
This unique case report introduces a worldwide first case of augmenting the retained acetabular shell with a dual mobility cup using Double Socket Technique showcasing its effectiveness in addressing instability, shortening surgical time, and reducing bone loss in patients with multiple prior surgeries.
Dr. Sanjay Agarwala, Consultant Orthopedic Surgeon, Director-Professional Services, P.D. Hinduja National Hospital, Mumbai, India. E-mail: drsa2011@gmail.com
Abstract
Introduction: Prevention of dislocation after total hip arthroplasty (THA) remains a topic of debate. There are various surgical options to manage hip instability such as large femoral heads, and constrained liners, although the best option to tackle this is still controversial. In revision scenarios with previous well-fixed acetabulum shells, the cementation of polyethylene liners or the cementation of dual mobility (DM) into a well-fixed acetabulum shell (Double Socket Technique) has been documented before. Here, we report a case of re-revision THA, where we have used the Double Socket Technique of retaining the previous well-fixed acetabular shell with the cementation of the DM cup along with an anti-protrusio cage inside the socket. To the best of our knowledge, this is the first such a case to be reported worldwide.
Case Report: A 54-year-old male who underwent THA in 1990 and an acetabulum cup revision in 2003 presented to us with right hip pain. Radiographs showed Paprosky Type 3A femoral bone loss and polyethylene wear. Intraoperatively after removing the polyethylene liner, the acetabulum shell was found to be well fixed and therefore retained. To increase stability, an anti-protrusio cage was inserted over it and a DM cup was cemented onto it (double socket). The femoral stem was revised using Wagner stem and encerclage wires and a hook plate was used to stabilize the osteotomy site.
Conclusion: This technique is a reliable option and helps shorten the surgical time and reduce the bone loss that can occur in extracting a well-fixed acetabulum shell. The use of a DM cup decreases the chances of instability compared to the cementation of polyethylene liners and decreases the high failure rate associated with the use of cementation of constrained liners. The addition of an anti-protrusio cage in addition to the Double Socket Technique increases the stability of the construct.
Keywords: Anti-protrusio cage, Dual mobility, Double socket, Revision total hip arthroplasty, Well-fixed acetabulum
Dislocation rates vary from 0.3 to 10% after primary Total Hip Arthroplasty (THA) and 14-28% in the revision scenario [1]. Multiple surgeries, neuromuscular disease, cognitive impairment, advanced age, tissue damage, and previous instability are significant risk factors for post-operative dislocations [2]. Although there are various surgical options to manage hip instability such as large femoral heads and constrained liners, high failure rates have been reported in the revision scenario [3,4]. The best option to tackle instability in the revision scenario is still controversial. The dual mobility (DM) THA has been used successfully for instability worldwide [5,6]. These THA have a greater range of motion due to the large head-neck ratio, and large head size and also provide decreased stresses at the cement interface compared to constrained liners [6]. In the revision of the well-fixed acetabular component, the cemented acetabular shell extraction can be difficult and can increase bone loss that is sometimes present secondary to osteolysis [7]. One option in such a revision scenario is the cementation of polyethylene liners or the cementation of DM into a well-fixed acetabulum shell, also termed the Double Socket Technique [7,8]. The concept of cementing DM into an existing acetabulum shell has been documented before [9]. It helps shorten the operative time and reduce bone loss or damage [10]. Here, we report a case of re-revision THA where we used the Double Socket Technique of retaining the previous well-fixed acetabular shell with the cementation of the DM cup along with an anti-protusio cage inside the socket. This is the first of such a case to be reported worldwide to the best of our knowledge.
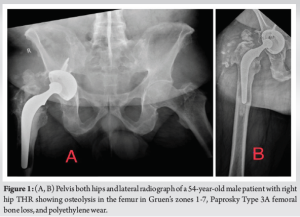
A 54-year-old male known case of ankylosing spondylitis was operated on for right THR in 1990 (Charnley) and underwent first revision in 2003 where the Charnley cup was revised to a large uncemented component. Fourteen years after the revision THR, the patient presented to us with right hip pain which worsened with activity. On presentation, radiographs showed osteolysis in the femur in Gruen’s zones 1-7, Paprosky Type 3A femoral bone loss, and polyethylene wear (Fig. 1). The acetabular component seemed to be well fixed on radiographs and CT scan. Blood investigations and ultrasound-guided aspiration ruled out infection.
A posterior approach was taken, and intraoperative samples were sent for culture and histopathology. An extended trochanteric osteotomy to remove the stem and cement mantle was done. The old polyethylene liner was removed (Fig. 2A) retaining the acetabular shell which was found to be well-fixed and stable. As the shell was in protrusion, anti-protrusio cage was overlayed over the retained shell of size 56 (Fig. 2B). A DM cup of size 47 was cemented on this construct (Fig. 2c).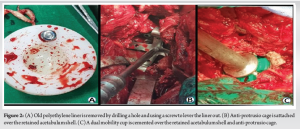
A Wagner stem of size 16 mm by 305 mm was used, and osteotomy closed using encerclage wires with an additional hook plate was used to further stabilize the osteotomy site. The patient was mobilized from the day of surgery, partial weight-bearing with the help of a walker. Intraoperative samples sent were negative. Post-operative DVT prophylaxis was started in the form of intermittent calf pumps and low molecular weight heparin.
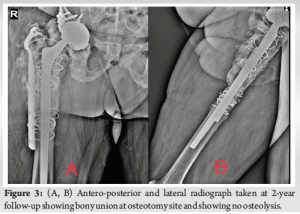
The patient was followed up at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year, till the last follow-up of 2 years. The patient was assessed clinically and radiographically at each follow-up. Clinically, the patient was asymptomatic until the last follow-up mobilized full weight-bearing without support, and had a Modified Harris Hip Score (HHS) of 79. Radiologically, there were no signs of loosening (Fig. 3).
Prevention of dislocation after THA remains a topic of debate. There are various surgical options to tackle hip instability, each with its own advantages and disadvantages. During revision, there is often bone loss and it may need augmentation by mesh, cages, or the use of megaprosthesis. In addition, multiple surgeries and tissue damage increase the instability of the hip. Here, we report a case where we have successfully addressed the problem faced during re-revision surgery. In our case, we have retained the acetabulum shell as it was found to be well-fixed and stable. As the acetabulum shell was in protrusio (Fig. 1), anti-protrusio cage was inserted over it to supplement the stability of our construct (Fig. 2B). Anti-protrusio cages are used to reconstruct severe acetabular bone deficiencies in revision hip replacement that are not amenable to reconstruction with porous-coated uncemented devices. The use of anti-protrusio cages associated with bone grafting in acetabular reconstructions is reliable because primary fixation and good secondary osteointegration are obtained despite substantial bone loss [11]. Due to the large surface area provided by cages, they can attach larger-sized shells, and multiple fixations can provide for biological fixation to the pelvis [11]. Schneider et al. [11] found a 10.4% rate of dislocation where a DM cup was cemented into anti-protrusio cages in a series of 96 patients in a mean follow-up of 41 months. The cemented fixation of DM cups in cages appears to be a good option. In a revision scenario with a well-fixed acetabulum component, adequate stability can be achieved by revising the modular components and cementing a liner, or constrained liner, or cemented cup, or DM cup (Double Socket Technique). Although the dislocation rates are reduced with constrained liners, they decrease the functional arc of motion and increase acetabular cup bone interface contact stress, leading to higher rates of acetabular loosening [4]. Khoury et al. [12] had a 23% failure rate with the use of constrained acetabular liners along with cages in 28-month follow-up of 16 patients. We used the Double Socket Technique where we cemented the DM cup in the anti-protrusio cage as various studies have shown a lower risk of subsequent dislocation, re-revision for dislocation, and reoperation using the DM cup. DM is an attractive option as the large head improves jump distance to dislocation, the impingement-free movement, and reduces contact stresses on the acetabular cup bone interface [6]. A recent study shows lower dislocation rates at the end of 4 years using DM cups cemented into acetabulum shell (double socket) than polyethylene liners [13]. The dislocation rate was 1% in the DM group and 12% in the polyethylene group [13]. In a retrospective study of 10 patients who underwent cementation of DM cup into the well-fixed cementless shell (double socket), the authors have found this a viable option to treat and prevent instability after revision THA without the use of constraint liners at the cement cup interface [14]. At a mean follow-up of 3.5 years, the dislocation rate was 10%, HHS score improved from 49.3 preoperatively to 71.3. Chalmers et al. [9] analyzed 18 patients who underwent cementation of DM cups in a well-fixed acetabulum (double socket) and found no dissociation of DM at the cement cup interface in their study. The authors have reported a post-operative dislocation rate of 17%. They recommended using this technique for recurrently dislocating THAs with well-fixed, well-positioned acetabular components and complex acetabular reconstructions in which constraints should be avoided. A recent retrospective study of 28 patients using the Double Socket Technique showed no dislocation, dissociation of the cemented DM cup construct, or aseptic loosening of the retained metal shell [10]. It ensures a straightforward and blood-sparing revision technique in frail patients with high surgical risk and/or older than their natural life expectancy [10]. To the best of our knowledge, this is the first case reported worldwide wherein the Double Socket Technique with retained acetabular shell was done along with an anti-protrusio cage in revision THA.
Fixation of the cage over a previously well-fixed acetabulum shell and cementation of the DM cup appears to be a reliable option in a patient with multiple prior revision surgeries. It helps shorten the surgical time and reduce the bone loss that can occur in extracting a well-fixed acetabulum shell. The use of a DM cup decreases the chances of instability compared to the cementation of polyethylene liners and decreases the high failure rate associated with the use of cementation of constrained liners. The addition of an anti-protrusio cage in addition to the Double Socket Technique increases the stability of the construct.
The Double Socket Technique, combining retained acetabular shell, anti-protrusio cage, and DM cup cementation, offers a novel and effective approach in revision scenarios demonstrating the potential benefits of reduced surgical time and bone loss that can occur while extracting a well-fixed acetabulum shell.
References
- 1.Parvizi J, Picinic E, Sharkey PF. Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-42. [Google Scholar | PubMed]
- 2.Carter AH, Sheehan EC, Mortazavi SM, Purtill JJ, Sharkey PF, Parvizi J. Revision for recurrent instability: What are the predictors of failure? J Arthroplasty 2011;26:46-52. [Google Scholar | PubMed]
- 3.Garbuz DS, Masri BA, Duncan CP, Greidanus NV, Bohm ER, Petrak MJ, et al. The frank stinchfield award: Dislocation in revision THA: Do large heads (36 and 40 mm) result in reduced dislocation rates in a randomized clinical trial? Clin Orthop Relat Res 2012;470:351-6. [Google Scholar | PubMed]
- 4.Della Valle CJ, Chang D, Sporer S, Berger RA, Rosenberg AG, Paprosky WG. High failure rate of a constrained acetabular liner in revision total hip arthroplasty. J Arthroplasty 2005;20:103-7. [Google Scholar | PubMed]
- 5.Agarwala S, Shetty V, Taywade S, Vijayvargiya M, Bhingraj M. Dual mobility THR: Resolving instability and providing near normal range of movement. J Clin Orthop Trauma 2021;13:40-5. [Google Scholar | PubMed]
- 6.Stucinskas J, Kalvaitis T, Smailys A, Robertsson O, Tarasevicius S. Comparison of dual mobility cup and other surgical construts used for three hundred and sixty two first time hip revisions due to recurrent dislocations: Five year results from Lithuanian arthroplasty register. Int Orthop 2018;42:1015-20. [Google Scholar | PubMed]
- 7.Beaulé PE, Ebramzadeh E, Le Duff M, Prasad R, Amstutz HC. Cementing a liner into a stable cementless acetabular shell: The double-socket technique. J Bone Joint Surg Am 2004;86:929-34. [Google Scholar | PubMed]
- 8.Young GH, Abdel MP, Amendola RL, Goetz DD, Lewallen DG, Callaghan JJ. Cementing constrained liners into secure cementless shells: A minimum 15-Year follow-up study. J Arthroplasty 2017;32:3480-3. [Google Scholar | PubMed]
- 9.Chalmers BP, Ledford CK, Taunton MJ, Sierra RJ, Lewallen DG, Trousdale RT. Cementation of a dual mobility construct in recurrently dislocating and high risk patients undergoing revision total arthroplasty. J Arthroplasty 2018;33:1501-6. [Google Scholar | PubMed]
- 10.Wegrzyn J, Saugy CA, Guyen O, Antoniadis A. Cementation of a dual mobility cup into an existing well-fixed metal shell: A reliable option to manage wear-related recurrent dislocation in patients with high surgical risk. J Arthroplasty 2020;35:2561-6. [Google Scholar | PubMed]
- 11.Schneider L, Philippot R, Boyer B, Farizon F. Revision total hip arthroplasty using a reconstruction cage device and a cemented dual mobility cup. Orthop Traumatol Surg Res 2011;97:807-13. [Google Scholar | PubMed]
- 12.Khoury JI, Malkani AL, Adler EM, Markel DC. Constrained acetabular liners cemented into cages during total hip revision arthroplasty. J Arthroplasty 2010;25:901-5. [Google Scholar | PubMed]
- 13.Brüggemann A, Mallmin H, Hailer NP. Do dual-mobility cups cemented into porous tantalum shells reduce the risk of dislocation after revision surgery? Acta Orthop 2018;89:156-62. [Google Scholar | PubMed]
- 14.Moreta J, Uriarte I, Foruria X, Urra I, Aguirre U, Martínez-de Los Mozos JL. Cementation of a dual-mobility cup into a well-fixed cementless shell in patients with high risk of dislocation undergoing revision total hip arthroplasty. HIP Int 2021;31:9-102. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report
August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report August 1, 2026 Short-term Outcomes of Impaction Bone Grafting Technique with a Collared Fully Hydroxyapatite-Coated Stem in Revision Total Hip Arthroplasty: A Case Series
August 1, 2026 Short-term Outcomes of Impaction Bone Grafting Technique with a Collared Fully Hydroxyapatite-Coated Stem in Revision Total Hip Arthroplasty: A Case Series August 1, 2026 Outcome of Large-Diameter Jumbo Cups or Acetabular Mesh with Impaction Bone Grafting for Acetabular Defects in Primary and Revision Total Hip Arthroplasty: A Case Series
August 1, 2026 Outcome of Large-Diameter Jumbo Cups or Acetabular Mesh with Impaction Bone Grafting for Acetabular Defects in Primary and Revision Total Hip Arthroplasty: A Case Series