
In adult patients with severe symptomatic spina bifida, arthrodesis may be a viable option for relieving pain and potentially permitting independent ambulation.
Mr. Austin Yu, Department of Orthopaedic Surgery, Rush University, Chicago, Illinois. E-mail: austin_yu@rush.edu
Abstract
Introduction: Spina bifida is a rare neurological condition that, if uncorrected, may cause chronic valgus knee stress difficulty with independent ambulation and significant pain. Current literature lacks comprehensive guidance on surgically correcting progressive hip and knee deformities in spina bifida patients, which include osteotomy and primary. When these options are contraindicated, alternative approaches such as arthrodesis may be indicated, although they remain understudied in this population
Case Report: A 47-year-old man presented with bilateral hip and knee pain. Radiographs demonstrated valgus knee deformities with severe arthrosis and bilateral femoral head subluxation. The patient had a history of spina bifida with chronic lower extremity weakness and neurogenic bladder. He underwent staged bilateral instrumented knee arthrodesis and staged bilateral total hip arthroplasty (THA).
Conclusion: This is the first reported case of bilateral instrumented knee arthrodesis in a patient with spina bifida. Orthopedic care of these patients is complex. Surgical correction of symptomatic knee and hip deformities through instrumented arthrodesis and THA may permit an improved functional outcome.
Keywords: Spina bifida, instrumented knee arthrodesis, total hip arthroplasty.
Spina bifida, a rare congenital malformation, results from failure of neural tube fusion during embryogenesis, resulting in lesions of the lumbosacral spine [1,2]. The goal of orthopedic management for patients with spina bifida is to correct musculoskeletal deformity during childhood. Kyphosis and scoliosis, common in these children, when addressed, may enhance overall function [3,4]. However, if they age without correction, severe lumbosacral symptoms often manifest in the lower extremities. Pelvic muscle imbalance may cause hip subluxation and dislocation, and in the knee, uncorrected valgus stress may induce osteoarthritis often with flexion-extension contractures [5]. The orthopedic literature lacks comprehensive guidance on surgically correcting progressive hip and knee deformities in spina bifida patients. While osteotomy and primary arthroplasty are viable options, caution arises due to poor bone quality, residual contractures, and muscular atrophy [5,6]. Consequently, alternative approaches like arthrodesis may be indicated, although they remain understudied in this population. This case report will expand upon the surgical correction of spina bifida patients who develop severe knee and hip symptoms.
DP, a 47-year-old male, presented to his primary care provider with 3 years of bilateral hip and knee pain. He had a significant history of spina bifida status-post serial neonatal casting, chronic neurogenic bladder, and severe lower extremity weakness and contractures. Initial knee radiographs revealed chronic deformities with significant joint space loss and functional knee effusions (Fig. 1). Plain films of the pelvis suggested bilateral dysplasia with complete hip dislocation (Fig. 2). Laboratory tests were within normal limits including a complete blood count, comprehensive metabolic panel, and urinalysis. He was prescribed extended-release naltrexone for pain management and referred to our tertiary medical center.

His physical examination revealed significant lower extremity atrophy. Sensation was intact to the mid-anterior tibial crest bilaterally but diminished distally. Distal pulses were intact and brisk bilaterally. Bilateral knee evaluation demonstrated full extension to 10° of flexion with active and passive range of motion. Active range of motion of the hips was limited to 10° of internal rotation, 15° of external rotation, and 20° of abduction and adduction. The patient was unable to plantarflex, dorsiflex, invert, or evert the ankles. Despite these challenges, he managed ambulation with a severely antalgic gait. The patient also received neurosurgical workup. Non-contrast magnetic resonance imaging of the spine revealed an osseous defect of the dorsal sacrum with tethered and low-lying conus medullaris at S2. Following a multidisciplinary discussion, it was decided that right-knee surgery was appropriate, with no emergent spinal intervention necessary. The patient was informed a total knee arthroplasty (TKA) would be challenging and prone to complications due to his severe limitations in flexion and quadriceps function. Any arthroplasty would have required a permanent drop-lock knee brace. Therefore, the decision was made to proceed with arthrodesis to give the patient a stable limb for ambulation. Intraoperatively, the right knee had significant scarring and atrophied muscle. Vastus medialis fibers were dissected proximally down to the knee joint and onto the subcutaneous tibia. Soft tissue attachments from the capsule and collateral ligaments were removed to visualize the distal femur for plating. A 5° valgus distal femur cut was made. The proximal tibia was exposed, and the posterior capsule was dissected. A tibial osteotomy perpendicular to the tibial axis was made, creating two opposable metaphyseal osteotomized surfaces with cuts orthogonal to the mechanical axis. A template was employed to contour an anterior proud 4.5 × 206 mm 11-hole locking plate (DePuy Synthes, Johnson and Johnson, Raynham, MA). The plate was inserted with two screws in the proximal segment and the articulated tensioning device was used to compress the osteotomy site. The construct was bolstered with four proximal and four distal screws. An additional 4.5 × 206 mm medial locking plate was contoured (Fig. 3a). The patient was made non-weight bearing for 8 weeks and discharged 4 days post-operatively after an uncomplicated hospital stay. At 3-month post-operatively, the patient had minimal pain and a considerably improved gait. Twelve months after the index procedure, he underwent uncomplicated instrumented arthrodesis of the left knee, with the same indication, operative technique, and methods of fixation (Fig. 3b).

Five months later, the patient underwent left total hip arthroplasty (THA) after failing conservative treatment. A posterolateral approach was used, revealing minimal abductor attachment to the proximal femur. The patient received a 50 mm G7 OsseoTi Acetabular Shell (Zimmer Biomet, Warsaw, IN), with four screws in multiple cup quadrants, placed at approximately 40° of inclination and 20° of anteversion. A G7 Dual Mobility CoCr liner (Zimmer Biomet) was impacted, and subsequent femoral components, including a size 15 Standard Offset Wagner Cone Prosthesis Stem (Zimmer Biomet) and a 28 mm, 3.5 mm offset Biolox Delta Femoral Head (Zimmer Biomet), were successfully implanted. A minor crack was observed at the proximal femoral neck during femoral component seeding, leading to the placement of a single Dall-Miles cable (Stryker, Kalamazoo, MI) distal to the crack (Fig. 4). The femoral stem remained stable, and the crack did not propagate. Six weeks of partial weight-bearing was advised due to limited acetabular bone stock. After 8 months, the patient underwent an uncomplicated right THA using a similar approach and implants except for a 28 mm, 0 mm offset Biolox Delta Femoral Head (Zimmer Biomet). At the most recent follow-up, 3.3 years after the index knee arthrodesis and 2.1 years after the index THA, the patient uses a manual wheelchair at baseline. While walking independently remains a challenge, he demonstrates the ability to wheel himself without difficulty. The patient’s bed transfers are independent, and he can stand with bilateral assistance. Complex activities of daily living require caregiver assistance. The patient is happy with his bilateral procedures, noting significantly reduced pain.
Spina bifida is a rare neurological condition that may progress to lower extremity deformities [5]. In the knees, this includes contractures, bony dysplasia, and valgus deformity from femoral mal-alignment, external tibial torsion, or pelvic muscle atrophy [2,7,8,9]. If left uncorrected, chronic valgus knee stress may render the adult spina bifida patient unable to independently ambulate without pain, similar to the current presentation. It is therefore essential to surveil these patients throughout adolescence to identify lower extremity symptoms that indicate progressive hip and knee deformity. Typically, surgical correction of lower extremity deformities in younger patients with spina bifida includes osteotomy, hamstring transfers, or quadricepsplasty [10-12]. For mild deformities, or when surgery is not feasible, serial casting may be of benefit [13,14]. When inadequately managed, patients with spina bifida often develop hip and knee symptoms emerging in adulthood. This case underscores arthrodesis as a viable option for relieving pain and potentially permitting independent ambulation. Although knee arthrodesis is seldom described for this purpose, ankle arthrodesis stands as a comparable procedure for managing spina bifida-related ankle deformities and has demonstrated functional improvement [7,15]. In the general orthopedic literature, knee arthrodesis primary addresses pain and instability following prior TKA. In rarer instances, it addresses metaphyseal bone loss, inadequate ligamentous or soft-tissue coverage, extension mechanism loss, or infection precluding an implant [16,17]. Classic contraindications to knee arthrodesis – ipsilateral hip/ankle osteoarthropathy, contralateral hip/knee osteoarthropathy, contralateral knee amputation, as well as difficulties ambulating post-operatively – derive from the arthroplasty literature [18]. To our knowledge, bilateral arthrodesis has never been attempted in a patient with spina bifida. In this case, while a custom-hinged or constrained TKA was initially contemplated, severe muscle imbalance and contractures would have necessitated a lifelong drop-lock brace for ambulation. We also envisioned challenges in obtaining flexion to implant arthroplasty hardware. This would have required extensor mechanism take down and reattachment, increasing the risk of future extensor mechanism disruption. Consequently, arthrodesis was chosen. Multiple techniques exist for knee arthrodesis, commonly employing rigid internal fixation with a nail [19]. Cementation, external fixation, plating, or hybrid methods involving nails, plates, and external fixation are also employed [19,20]. Instrumented arthrodesis with plating was selected in this case due to the patient’s minimal knee motion, limited extension/flexion, and significant hip dysplasia. Long intramedullary nailing’s implications for future THAs were also considered. All knee arthrodesis methods carry a significant risk of complications, including nonunion, peroneal nerve palsy, infection, thrombophlebitis, and stress fractures at the arthrodesis site [16,20]. However, we believe that these risks were mitigated by meticulous surgical technique, resulting in clinical success over a 3-year follow-up period. Furthermore, our threshold for iatrogenic neuropraxia was underscored by the patient’s minimal baseline function in the peroneal distribution.
In summary, we describe a patient with severe osteoarthropathy of the knees and hips secondary to spina bifida, who was successfully treated surgically with bilateral, staged instrumented arthrodesis, followed by bilateral, staged THA. Although this current patient now is a minimal ambulator at baseline due to other medical comorbidities, his overall level of pain is much improved post-operatively. We highlight the importance of this surgical technique in a unique patient cohort to alleviate pain and dysfunction and to inform orthopedists of an acceptable option when encountering spina bifida patients in clinical practice.
Staged instrumented arthrodesis may be recommended for highly symptomatic lower extremities in adults with spina bifida. Typically, surgical correction for lower extremity deformities in younger patients with spina bifida includes osteotomy, hamstring transfers, or quadricepsplasty. However, these options may not be viable in cases of severe muscle atrophy and contracture as in this case. While arthrodesis commonly addresses pain and instability following prior TKA, it may also be used to relieve lower extremity pain in severe cases of spina bifida.
References
- 1.Feeley BT, Ip TC, Otsuka NY. Skeletal maturity in myelomeningocele. J Pediatr Orthop 2003;23:718-21. [Google Scholar | PubMed]
- 2.Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, et al. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol 2010;88:1008-16. [Google Scholar | PubMed]
- 3.Centers for Disease Control and Prevention (CDC). Racial/ethnic differences in the birth prevalence of spina bifida-United States, 1995-2005. MMWR Morb Mortal Wkly Rep 2009;57:1409-13. [Google Scholar | PubMed]
- 4.Selber P, Dias L. Sacral-level myelomeningocele: Long-term outcome in adults. J Pediatr Orthop 1998;18:423-7. [Google Scholar | PubMed]
- 5.Jobe AH. Fetal surgery for myelomeningocele. N Engl J Med 2002;347:230-1. [Google Scholar | PubMed]
- 6.Sutton LN. Fetal surgery for neural tube defects. Best Pract Res Clin Obstet Gynaecol 2008;22:175-88. [Google Scholar | PubMed]
- 7.Drennan JC. The role of muscles in the development of human lumbar kyphosis. Dev Med Child Neurol Suppl 1970;22 Suppl 22:33-8. [Google Scholar | PubMed]
- 8.Asher M, Olson J. Factors affecting the ambulatory status of patients with spina bifida cystica. J Bone Joint Surg Am 1983;65:350-6. [Google Scholar | PubMed]
- 9.Westcott MA, Dynes MC, Remer EM, Donaldson JS, Dias LS. Congenital and acquired orthopedic abnormalities in patients with myelomeningocele. Radiographics 1992;12:1155-73. [Google Scholar | PubMed]
- 10.Swaroop VT, Dias L. Orthopedic management of spina bifida. Part I: Hip, knee, and rotational deformities. J Child Orthop 2009;3:441-9. [Google Scholar | PubMed]
- 11.Dias LS, Jasty MJ, Collins P. Rotational deformities of the lower limb in myelomeningocele. Evaluation and treatment. J Bone Joint Surg Am 1984;66:215-23. [Google Scholar | PubMed]
- 12.Dias L. Orthopaedic care in spina bifida: Past, present, and future. Dev Med Child Neurol 2004;46:579. [Google Scholar | PubMed]
- 13.Vankoski S, Moore C, Statler KD, Sarwark JF, Dias L. The influence of forearm crutches on pelvic and hip kinematics in children with myelomeningocele: Don’t throw away the crutches. Dev Med Child Neurol 1997;39:614-9. [Google Scholar | PubMed]
- 14.Lim R, Dias L, Vankoski S, Moore C, Marinello M, Sarwark J. Valgus knee stress in lumbosacral myelomeningocele: A gait-analysis evaluation. J Pediatr Orthop 1998;18:428-33. [Google Scholar | PubMed]
- 15.Dippe K, Parsch K. Die behandlung der kniegelenkdeformität bei spina bifida [Treatment of knee joint deformities in spina bifida]. Helv Paediatr Acta 1978;33:205-10. [Google Scholar | PubMed]
- 16.Marshall PD, Broughton NS, Menelaus MB, Graham HK. Surgical release of knee flexion contractures in myelomeningocele. J Bone Joint Surg Br 1996;78:912-6. [Google Scholar | PubMed]
- 17.Dias LS. Surgical management of knee contractures in myelomeningocele. J Pediatr Orthop 1982;2:127-31. [Google Scholar | PubMed]
- 18.Damron TA, McBeath AA. Arthrodesis following failed total knee arthroplasty: Comprehensive review and meta-analysis of recent literature. Orthopedics 1995;18:361-8. [Google Scholar | PubMed]
- 19.Spiro AS, Babin K, Lipovac S, Rupprecht M, Meenen NM, Rueger JM, et al. Anterior femoral epiphysiodesis for the treatment of fixed knee flexion deformity in spina bifida patients. J Pediatr Orthop 2010;30:858-62. [Google Scholar | PubMed]
- 20.Conway JD, Mont MA, Bezwada HP. Arthrodesis of the knee. J Bone Joint Surg Am 2004;86:835-48. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study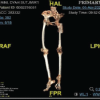 June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review
June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review June 1, 2026 A Case of Bilateral Steroid Arthropathy of the Hip Following Repeated Intra-articular Steroid Injections
June 1, 2026 A Case of Bilateral Steroid Arthropathy of the Hip Following Repeated Intra-articular Steroid Injections June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report
June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report