
Early surgery could be safe and effective in babies with polymelia.
Dr. Dominic Konadu-Yeboah, Department of Orthopaedics and Trauma, Komfo Anokye Teaching Hospital, Kumasi, Ghana; Department of Surgery, School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana. E-mail: domiyk@yahoo.com
Abstract
Introduction: Polymelia is the presence of supernumerary limbs attached to a segment of the body. It occurs in about 6/10,000 live births with 1.1/10,000 cases involving the lower limbs. It has a heterogeneous pathogenesis including incomplete separation of monozygotic twins.
Case Report: A 5-month-old baby with polymelia associated with ectopic right kidney, anorectal agenesis with a rectovaginal fistula, and right corneal opacity, delivered through cesarean section at 37 weeks, 3-day gestation to a 38-year-old mother. There were no known predisposing factors.
Conclusion: In the management of polymelia, a thorough clinical and radiological assessment to identify additional anomalies is critical, and early surgical intervention is safe and optimizes survival.
Keywords: Polymelia, pyromelia, APGAR score.
Polymelia, the presence of supernumerary limbs attached to a segment of the body, is a rare limb malformation that occurs in about 6/10,000 live births with 1.1/10,000 involving the lower limbs [1]. It has a heterogeneous pathogenesis including incomplete separation of monozygotic twins [2]. In human embryogenesis, limb formation occurs in the 4th and 5th weeks of gestation, during which two pairs of limb buds develop from both sides of the embryo, comprising cells from the ectoderm and mesoderm [3]. Maternal exposure to ionizing radiation and some medications such as thalidomide or progesterone, as well as infectious agents and toxins, during early pregnancy, is a risk factor for limb defects in children born to those mothers. The anomaly is associated with genetic mutations and chromosomal aberrations [4,5,6]. Polymelia can be diagnosed in utero with antenatal ultrasonography [7]. The classification of this condition is based on the body region to which the accessory limb is attached. Pyromelia refers to extra limbs attached to the pelvis, thoracomelia to extra limbs attached to the thorax, notomelia to extra limbs attached to the spine, and it is called cephalomelia when the extra limbs are attached to the head [7]. Polymelia may occur in association with other congenital anomalies such as cardiac defects and hepatic dysplasia. The prognosis of the disease depends on the type of polymelia and the related abnormalities [8]. It may present as a component of the omphalocele exstrophy imperforate anus spinal defects (OEIS) complex which is a congenital malformation syndrome. Babies with OEIS complex may present with polymelia, omphalocele, spinal defects, absence of urinary bladder, ambiguous anus, and genitalia [9]. The management of polymelia involves thorough clinical and radiological evaluations to exclude any related congenital anomalies followed by excision of the false limbs. With timely and appropriate treatment, affected babies tend to have favorable growth and development. Furthermore, surgical resection of the supernumerary limbs at an early age is recommended [2,10,11].
We report a case of a 5-month-old female baby delivered through cesarean section at 37 weeks + 3-days gestation, on account of maternal request for bilateral tubal ligation, to a 38-year-old para 5 mother with APGAR score of 8 and 9 at 1 and 5 min, respectively. The baby was delivered at a district hospital and referred to the Komfo Anokye Teaching Hospital 4 hours after birth, with a birth weight of 3.7 kg. There was associated anorectal agenesis with a rectovaginal fistula, for which a sigmoid colostomy was performed at 3 weeks of age. The mother had no known history of exposure to teratogenic agents such as ionizing radiation or hormonal contraceptives. She has no family history of hereditary diseases or congenital anomalies and no history of birth defects in her community. In addition, the mother of the baby had no history of consanguinity or illness during pregnancy. The baby is the last of 5 children all of whom are alive and well. The mother is a teacher, and the father, a 44-year-old banker. None of the parents smoke cigarette, and the mother’s immunization was up to date. The mother was a regular antenatal clinic attendant. She had antenatal ultrasonography which did not document any fetal anomaly. There is no known history of maternal ingestion of teratogenic medications in the first trimester of pregnancy. At birth, the baby had six limbs, two upper and four lower limbs, vitiligo on the root of the nose, and a right corneal opacity. The two medial lower limbs had power of 1/5, and the power in the two lateral lower limbs was 5/5. There were two pelvises, each had a genitalia and palpable pelvic bones. The genitalia of both pelvises were phenotypically female, vestigial on the right and well developed on the left, with mons pubis, clitoris, labia majora and minora, and an introitus which exuded feces and urine. There was an associated sacral meningocele. An abdominal ultrasound scan found an ectopically located right kidney at the right iliac fossa, adjacent to the urinary bladder which was malrotated and enlarged 6.5 cm by 3.0 cm, with the dilatation of the right pelvicalyceal system. There was a single urinary bladder which was of uniform wall thickness and a single uterus measuring 2.5 by 1.1 cm, which was centrally located in the pelvis. Computed tomography scan of the chest, abdomen, and pelvis as well as magnetic resonance imaging of the spine was undertaken to help rule out additional anomalies. Echocardiogram was performed, and the findings were normal. Hip disarticulation with triradiate cartilage enucleation of the dysplastic medial lower limbs, symphysiodesis with size 2 ethibond sutures, soft-tissue reconstruction, and closure of the meningocele was performed under general anesthesia and fluoroscopic guidance. The surgery was performed at 5 months of age. The clinical photograph, as well as a plain X-ray of the baby, that was taken at 3 weeks of age, before the surgery, is shown in Fig. 1. The ventral and dorsal appearances of the baby at the time of surgery are depicted in Fig. 2.
The ventral and dorsal appearances of the baby at the time of surgery are depicted in Fig. 2. The immediate post-operative ventral and dorsal photographs are shown in Fig. 3.
The immediate post-operative ventral and dorsal photographs are shown in Fig. 3. In addition, a picture showing the ventral surface of the baby, 10 days following the surgery and a post-operative plain radiograph are shown in Fig. 4; 6 months following the surgery, the baby is alive and well, as shown in Fig. 5.
In addition, a picture showing the ventral surface of the baby, 10 days following the surgery and a post-operative plain radiograph are shown in Fig. 4; 6 months following the surgery, the baby is alive and well, as shown in Fig. 5.
Polymelia has rarely been reported in humans. The reported anomalies involving the limbs include amelia, meromelia, and phocomelia. Our case, pyromelic polymelia, and its diagnosis at birth, are extremely uncommon in literature. In Niger, a baby born with multiple malformations including polymelia has been reported, in whom there was accessory male genitalia at the base of a supernumerary limb which had no motor or sensory function. There was a vestigial appendage with an adjacent sinus that communicated with the dura mater through a defect in the vertebral arches. Three cases have been reported in consanguineous parents in the same ethnic group supporting the genetic basis of the condition [12]. Similarly, in the baby of our report, the medial two lower limbs had impaired motor function; there was sacrococcygeal myelomeningocele and an ectopic right kidney. However, there was no history of consanguinity or ethnic group prevalence. The diagnosis of congenital malformations on pre-natal ultrasonography has been recommended [9]. In the baby of this report, on the other hand, the diagnosis of polymelia was made at birth. The mouse mutant disorganization Ds gene has been shown to be widely associated with the development of polymelia. It is lethal in homozygotes and has variable penetrance in heterozygotes. Fibroblast growth factors −1, −2, −4, and −8 have been demonstrated to cause polymelia in chick embryos experimentally [1]. In our case, no predisposition to the condition has been identified yet. The need for a radiological evaluation of babies with polymelia for additional congenital abnormalities, before surgical excision has been demonstrated [2,13]. A thorough clinical and radiological evaluation preceded the surgical intervention in the management of the baby of this report which could explain the favorable outcome. Considering the paucity of literature on polymelia, further studies are recommended to deepen our understanding on the management and long-term treatment outcomes of babies with polymelia.
In the management of polymelia, a thorough clinical and radiological assessment to identify additional anomalies is critical, and early surgical intervention is safe and optimizes survival. The cause of the malformation may not be evident at the time of diagnosis and treatment.
The management of polymelia is multidisciplinary and early surgery could be safe and effective.
References
- 1.Pitchaiah G, Pushpalatha E. Pathogenesis of horrifying rare genetic disorders in humans-a review. Pharma Innov 2017;6:85-9. [Google Scholar | PubMed]
- 2.Montalvo N, Redrobán L, Espín VH. Incomplete duplication of a lower extremity (polymelia): A case report. J Med Case Rep 2014;8:184. [Google Scholar | PubMed]
- 3.O’Rahilly R, Muller F. Developmental Stages in Human Embryos. Publication No 637. Washington: Carnegie Institution; 1987. [Google Scholar | PubMed]
- 4.Griffet J, Bastiani-Griffet F, Jund S, Moreigne M, Zabjek KF. Duplication of the leg--renal agenesis: Congenital malformation syndrome. J Pediatr Orthop B 2000;9:306-8. [Google Scholar | PubMed]
- 5.La Torre R, Fusaro P, Anceschi MM, Montanino-Oliva M, Modesto S, Cosmi EV. Unusual case of caudal duplication (dipygus). J Clin Ultrasound 1998;26:163-5. [Google Scholar | PubMed]
- 6.Kher AS, Gahankari DR, Tambwekar SR, Doraiswamy A, Iyer S, Bharucha BA, et al. Supernumerary limbs: A case report of a rare congenital anomaly. Ann Plast Surg 1996;37:549-52. [Google Scholar | PubMed]
- 7.Verma S, Khanna M, Tripathi VN, Yadav NC. Occurrence of polymelia in a female child. J Clin Imaging Sci 2013;3:18. [Google Scholar | PubMed]
- 8.Liu J, Liu Y, Xue Y, Guo Y. Prenatal ultrasound-based diagnosis of fetal OEIS complex associated with lower limb polymelia and cardiac, hepatic dysplasia: A case report. Clin Case Rep 2019;7:2153-5. [Google Scholar | PubMed]
- 9.Liu J, Liu Y, Xue Y, Guo Y. Prenatal ultrasound-based diagnosis of fetal OEIS complex associated with lower limb polymelia and cardiac, hepatic dysplasia: A case report. Clin Case Rep 2019;7:2153-5. [Google Scholar | PubMed]
- 10.Acharya S, Pradhan NK, Rao PT. Congenital incomplete reduplication of the lower limb. A case report. Int Orthop 1993;17:308-9. [Google Scholar | PubMed]
- 11.García-Espinosa I, García-Cruz R, Huerta-Mendoza H, Cabrera-Hernández R, Merelo-Villafán I, López-Alfonso A. Polymelia: Case report and review of the literature. Acta Ortop Mex 2002;16:272-5. [Google Scholar | PubMed]
- 12.Kelani AB, Moumouni H, Issa AW, Younsaa H, Fokou H, Sani R, et al. Notomelia and related neural tube defects in a baby born in Niger: Case report and literature review. Childs Nerv Syst 2017;33:529-34. [Google Scholar | PubMed]
- 13.Norman WH. A child with three lower extremities. J Bone Joint Surg Am 1964;46:1755-8. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 28, 2019 Management of an Open Distal Radius Epiphysiolysis in a 14-year-old Male: A Case Report
November 28, 2019 Management of an Open Distal Radius Epiphysiolysis in a 14-year-old Male: A Case Report March 11, 2017 An Isolated Pure Dislocation of Fifth Carpometacarpal Joint: Case Report and Review of Literature
March 11, 2017 An Isolated Pure Dislocation of Fifth Carpometacarpal Joint: Case Report and Review of Literature May 10, 2024 Magnetic Resonance Imaging in the Evaluation of Avulsion Injuries of the Pelvis and Hip in Adolescent Professional Footballers: A Case Series
May 10, 2024 Magnetic Resonance Imaging in the Evaluation of Avulsion Injuries of the Pelvis and Hip in Adolescent Professional Footballers: A Case Series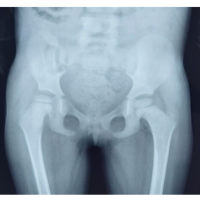 November 10, 2021 Freeman-Sheldon Syndrome with Stiff Knee Gait – A Case Report
November 10, 2021 Freeman-Sheldon Syndrome with Stiff Knee Gait – A Case Report