were inserted from the plantar aspect of the distal part of the proximal phalanx to the dorsal aspect of the base of the proximal phalanx under an image intensifier (Fig. 3), and two suture anchors were inserted (FiberTak DX Suture Anchor, Arthrex, Naples, FL, JuggerKnot Mini, Zimmer Biomet, Warsaw, IN).
The distal phalanx is easily dislocated manually in the dorsal and plantar directions. The IP joint was temporarily fixed in a slightly flexed position using a 1.2 mm-Kirschner wire (Fig. 2). Two guide pins were inserted from the plantar aspect of the distal part of the proximal phalanx to the dorsal aspect of the base of the proximal phalanx under an image intensifier (Fig. 3), and two suture anchors were inserted (FiberTak DX Suture Anchor, Arthrex, Naples, FL, JuggerKnot Mini, Zimmer Biomet, Warsaw, IN). The plantar plate was repaired by suturing using horizontal mattress stitches (Fig. 3). Postoperative treatment consisted of 1 week of non-weight-bearing, and the Kirschner wire was removed 4 weeks postoperatively, after which range-of-motion exercises were started. The patient was allowed to return to sports 3 months postoperatively. At 1 year follow-up, there was no hyperextension or instability of the IP joint of the great toe, no degenerative changes on plain radiographic images (Fig. 4), and excellent clinical outcomes with a score of 100 on the JSSF hallux scale.
The plantar plate was repaired by suturing using horizontal mattress stitches (Fig. 3). Postoperative treatment consisted of 1 week of non-weight-bearing, and the Kirschner wire was removed 4 weeks postoperatively, after which range-of-motion exercises were started. The patient was allowed to return to sports 3 months postoperatively. At 1 year follow-up, there was no hyperextension or instability of the IP joint of the great toe, no degenerative changes on plain radiographic images (Fig. 4), and excellent clinical outcomes with a score of 100 on the JSSF hallux scale. The Self-Administered Foot Evaluation Questionnaire [6] demonstrated the all subscales of 100 for pain and pain-related symptoms, physical function and daily living, social function, shoe-related issues, and general health and well-being.
The Self-Administered Foot Evaluation Questionnaire [6] demonstrated the all subscales of 100 for pain and pain-related symptoms, physical function and daily living, social function, shoe-related issues, and general health and well-being.
Isolated plantar plate rupture is difficult to diagnose definitively in the acute phase because of the lack of specific findings on physical and radiographic examinations. Repairing the plantar plate using suture anchors could be a useful option for isolated plantar plate tears, regardless of the chronic phase, when its insertion into the distal phalanx is preserved because of excellent short-term postoperative results. Several components contribute to the stability of the IP joint of the great toe, including the flexor and extensor hallucis longus tendons, collateral ligaments, capsule, and plantar plate [7]. The plantar plate is a thick, fibrocartilaginous pad formed by the condensation of the collateral and capsular ligaments [8], and the plantar plate of the IP joint is inserted proximally to the condyle of the proximal phalanx and distally to the condyle of the base of the distal phalanx [9]. The plantar plate prevents hyperextension of the IP joint as a static stabilizer [7]. Injury to the IP joint is usually caused by an axial load applied at the terminal end of the digit [10], and the mechanism of injury that causes dislocation of the IP joint of the great toe is an axial load with a hyperextension force [7]. A cadaveric study described that the IP joint could be dislocated by cutting the connection between the plantar plate and proximal phalanx. Insertion into the distal phalangeal base was preserved, and the plantar plate could not be displaced into the IP joint space. When the plantar plate was further ruptured at its attachment to the base of the distal phalanx, it could move into the joint space [2]. In such a state, partial spontaneous reduction with interposition of the plantar plate or sesamoid causes subtle widening of the joint on radiography [10]. In the present case, the plantar plate ruptured at the insertion of the proximal phalanx; however, preserved attachment to the distal phalanx was confirmed intraoperatively. Thus, the dorsal dislocation of the IP joint that occurred at the time of injury was repositioned spontaneously because the plantar plate and sesamoid could not be moved into the IP joint space. Subsequently, persistent pain and instability of the IP joint of the great toe were caused by the rupture of the plantar plate. Importantly, plantar plate tears of the IP joint of the great toe should be considered as a differential diagnosis in toe injury, especially in patients who experience characteristic injury mechanisms and sustain great toe pain with hyperextension of the IP joint. Intraoperatively, the direction of the anchor guide pin should be confirmed under fluoroscopy for safe placement of the anchors into the proximal phalanx. The use of small suture anchors is suitable for pediatric patients with small bone structures.
Plantar plate repair using suture anchors may be a promising option for treating chronic plantar plate tears of the IP joint of the great toe when its insertion into the distal phalanx is preserved.
Plantar plate rupture should be suspected as a differential diagnosis in patients with great toe injury caused by an axial load and a hyperextension force, who experience pain on the plantar side of the great toe and hyperextension of the IP joint.
References
- 1.York PJ, Wydra FB, Hunt KJ. Injuries to the great toe. Curr Rev Musculoskelet Med 2017;10:104-12. [Google Scholar | PubMed]
- 2.Miki T, Yamamuro T, Kitai T. An irreducible dislocation of the great toe. Report of two cases and review of the literature. Clin Orthop Relat Res 1988;230:200-6. [Google Scholar | PubMed]
- 3.Poppe T, Reinhardt D, Tarakemeh A, Vopat BG, Mulcahey MK. Turf toe: Presentation, diagnosis, and management. JBJS Rev 2019;7:e7. [Google Scholar | PubMed]
- 4.Seow D, Tengku Yusof TN, Yasui Y, Shimozono Y, Kennedy JG. Treatment options for turf toe: A systematic review. J Foot Ankle Surg 2020;59:112-6. [Google Scholar | PubMed]
- 5.Niki H, Aoki H, Inokuchi S, Ozeki S, Kinoshita M, Kura H, et al. Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders I: Development of standard rating system. J Orthop Sci 2005;10:457-65. [Google Scholar | PubMed]
- 6.Niki H, Aoki H, Inokuchi S, Ozeki S, Kinoshita M, Kura H, et al. Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders I: Development of standard rating system. J Orthop Sci 2005;10:457-65. [Google Scholar | PubMed]
- 7.Crosby LA, McClellan JW 3rd, Prochaska VJ. Irreducible dorsal dislocation of the great toe interphalangeal joint: Case report and literature review. Foot Ankle Int 1995;16:559-61. [Google Scholar | PubMed]
- 8.Davies MB, Dalal S. Gross anatomy of the interphalangeal joint of the great toe: Implications for excision of plantar capsular accessory ossicles. Clin Anat 2005;18:239-44. [Google Scholar | PubMed]
- 9.Moroni S, Márquez J, Fernández-Gibello A, Nieves GC, Montes R, Vázquez T, et al. The hallucal interphalangeal ossicle: Anatomy and basis for ultrasound-guided surgical shaving. Sci Rep 2022;12:4789. [Google Scholar | PubMed]
- 10.Reid JJ, Early JS. Injuries to the toes. In: Bucholz RW, Heckman JD, Court-Brown CM, Tornetta P, editors. Rockwood and Green’s Fractures in Adults. Philadelphia, PA: Lippincott Williams and Wilkins; 2010. p. 2162-9. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Complex Irreducible Dislocation of the Fourth Toe Proximal Interphalangeal Joint in a 5-year-old Boy Fixed by Soft Anchor: A Case Report
August 1, 2026 Complex Irreducible Dislocation of the Fourth Toe Proximal Interphalangeal Joint in a 5-year-old Boy Fixed by Soft Anchor: A Case Report November 1, 2025 Irreducible Dislocation of the Great Toe Interphalangeal Joint Secondary to an Incarcerated Sesamoid: A Retrospective Case Series of Six Patients
November 1, 2025 Irreducible Dislocation of the Great Toe Interphalangeal Joint Secondary to an Incarcerated Sesamoid: A Retrospective Case Series of Six Patients April 1, 2025 Severe Type 1 Thumb Boutonniere Deformity with Interphalangeal Joint Dislocation in a Young Patient: A Case Report
April 1, 2025 Severe Type 1 Thumb Boutonniere Deformity with Interphalangeal Joint Dislocation in a Young Patient: A Case Report August 1, 2026 Medial Subtalar Joint Dislocation in an 18-Year-Old Athlete with Pes Planus: Beyond A Simple Misstep
August 1, 2026 Medial Subtalar Joint Dislocation in an 18-Year-Old Athlete with Pes Planus: Beyond A Simple Misstep