
The diagnosis of knee pain is delayed in cases with no soft-tissue mass, magnetic resonance imaging is the gold standard for diagnosis, and surgeons should not discharge patients with sciatic nerve schwannoma from routine follow-up to avoid the risk of missed recurrence.
Dr. Collen Sandile Nkosi, Department of Orthopaedic Surgery, Chris Hani Baragwanath Academic Hospital, 26 Chris Hani Rd, Diepkloof 319-Iq, Johannesburg, 1864, South Africa. E-mail: drcsnkosi@gmail.com
Abstract
Introduction: Schwannomas are rare benign tumors of the nerve sheath that originate from the Schwann cells of the peripheral nerve and have a broad anatomic distribution that includes superficial tissues, deep tissues, including the central nervous system, and the gastrointestinal system.
Case Report: A 60-year-old male presented with left knee pain for 5 years. This pain was associated with paresthesia, night pain unresponsive to analgesia, on the left foot intermittent pins and needles sensation. Schwannoma lesion was excised, histology confirmed the diagnosis, and the patient’s symptoms improved.
Conclusion: Schwannoma around the knee is a rare or atypical cause of the non-arthritic pain and should be considered in the differential diagnosis of non-arthritic and extra-articular causes of knee pain with neurological deficit of the foot in an adult population.
Keywords: Schwannoma, sciatic nerve, knee pain, benign tumor.
Schwannomas are benign tumors of the nerve sheath that originate from the Schwann cells of the peripheral nerve and have a broad anatomic distribution that includes superficial tissues (skin and subcutaneous areas), deep tissues, including the central nervous system, and the gastrointestinal system [1,2]. They are isolated, solitary, well-circumscribed, and well-capsulated tumors and are rarely in the plexiform [1,3]. Lower limb benign schwannoma of the sciatic nerve accounts for <1% of all schwannomas [2,4]. These tumors usually present between the 3rd and 5th decades of life [5]. Clinical presentation is non-specific, which leads to delays in diagnosis and treatment [6]. The purpose of this case study and literature review is to highlight the non-arthritic and extra-articular causes of knee pain in an adult population that required excision for the resolution of symptoms.
A 60-year-old male presented with left knee pain for 5 years. This pain was accompanied by numbness, nighttime pain that was unresponsive to analgesia, and intermittent pins and needles on the left foot. He reports having had left knee negative arthroscopic surgery 2 years ago in another academic hospital with no improvement, and his activities of daily living were impaired due to worsening paresthesia. He denied any history of trauma and had no known comorbid diseases. Physical examination reveals normal gait (reduced stride, toe-off, and heel strike). A knee joint examination showed no tenderness on the joint line and anatomical landmarks, no palpable masses, and a symmetrical range of motion and symmetrical pulses. A back examination reveals no abnormality. A neurological examination revealed a sensation of 1/2 on the dorsum of the foot and weak dorsiflexion of 4/5. The systemic examination was unremarkable. A plain radiographic examination of the knee (Fig. 1) showed early degenerative changes of the tibiofemoral and patellofemoral joints, with joint space still maintained. The ultrasound revealed a homogeneous prominent mass measuring approximately 17.4 mm × 85.4 mm with an impression origin from the tibial nerve continuously proximally and distally. Doppler ultrasound findings were patent with compressible vessels and mass not compressible. Laboratory evaluation: His blood results were within normal limits. Magnetic resonance imaging (MRI) (Fig. 2) showed a fusiform-shaped mass with tapered ends of the sciatic nerve just above the popliteal fossa area, with multiple small ring-like structures hypodensity in T2WI and T1C+GD, normal popliteal vessels, and no intra-articular pathology.
The ultrasound revealed a homogeneous prominent mass measuring approximately 17.4 mm × 85.4 mm with an impression origin from the tibial nerve continuously proximally and distally. Doppler ultrasound findings were patent with compressible vessels and mass not compressible. Laboratory evaluation: His blood results were within normal limits. Magnetic resonance imaging (MRI) (Fig. 2) showed a fusiform-shaped mass with tapered ends of the sciatic nerve just above the popliteal fossa area, with multiple small ring-like structures hypodensity in T2WI and T1C+GD, normal popliteal vessels, and no intra-articular pathology. 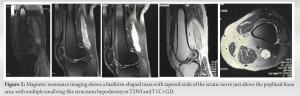 Nerve conduction and electromyography findings: Nerve conduction had a normal amplitude, normal latencies, and a normal SNAP. The electromyogram showed active denervation of the tibial nerve, anterior, and gastrocnemius, with some features of neurogenic recruitment. The peroneal nerve had normal findings. A surgical procedure (Fig. 3) was undertaken with the patient placed in the prone position, and a tourniquet was applied before turning the patient to the prone position. The procedure was done under sterile conditions. A posterior approach was used with an S-shaped incision over the popliteal crease and hemostasis was maintained by blunt dissection on the soft tissue plane.
Nerve conduction and electromyography findings: Nerve conduction had a normal amplitude, normal latencies, and a normal SNAP. The electromyogram showed active denervation of the tibial nerve, anterior, and gastrocnemius, with some features of neurogenic recruitment. The peroneal nerve had normal findings. A surgical procedure (Fig. 3) was undertaken with the patient placed in the prone position, and a tourniquet was applied before turning the patient to the prone position. The procedure was done under sterile conditions. A posterior approach was used with an S-shaped incision over the popliteal crease and hemostasis was maintained by blunt dissection on the soft tissue plane. A schwannoma was identified in the tibial and peroneal bundles of nerves. It was excised, fascicles were separated, and a 6 mm nerve conduit was split and used to hold the nerve fascicles together. The closure was done in layers, and a bulky dressing was applied. Histopathology analysis showed (Fig. 4) the following: (i) macroscopy findings: the specimen measures 27 mm × 20 mm × 18 mm and is firm, round, and nodular. On serial slicing, it showed a mixed tan-to-orange cut surface with no calcification, hemorrhage, or calcification. (ii) Microscopy findings: the tissue comprises a biphasic pattern of compact, hypercellular Antoni A areas and myxoid, hypocellular Antoni B areas.
A schwannoma was identified in the tibial and peroneal bundles of nerves. It was excised, fascicles were separated, and a 6 mm nerve conduit was split and used to hold the nerve fascicles together. The closure was done in layers, and a bulky dressing was applied. Histopathology analysis showed (Fig. 4) the following: (i) macroscopy findings: the specimen measures 27 mm × 20 mm × 18 mm and is firm, round, and nodular. On serial slicing, it showed a mixed tan-to-orange cut surface with no calcification, hemorrhage, or calcification. (ii) Microscopy findings: the tissue comprises a biphasic pattern of compact, hypercellular Antoni A areas and myxoid, hypocellular Antoni B areas.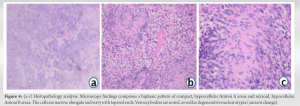 The cells are narrow, elongated, and wavy with taped ends. Verocay bodies are noted, as well as degenerative nuclear atypia. (iii) Immunohistochemistry: S-100 diffuse positive nuclear and cytoplasmic staining in neoplastic cells. In conclusion, a diagnosis of schwannoma was made. At the 2-week postoperative assessment, the wound was evaluated and found to be healed. Improvements in pain, numbness, and dorsiflexion were noted by the patient.
The cells are narrow, elongated, and wavy with taped ends. Verocay bodies are noted, as well as degenerative nuclear atypia. (iii) Immunohistochemistry: S-100 diffuse positive nuclear and cytoplasmic staining in neoplastic cells. In conclusion, a diagnosis of schwannoma was made. At the 2-week postoperative assessment, the wound was evaluated and found to be healed. Improvements in pain, numbness, and dorsiflexion were noted by the patient.
Schwannomas are rare benign tumors of the nerve sheath that originate from the Schwann cells of the peripheral nerve and have a broad anatomic distribution that includes superficial tissues (skin and subcutaneous areas), deep tissues including the central nervous system, and the gastrointestinal system [1,2]. Peripheral nerve sheath tumors consist of a heterogeneous group of neoplasms derived from one or more of the cell types that accompany peripheral nerve fibers. The predominant cell types include Schwann cells and perineurial cells. Schwann cells are neural crest-derived spindle cells that form the innermost layer of the endoneurium and are intimately associated with the nerve fibers [2,5]. They are described in the literature using different names, such as schwannoma and neurilemoma. Other synonymous names described include neurilemoma, neurinoma neurocytoma, peripheral glioma or perineurial fibroblastoma, peripheral glioma, and schwannoma since it was identified in 1908 by Verocay [4]. May be associated with syndromes such as neurofibromatosis types 1 or 2, multiple endocrine neoplasia, type II, and the carney complex [7,8,9]. Multiple schwannoma lesions are rare. Benign sciatic nerve schwannomas are usually isolated, solitary, well-circumscribed, and well-capsulated tumors and are rarely in the plexiform [3,10]. Lower limb extremities schwannoma is commonly found in the posterior tibial nerve, and involvement of sciatic nerve schwannoma is rare at 1% [4,10,11]. It has an incidence of 0.3–04/100.000 cases per year [12]. There are 72 previous reported cases of lower limb sciatic nerve schwannoma that we identified from the literature review from the past 51 years until December 2020 [1,3,4,5,6,8,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27]. The exact causes are not known, and there is no gender predilection described [12,15]. Females outnumbered males in the Telera et al. study by 60.9 to 39.1% [12]. These tumors usually present between the 2nd and 5th decades of life [12,13]. It is a slow-growing tumor over years, with a mean absolute growth rate of 1.69 cm3/year [2,3]. Sciatic nerve schwannoma is rarely associated with neurofibromatosis, with a reported incidence of 3%. 90% are sporadic, 2% have schwannomatosis, and 5% have meningiomatosis with or without neurofibromatosis type 2 [7,11,12]. Among the benign sciatic nerve tumors schwannomas account for 38%, while 60% are represented by neurofibromas [12]. Although a schwannoma may be found in isolation, it usually occurs with other features of neurofibromatosis as part of von Recklinghausen’s disease [10].
Diagnosis
Knee pain is the most common nontraumatic complaint in the elderly population. A comprehensive history and thorough physical examination are essential to exclude local and distant causes such as referred pain or a neurological condition. Pain is the principal symptom of a range of knee pathologies. Knee pain is one of the commonest regional musculoskeletal pains and is reported by 25% of people over 55 years old [28]. Pain has distinctive features such as location, character, severity, and timing. Schwannoma’s clinical presentation is non-specific, which leads to delayed diagnosis and treatment. They present with a compression effect such as radicular pain (difficult to diagnose or painless), neuropraxia or paresthesia, the Tinel sign of palpation, and difficulty palpating the mass [6,11,12]. A radiological investigation is useful to rule out differential causes and describe the exact location of the lesion, which assists the surgical decision. MRI is the most sensitive investigation, which showed a fusiform-shaped mass with tapered ends of the sciatic nerve just above the popliteal fossa area, with multiple small ring-like structures and hypodensities in T2WI and T1C+GD, normal popliteal vessels, and no intra-articular pathology. Features suggestive of schwannoma or neurofibroma in our case. T1-weighted MRI shows a low-signal-intensity mass within the nerve. T2-weighted MRI will show a hyperintense signal of the mass and a heterogeneous or homogeneous appearance [5,12,15]. Maes et al. MRI is the imaging modality of choice [4]. Plain radiography and nerve conduction studies are not often helpful [16]. Ultrasound is sensitive enough to identify a well-defined nerve mass, but the contact examination of the nerve is challenging [4]. Ultrasound showed a well-defined, round mass, a heterogeneous lesion with cystic degeneration, or a homogeneous and eccentric lesion [5, 7, 13]. Color Doppler along with compression is very effective, as an obliteration of flow with compression is seen with schwannoma and not with neurofibromas or lymph nodes [5]. A biopsy is mandatory to confirm the diagnosis [6] Maini et al. reported a rare case of sciatic schwannoma of the thigh detected on a bone scan in their case to exclude reflex sympathetic dystrophy (8). Computed tomography scan demonstrates a well-defined, ovoid, soft tissue density mass and its accurate location [5,14]. A differential diagnosis of a benign peripheral nerve sheath tumors include leiomyomas, malignant peripheral nerve sheath tumors(MPNSTs), synovial sarcomas, fibrosarcomas, leiomyosarcomas, and melanoma [7]. A differential diagnosis of knee pain: anterior knee pain includes a minor meniscal tear, Hoffa’s fat pad syndrome, quadriceps, patellar tendinopathy, Osgood–Schlatter disease, bursitis, Plica syndrome, patella subluxation, patellofemoral pain, chondromalacia patella, and a patellar stress fracture [9,29]. Lateral knee pain includes iliotibial band tendinopathy and a lateral collateral ligament sprain. Medial knee pain includes medial collateral ligament sprain, medial plica syndrome, and pes anserine bursitis. Posterior knee pain includes a popliteal (Baker’s) cyst. Associated effusion symptoms include septic arthritis and crystalline disease (gout, pseudogout) [13,29]. Macroscopy: A schwannoma nodule is a fusiform, round, or oval mass that is sharply circumscribed and encapsulated. It is commonly <5 cm in diameter and more than 5 cm in the retroperitoneum and mediastinum regions. Microscopy: high and low cellular regions called Antoni A and B Antoni. A focus area has foci of palisade nuclei called Verocay bodies and thick capsules. Blood vessels may be present with a hyalinized layer. Immunohistochemically, schwannomas show intense and relatively uniform staining for S-100 protein, which is a marker for Schwann cells [4,6,9,11,12,13,30]. Histological schwannoma variants include ancient schwannoma, plexiform schwannoma, cellular schwannoma, epithelioid schwannoma, melanotic (pigmented) schwannoma, schwannoma with pseudoglandular elements, cystic schwannoma, and psammomatous schwannoma. Classical schwannomas are more common and commonly found in the following locations: the head and neck region, followed by the extremities, seen over a wide age range [7,30]. Excision surgery is the treatment of choice for the tumor. The outcomes are usually good, with a reported very low recurrence rate and malignant transformation rate of 5% [10,12].
Schwannomas are rare causes of radicular knee pain. The clinical features are usually non-specific. A comprehensive history, focused physical examination, and dedicated special investigations are essential to rule out extra-articular causes of knee pain and avoid delay in diagnosis. The diagnosis is confirmed by a biopsy. The treatment of schwannoma is excision, which provides good pain relief and functional outcomes and has a very low recurrence rate and malignant transformation.
Sciatic nerve schwannomas are uncommon and simple to overlook. When evaluating knee pain in all patients, a systematic approach should be used. Rare causes of knee pain should be looked for when routine investigations are normal.
References
- 1.Das Gupta TK, Brasfield RD, Strong EW, Hajdu SI. Benign solitary schwannomas (neurilemomas). Cancer 1969;24:355-66. [Google Scholar | PubMed]
- 2.Cavalcante JB, Cembraneli PN, Cavalcante RB, Valente VF, Cavalcante JE. Unusual presentation of giant schwannoma in the sciatic nerve. Case Rep Int 2020;9:1-4. [Google Scholar | PubMed]
- 3.El Sayed L, Masmejean EH, Parfait B, Kalamarides M, Biau D, Peyre M. Natural history of peripheral nerve schwannomas. Acta Neurochir (Wien) 2020;162:1883-9. [Google Scholar | PubMed]
- 4.Maes R, Ledoux P, de Brouckere G. A rare cause of sciatica: Sciatic nerve schwannom-report of one case with long subclinical course and misleading presentation. SICOT J 2020;6:16. [Google Scholar | PubMed]
- 5.Thomas SC, Gurushankar G, Anand SH. Schwannoma of the sciatic nerve-a case report. Res J Med Allied Health Sci 2020;3:24-7. [Google Scholar | PubMed]
- 6.Knight DM, Birch R, Pringle J. Benign solitary schwannomas: A review of 234 cases. J Bone Joint Surg Br 2007;89:382-7. [Google Scholar | PubMed]
- 7.Abdellatif E. Schwannoma. Available from: https://www.pathologyoutlines.com/topic/softtissueschwannoma.html [Last accessed on 2021 Mar 20]. [Google Scholar | PubMed]
- 8.Maini A, Tripathi M, Shekar NC, Malhotra A. Sciatic schwannoma of the thigh detected on bone scan: A case report. Clin Imaging 2003;27:191-3. [Google Scholar | PubMed]
- 9.Ilagan C, Poliakin L, Asarian A, Xiao P, Sirsi S. Anterior knee schwannoma. J Surg Case Rep 2019;2019:rjz236. [Google Scholar | PubMed]
- 10.Rhanim A, El Zanati R, Mahfoud M, Berrada MS, El Yaacoubi M. A rare cause of chronic sciatic pain: Schwannoma of the sciatic nerve. J Clin Orthop Trauma 2013;4:89-92. [Google Scholar | PubMed]
- 11.George K, Burke S, Arkun K, Riesenburger R. Cauda Canis: Variation of a Tinel’s sign for a sciatic nerve tumor. Case Rep Neurol Med 2020;2020:8822866. [Google Scholar | PubMed]
- 12.Telera S, Raus L, Vietti V, Pace A, Villani V, Galié E, et al. Schwannomas of the sciatic nerve: A rare and neglected diagnosis. A review of the literature with two illustrative cases. Clin Neurol Neurosurg 2020;195:105889. [Google Scholar | PubMed]
- 13.Nahar S, Goyal A. A large schwannoma of sciatic nerve-a case report. J Periphe Nerve Surg 2018;2:86-9. [Google Scholar | PubMed]
- 14.Thiebot J, Laissy JP, Delangre T, Biga N, Liotard A. Benign solitary neurinomas of the sciatic popliteal nerves CT study. Neuroradiology 1991;33:186-8. [Google Scholar | PubMed]
- 15.Woo PY, Ho JM, Ho JW, Mak CH, Wong AK, Wong HT, et al. A rare cause of sciatica discovered during digital rectal examination: Case report of an intrapelvic sciatic notch schwannoma. Br J Neurosurg 2019;33:562-5. [Google Scholar | PubMed]
- 16.Henky J, Faried A. Functional recovery of rare case of sciatic nerve schwannoma with peripheral nerve block. Bandung Medical Journal 2020;52:119-124. [Google Scholar | PubMed]
- 17.Wu WT, Chang KV, Hsu YC, Yang YC, Hsu PC. Ultrasound imaging for a rare cause of sciatica: A schwannoma of the sciatic nerve. Cureus 2020;12:e8214. [Google Scholar | PubMed]
- 18.Munakomi S, Shrestha P. Case report: Sciatic nerve schwannoma-a rare cause of sciatica. F1000Res 2017;6:267. [Google Scholar | PubMed]
- 19.Chikkanna JK, Gopal S, Sampath D. Mystery of sciatica resolved-a rare case report. J Clin Diagn Res 2016;10:D04-5. [Google Scholar | PubMed]
- 20.Blohm D, Hansen LB, Jakobsen BW. Hamstring pain in an athletic sprinter caused by a schwannoma of the sciatic nerve. Knee Surg Sports Traumatol Arthrosc 1999;7:135-6. [Google Scholar | PubMed]
- 21.Gominak SC, Ochoa JL. Sciatic schwannoma of the thigh causing foot pain mimicking plantar neuropathy. Muscle Nerve 1998;21:528-30. [Google Scholar | PubMed]
- 22.Artico M, Cervoni L, Wierzbicki V, D’Andrea V, Nucci F. Benign neural sheath tumours of major nerves: Characteristics in 119 surgical cases. Acta Neurochir (Wien) 1997;139:1108-16. [Google Scholar | PubMed]
- 23.Sato M, Handa J, Koyama T. Solitary schwannoma of sciatic nerve. Diagnosis by CT. Nihon Geka Hokan 1982;51:534-6. [Google Scholar | PubMed]
- 24.Dubuisson A, Fissette J, Vivario M, Reznik M, Stevenaert A. A benign tumor of the sciatic nerve: Case report and review of the literature. Acta Neurol Belg 1991;91:5-11. [Google Scholar | PubMed]
- 25.Nose Y, Naito A, Kato T, Mori R, Oneda Y, Ishida T, et al. A case of schwannoma originating from the sciatic nerve. Gan To Kagaku Ryoho 2016;43:2435-7. [Google Scholar | PubMed]
- 26.Guedes F, Brown RS, Torrão-Júnior FJ, Siquara-de-Sousa AC, Amorim RM. Nondiscogenic sciatica: What clinical examination and imaging can tell us? World Neurosurg 2020;134:e1053-61. [Google Scholar | PubMed]
- 27.Murthy NK, Sharma M, Spinner RJ. Primary peripheral nerve tumors associated with nerve-territory herpes zoster. Acta Neurochir (Wien) 2020;162:1147-51. [Google Scholar | PubMed]
- 28.Peat G, Thomas E, Handy J, Wood L, Dziedzic K, Myers H, et al. The knee clinical assessment study--CAS(K). A prospective study of knee pain and knee osteoarthritis in the general population. BMC Musculoskelet Disord 2004;5:4. [Google Scholar | PubMed]
- 29.Covey CJ, Hawks MK. Nontraumatic knee pain: A diagnostic and treatment guide. J Fam Pract 2014;63:720-8. [Google Scholar | PubMed]
- 30.Patil SB, Chatura KR. Schwannoma and its unusual variants-a histopathological study. Indian J Pathol Oncol 2016;3:727-31. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Schwannoma Arising from the Deep Peroneal Nerve: A Case Report
July 1, 2026 Schwannoma Arising from the Deep Peroneal Nerve: A Case Report April 1, 2026 A Rare and Interesting Case of Sciatic Nerve Compression Due to Proximal Femoral Osteochondroma in a Young Adult – A Case Report
April 1, 2026 A Rare and Interesting Case of Sciatic Nerve Compression Due to Proximal Femoral Osteochondroma in a Young Adult – A Case Report March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study
March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study