
Management of plateau injuries with concaminant PCL injury.
Dr. Michael Booth, Department of Orthopedics, West Virginia University, Morgantown, West Virginia. E-mail: michael.booth1@hsc.wvu.edu
Abstract
Introduction: Posterior cruciate ligament (PCL) injuries and tibial plateau fractures are common orthopedic injuries. In the pediatric population, femoral-sided avulsions are the most common injury pattern for PCL injuries. However, there is limited literature on the characterization and treatment of pediatric PCL avulsion with concomitant tibial plateau fracture.
Case Report: We present the case of an adolescent female who was involved in an all-terrain vehicle rollover. The patient sustained a femoral-sided PCL avulsion injury with an associated lateral tibial plateau fracture. The PCL avulsion was treated through arthroscopic cruciate repair, while the tibial plateau fracture was managed with open reduction and internal fixation (ORIF).
Conclusion: This case report highlights a rare combination of a femoral-sided PCL avulsion and lateral tibial plateau fracture in a pediatric patient. The treatment involved arthroscopic cruciate repair for the PCL avulsion and ORIF for the tibial plateau fracture. Further studies are needed to establish optimal management strategies for similar cases.
Keywords: Posterior cruciate ligament, PCL avulsion, tibial plateau fracture, pediatric, arthroscopic cruciate repair, open reduction and internal fixation.
Pediatric posterior cruciate ligament (PCL) injuries are relatively uncommon. The prevailing literature indicates that when PCL injuries occur in the pediatric population, they most commonly manifest as avulsion fractures rather than mid-substance tears. Specifically, femoral-side avulsions are the prevailing injury pattern, whereas tibial-side avulsions are rarely reported. This differs from the adult population, where tibial-side avulsions are more prevalent. Non-operative management has been successful in cases of avulsion fractures with minimal displacement or partial ligament tears [1,2]. However, various fixation methods have been described and the debate regarding the outcomes of open versus arthroscopic approaches remains ongoing, with arthroscopic repair being more prevalent in the literature. Notably, Pisanu and Ross have reported satisfactory outcomes with arthroscopic repairs of femoral-side avulsions [3]. PCL injuries rarely occur in isolation and are often accompanied by additional ligamentous injuries in the knee. In a comprehensive review of 222 acute knee hemarthroses, only three cases involved isolated PCL injuries. Multi-ligamentous knee injuries involving the PCL are well-documented; however, reports of PCL injuries in conjunction with tibial plateau fractures are scarce [4]. Abdel-Hamid performed diagnostic arthroscopies on 98 tibial plateau fractures and identified peripheral meniscus tears and ACL avulsions as the most associated injuries [5]. To the best of our knowledge, there are no reports in the literature describing the treatment of PCL injuries occurring concurrently with tibial plateau fractures in the pediatric population.
A healthy 14-year-old female presented to our emergency department (ED) with severe left knee pain and swelling following an all-terrain vehicle rollover crash. On evaluation, the ED assessment revealed a large left knee effusion and limited range of motion due to pain. Radiographic imaging, including plain films and subsequent computerized tomography (CT) scans, revealed a left lateral tibial plateau fracture with a split depression type fracture pattern (Fig. 1). Additional imaging with CT and magnetic resonance imaging (MRI) identified a bony fragment within the femoral notch adjacent to the origin of the PCL on the femur (Fig. 2).
Additional imaging with CT and magnetic resonance imaging (MRI) identified a bony fragment within the femoral notch adjacent to the origin of the PCL on the femur (Fig. 2).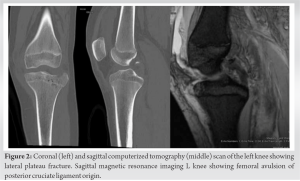 The non-contrast MRI study confirmed a suspected PCL avulsion from the femoral origin with an intact tibial insertion (Fig. 3).
The non-contrast MRI study confirmed a suspected PCL avulsion from the femoral origin with an intact tibial insertion (Fig. 3). 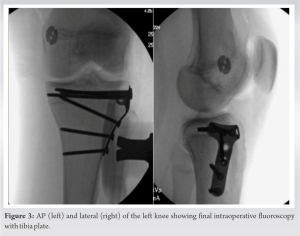 Evaluation of the anterior cruciate ligament (ACL) and menisci showed no apparent damage, while partial tears of the medial and lateral collateral ligaments and bony edema in the lateral femoral condyle were observed. To manage the injury, the patient was placed in a hinged knee brace locked in extension and made non-weight-bearing on the injured extremity. Considering the degree of PCL displacement and depression at the tibial articular surface, a delayed surgery was recommended to allow for swelling reduction. One week after the initial injury, the patient underwent surgery. A posterior drawer maneuver under anesthesia confirmed a Grade 1 PCL injury and diagnostic arthroscopy revealed detachment of the PCL from its anatomic location at the distal femur. The PCL avulsion was repaired using #2 FiberWire (Arthrex) through the PCL stump, with the free end passed through the PCL origin footprint and anchored to the medial distal femur cortex using a 14 mm suture button. The final position of the PCL was confirmed to be anatomical and stable. An anterolateral incision was made at the proximal left leg, followed by a sub-meniscal arthrotomy to visualize the articular surface of the proximal tibia. The fractured tibial plateau was restored to anatomic position and crushed cancellous allograft chips were used to augment the traumatic defect. A 4-hole T-plate (Synthes) was contoured to accommodate the patient’s proximal anterolateral tibia and secured with cortical screws to stabilize the articular fragments (Fig. 3). Postoperatively, the patient remained non-weight-bearing with crutches and a hinged knee brace locked in extension. Progressive weight-bearing and rehabilitation exercises were initiated in the following weeks, leading to satisfactory bony healing and functional recovery. At the 2-year follow-up, the patient reported a successful return to varsity high school soccer without any pain or instability in the left knee. Radiographs and physical examination revealed a normal joint with symmetrical strength and range of motion compared to the contralateral knee. The patient had completed a formal physical therapy program and had been released to full activity and athletic play without restrictions. The patient was asymptomatic with the tibia plate and there is no plan for removal unless she becomes symptomatic.
Evaluation of the anterior cruciate ligament (ACL) and menisci showed no apparent damage, while partial tears of the medial and lateral collateral ligaments and bony edema in the lateral femoral condyle were observed. To manage the injury, the patient was placed in a hinged knee brace locked in extension and made non-weight-bearing on the injured extremity. Considering the degree of PCL displacement and depression at the tibial articular surface, a delayed surgery was recommended to allow for swelling reduction. One week after the initial injury, the patient underwent surgery. A posterior drawer maneuver under anesthesia confirmed a Grade 1 PCL injury and diagnostic arthroscopy revealed detachment of the PCL from its anatomic location at the distal femur. The PCL avulsion was repaired using #2 FiberWire (Arthrex) through the PCL stump, with the free end passed through the PCL origin footprint and anchored to the medial distal femur cortex using a 14 mm suture button. The final position of the PCL was confirmed to be anatomical and stable. An anterolateral incision was made at the proximal left leg, followed by a sub-meniscal arthrotomy to visualize the articular surface of the proximal tibia. The fractured tibial plateau was restored to anatomic position and crushed cancellous allograft chips were used to augment the traumatic defect. A 4-hole T-plate (Synthes) was contoured to accommodate the patient’s proximal anterolateral tibia and secured with cortical screws to stabilize the articular fragments (Fig. 3). Postoperatively, the patient remained non-weight-bearing with crutches and a hinged knee brace locked in extension. Progressive weight-bearing and rehabilitation exercises were initiated in the following weeks, leading to satisfactory bony healing and functional recovery. At the 2-year follow-up, the patient reported a successful return to varsity high school soccer without any pain or instability in the left knee. Radiographs and physical examination revealed a normal joint with symmetrical strength and range of motion compared to the contralateral knee. The patient had completed a formal physical therapy program and had been released to full activity and athletic play without restrictions. The patient was asymptomatic with the tibia plate and there is no plan for removal unless she becomes symptomatic.
This case represents a unique presentation of a PCL avulsion with a lateral plateau fracture in a pediatric patient. The literature provides some guidance on the management of similar PCL avulsion injuries, with successful outcomes reported in various surgical techniques. A case series by Pandya et al. described two pediatric PCL avulsion injuries treated with open reduction and internal fixation (ORIF) using different fixation methods, demonstrating successful outcomes [6]. Solayar also reported a case of open repair with fixation using a cancellous screw [7]. Another case report by Kwon described arthroscopic repair of a pediatric PCL tibial avulsion using a pull-out suture technique [8]. These cases demonstrate the feasibility of surgical repair in achieving positive outcomes and allowing for a return to sports activities. Reconstruction techniques using Achilles and hamstring grafts have also been described in the literature by Bovid and Sorenson, respectively. However, it is important to note that these techniques were primarily used for intrasubstance tears rather than avulsion injuries [9,10]. A direct comparison between repair and reconstruction procedures for PCL injuries is currently lacking in the literature. To the best of our knowledge, this is the first reported case discussing a femoral-sided PCL avulsion associated with a lateral tibial plateau fracture and subsequent operative treatment. In our patient, we opted for cruciate repair instead of reconstruction due to the intact visualization of the PCL during arthroscopy. However, reconstruction has been described as a viable option for femoral-sided avulsions [11]. For the lateral tibial plateau fracture, we chose a standard ORIF with a plate and screw construct, which has also been recommended in the pediatric population. The rehabilitation protocol was tailored to address the unique combination of bony and ligamentous injuries in this patient. Overall, our patient achieved an excellent outcome following intervention for this rare knee injury. Further studies and case reports are warranted to establish optimal treatment strategies and compare the outcomes of repair versus reconstruction in pediatric PCL avulsion injuries.
This case report provides valuable insights into the successful surgical management of a rare combination of PCL avulsion and lateral tibial plateau fracture in a pediatric patient.
This case highlights the importance of considering the possibility of combined injuries, such as PCL avulsion and lateral tibial plateau fracture, in pediatric patients presenting with knee trauma. Prompt diagnosis, thorough imaging evaluation, and a multidisciplinary approach involving orthopedic surgeons, physiotherapists, and radiologists are essential for accurate assessment and optimal treatment planning. Clinicians should be aware of various surgical options available, including avulsion repair and ORIF, tailored to the specific injury pattern, to achieve successful outcomes and facilitate the patient’s return to normal function.
References
- 1.Kocher MS, Shore B, Nasreddine AY, Heyworth BE. Treatment of posterior cruciate ligament injuries in pediatric and adolescent patients. J Pediatr Orthop 2012;32:553-60. [Google Scholar | PubMed]
- 2.Katsman A, Strauss EJ, Campbell KA, Alaia MJ. Posterior cruciate ligament avulsion fractures. Curr Rev Musculoskelet Med 2018;11:503-9. [Google Scholar | PubMed]
- 3.Pisanu G, Moura JL, Saithna A, Sonnery-Cottet B. Arthroscopic repair of proximal posterior cruciate ligament injuries in pediatric patients. Arthrosc Tech 2019;8:e691-5. [Google Scholar | PubMed]
- 4.Fanelli GC, Edson CJ. Posterior cruciate ligament injuries in trauma patients: Part II. Arthroscopy 1995;11:526-9. [Google Scholar | PubMed]
- 5.Abdel-Hamid MZ, Chang CH, Chan YS, Lo YP, Huang JW, Hsu KY, et al. Arthroscopic evaluation of soft tissue injuries in tibial plateau fractures: Retrospective analysis of 98 cases. Arthroscopy 2006;22:669-75. [Google Scholar | PubMed]
- 6.Pandya NK, Janik L, Chan G, Wells L. Case reports: Pediatric PCL insufficiency from tibial insertion osteochondral avulsions. Clin Orthop Relat Res 2008;466:2878-83. [Google Scholar | PubMed]
- 7.Solayar GN, Kapoor H. PCL tibial avulsion with an associated medial meniscal tear in a child: A case report on diagnosis and management. J Pediatr Orthop B 2012;21:356-8. [Google Scholar | PubMed]
- 8.Kwon OS, Park MJ, Kelly JD 4th. Arthroscopic treatment of a PCL avulsion fracture in a skeletally immature patient. Orthopedics 2011;34:137. [Google Scholar | PubMed]
- 9.Bovid KM, Salata MJ, Vander Have KL, Sekiya JK. Arthroscopic posterior cruciate ligament reconstruction in a skeletally immature patient: A new technique with case report. Arthroscopy 2010;26:563-70.1. [Google Scholar | PubMed]
- 10.Sørensen OG, Faunø P, Christiansen SE, Lind M. Posterior cruciate ligament reconstruction in skeletal immature children. Knee Surg Sports Traumatol Arthrosc 2017;25:3901-5. [Google Scholar | PubMed]
- 11.Zionts LE. Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345-55. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report
August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report
August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series
August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature
July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature