
While choosing the femoral neck system, it is imperative to consider the type of neck femur fracture, the trauma to surgery time, as well as the age of the patient.
Dr. Joydeep K Dey, Department of Orthopaedics, Dr. DY Patil Medical College and Hospital, Mumbai, Maharashtra, India. E-mail: Jdey0000@gmail.com
Abstract
Introduction: The femoral neck system (FNS) represents an emerging fixation system designed for the management of femoral neck fractures. This innovative system combines the mechanical benefits of compression and anti-rotation properties in internal fixation. Biomechanical studies have demonstrated the superior axial and rotational stability of the FNS implant when compared to traditional cannulated screws and dynamic hip screw. Despite these promising mechanical advantages, there is currently a limited body of literature addressing the factors contributing to FNS failure. A thorough assessment of the safety and outcomes associated with this novel implant is essential.
Case Report: In this context, we present three cases wherein FNS failure occurred, aiming to elucidate the potential causes behind these failures, and had to undergo either an implant removal or bipolar hemiarthroplasty.
Conclusion: While considering the femoral neck system as the implant of choice, we should consider the age, injury to surgery time, and the location of the fracture line . However, we cannot conclusively ascertain whether age contributes independently to the risk of failure.
Keywords: Femoral neck system, neck femur fracture, limitations, subcapital fracture.
With increasing age, neck of femur fractures has become a common injury in the 3rd to 4th decade and elderly population[1,2]. Various methods of internal fixation such as cannulated compression screws, sliding hip screws, and pin system, have been used for the treatment of neck of femur fractures. However, post-operative failure of internal fixation is common. Various other studies have reported that 7–22% of patients receive secondary operations, mostly due to complications, such as avascular necrosis of the femoral head, non-union, severe femoral neck shortening, and implant cut out [3,4]. To decrease the post-operative complications, researchers are trying to constantly surpass and improve the already existent internal fixation systems and have now come up with femoral neck systems (FNSs) which consist of a blade, a barrel, a derotation screw, a barrel plate, and a locking screw. It exhibits anti-sliding, anti-rotation, and anti-shearing functions. There is very sparse literature available in context with the drawbacks or the possible limitations of this implant, and hence, this case report may add to the implant’s existing literature.
Case 1
A 53-year-old male was brought to the Outpatient Department, with a complaint of pain in the right hip and difficulty in walking 2 months after being treated for a right-sided subcapital neck of femur fracture with the FNS. He had been operated on, 9 days after the initial fall as he delayed seeking medical assistance. Postoperatively the patient had no significant complaints. On the radiograph, a varus collapse of the right hip with the implant impinging the joint line was noted (Fig. 1). The implant had to be removed (Fig. 2) and the patient was rehabilitated withhip range of motion exercises on day 3, followed by weight bearing commenced on day 7.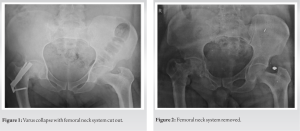
Case 2
A 48-year-old male presented to the outpatient department complaining of pain in the left hip during flexion, 10 months after receiving treatment for a left-sided subcapital neck of femur fracture (Fig. 3).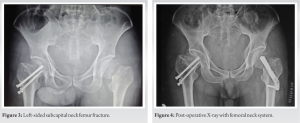 The initial treatment involved the use of the FNS (Fig. 4). The surgical intervention occurred 11 days after the initial fall due to the patient’s unfit condition for immediate surgery. Postoperatively, the patient regained full range of motion. However, on subsequent radiographs, an implant cut out with non-union was observed (Fig. 5).
The initial treatment involved the use of the FNS (Fig. 4). The surgical intervention occurred 11 days after the initial fall due to the patient’s unfit condition for immediate surgery. Postoperatively, the patient regained full range of motion. However, on subsequent radiographs, an implant cut out with non-union was observed (Fig. 5).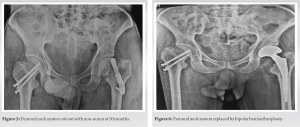 To address this complication, the implant had to be replaced with a bipolar hemiarthroplasty (Fig. 6). Following the replacement procedure, the patient underwent rehabilitation, including hip range of motion exercises on day 1, with weight-bearing initiated on day 3.
To address this complication, the implant had to be replaced with a bipolar hemiarthroplasty (Fig. 6). Following the replacement procedure, the patient underwent rehabilitation, including hip range of motion exercises on day 1, with weight-bearing initiated on day 3.
Case 3
A 42-year-old female visited the outpatient department, reporting an inability to walk 10 months after receiving treatment for a left-sided subcapital neck of femur fracture utilizing the FNS. The surgical procedure took place 8 days after the initial fall, as the patient initially hesitated about undergoing surgery (Fig. 7) Following the operation, the patient regained full range of motion. Unfortunately, she was lost to follow-up and reappeared directly after 12 months. On assessment through a pelvis with both hips radiograph, indications of a screw cutout were observed (Fig. 8). Despite counseling, the patient expressed unwillingness to undergo any further management.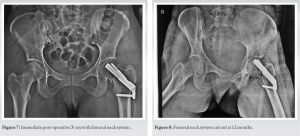
Surgical interventions for femoral neck fractures primarily encompass internal fixation and primary arthroplasty. The choice of treatment is contingent on factors such as the extent of displacement, the presence of hip osteoarthritis, the patient’s age, the quality of reduction achieved, and the stability. The FNS represents a relatively recent innovation in the realm of internal fixation devices designed for femur neck fracture fixations [4-6]. The FNS furnishes stable fixation with an angular orientation of 130° between the femoral neck and shaft, amalgamating the merits of angular stability with minimally invasive surgical techniques [7]. It reduces soft-tissue trauma and reduces the total intraoperative time. Biomechanical load tests have evidenced that the FNS affords superior resistance against deformation and demonstrates less sensitivity to deviations in implant placement [8,9]. Comparative studies with cannulated compression screws and dynamic hip screws have reported gratifying short-term clinical results with the utilization of the FNS. Nevertheless, there is no literature stating the direct limitations of the FNS. Hence, in this report, complications have been highlighted such as screw back out, avascular necrosis (AVN), and non-union of the neck of the femur [10]. While internal fixation is frequently favored for individuals in the young and middle-aged, this topic has still been debated. Certain investigations suggest a heightened incidence of complications in the age group above 40 due to poor bone quality, compromised healing capabilities of the body, and associated comorbidities underscoring the critical role of patient selection and surgical proficiency. Anatomical classification of neck of femur fractures categorizes femur fractures based on the anatomical location of the fracture line and is regarded as a contributory factor for failure of FNS. It has been mainly observed in the subcapital type of fracture as there is a limited purchase for the screw proximally, while inserting the head screw, the small proximal fragment tends to rotate easily leading to inadequate compression and implant failure. We also observed that fixing the fracture early, within 7 days, was a modifiable factor that could be considered to prevent AVN of the femoral head. It is a well-known factor worldwide, that neck femur fracture interferes with the blood supply and increases the chances of osteonecrosis of the head femur with prolonged injury to surgery time. Hence, it is necessary to fix the neck of the femur fracture as early as possible [10].
While patient selection we should consider the age, injury to surgery time, and the location of the fracture line before choosing the FNS in the treatment of a fractured neck of femur. However, we cannot conclusively ascertain whether age contributes independently to the risk of failure.
While choosing the FNS, it is imperative to consider the type of neck femur fracture, the trauma to surgery time, as well as the age of the patient.
References
- 1.Stoffel K, Zderic I, Gras F, Sommer C, Eberli U, Mueller D, et al. Biomechanical evaluation of the femoral neck system in unstable Pauwels III femoral neck fractures: a comparison with the dynamic hip screw and cannulated screws. J Orthop Trauma 2017;31:131-7. [Google Scholar | PubMed]
- 2.Lu Y, Huang Z, Xu Y, Huang Q, Ren C, Li M, et al. Femoral neck system versus cannulated screws for fixation of femoral neck fracture in young adults: a systematic review and meta-analysis. Am J Transl Res 2022;15:5480-90. [Google Scholar | PubMed]
- 3.Hu H, Cheng J, Feng M, Gao Z, Wu J, Lu S, et al. Clinical outcome of femoral neck system versus cannulated compression screws for fixation of femoral neck fracture in younger patients. J Orthop Surg Res 2021;16:370. [Google Scholar | PubMed]
- 4.Tang Y, Zhang Z, Wang L, Xiong W, Fang Q, Wang G. Femoral neck system versus inverted cannulated cancellous screw for the treatment of femoral neck fractures in adults: A preliminary comparative study. J Orthop Surg Res 2021;16:504. [Google Scholar | PubMed]
- 5.Zhou XQ, Li ZQ, Xu RJ, She YS, Zhang XX, Chen GX, et al. Comparison of early clinical results for femoral neck system and cannulated screws in the treatment of unstable femoral neck fractures. Orthop Surg 2021;13:1802-9. [Google Scholar | PubMed]
- 6.Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury 2015;46:484-91. [Google Scholar | PubMed]
- 7.Florschutz AV, Langford JR, Haidukewych GJ, Koval KJ. Femoral neck fractures: Current management. J Orthop Trauma 2015;29:121-9. [Google Scholar | PubMed]
- 8.Panteli M, Rodham P, Giannoudis PV. Biomechanical rationale for implant choices in femoral neck fracture fixation in the non-elderly. Injury 2015;46:445-52. [Google Scholar | PubMed]
- 9.Slobogean GP, Stockton DJ, Zeng B, Wang D, Ma BT, Pollak AN. Femoral neck fractures in adults treated with internal fixation: a prospective multicenter Chinese cohort. J Am Acad Orthop Surg 2017;25:279-303. [Google Scholar | PubMed]
- 10.Schopper C, Zderic I, Menze J, Müller D, Rocci M, Knobe M. Higher stability and more predictive fixation with the femoral neck system versus Hansson Pins in femoral neck fractures Pauwels II. J Orthop Transl 2020;24:88-95. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report
July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System September 1, 2025 Failure of the Femoral Neck System in a Young Patient: A Case Report
September 1, 2025 Failure of the Femoral Neck System in a Young Patient: A Case Report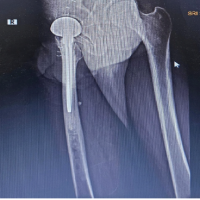 November 1, 2024 A Prospective Case Series – Study of Neck of Femur Fractures in Elderly Patients with Pre-operative Urinary Tract Infection in Rural India
November 1, 2024 A Prospective Case Series – Study of Neck of Femur Fractures in Elderly Patients with Pre-operative Urinary Tract Infection in Rural India