
We report a case and described a technique to manage a rare presentation of pure distal PT rupture without an avulsion fracture. Our technique was unique and based on using knotless anchors with FiberTape® sutures. To the best of our knowledge, this technique has never been used before in such injury and anatomical location. At two years of follow-up, the patient is free of complaints with almost full ROM at the knee and back to his standard daily life activity.
Dr. Razan Mohammed Alotaibi, Division of Orthopedics, Department of Surgery, King Abdullah Bin Abdulaziz University Hospital, Riyadh, Saudi Arabia. E-mail: razzanalotaibi@gmail.com
Abstract
Introduction: The extensor mechanism and patellar tendon (PT) are considered essential components. Adult PT avulsion from the tibial tubercle is uncommon, with little information in the literature. Technical challenges arise during injury management. Knotless anchors have several applications in treating tendon injuries, such as the rotator cuff, distal biceps, and quadriceps tendons but were not used to repair distal PT avulsions.
Case Report: A 50-year-old male patient, an active adult, presented to emergency department with significant right knee pain, giving away and limitation of range of motion (ROM) that had started after he sustained direct trauma with a ground-level fall on his knee that morning.
Conclusion: In this paper, we report a case and describe a technique to manage a rare presentation of pure distal PT rupture without an avulsion fracture using knotless anchors with FiberTape®, which showed excellent results. To the best of our knowledge, this technique has never been used before in such injury and anatomical location. At 2 years of follow-up, the patient is free of complaints with almost full ROM at the knee and back to his standard daily life activity.
Keywords: Anchors, patellar tendon, spontaneous rupture.
The patellar tendon (PT) is an essential component of the extensor mechanism. Its rupture, in general, is considered a rare injury. However, it is an extensively disabling injury and usually requires surgical repair [1,2]. It mostly occurs in the younger population, especially those under 40 and highly active athletes [3,4]. Several predisposing factors have been linked to causing spontaneous rupture of PT, including steroid or fluoroquinolone use, rheumatoid arthritis, systemic lupus erythematosus, metabolic disorders, and diabetes mellitus [1,5,6]. Typically, the vast majority of the PT ruptures are observed at its origin in the inferior pole of the patella or at its insertion in the tibial tubercle. Usually, it will be associated with an avulsion fracture of either the inferior patella or tibial tubercle [2,7,8]. Nevertheless, cases describing spontaneous rupture of PT at distal insertion are limited [3,9,10]. After an extensive literature review, we found only one case report of pure spontaneous distal PT rupture without any associated avulsion fracture that occurred in the absence of a systemic cause [5]. This case aimed to demonstrate a rare presentation of PT rupture in adult males, report a unique surgical technique, and evaluate the outcome of using FiberTape® in fixing pure distal PT rupture. It occurred spontaneously at its insertion on the tibial tubercle without significant trauma. There was no avulsion fracture associated with it. In this case, surgical treatment led to a complete resolution of the patient’s symptoms. We used two knotless anchors with a non-absorbable FiberTape® suture. To the best of our knowledge, it has never been used to fix PT rupture at the distal insertion. Moreover, highlights of our unique surgical technique are mentioned in this report.
A 50-year-old male patient, an active adult, presented to our emergency department with significant right knee pain, giving away and limitation of range of motion (ROM) that had started after he sustained direct trauma with a ground-level fall on his knee that morning. Moreover, he had no history of any chronic medical illness except chronic kidney disease managed with a renal transplant, and was not involved in any competitive sports activity. He denied any history of previous knee injury or complaints. In addition, he was not using any form of antibiotics. However, he was on continuous immunosuppressant agents (cyclosporine) and steroids after his renal transplant surgery for 7 years. At present, he is on a small dose of steroids (5 mg). Upon examination, mild swelling with ecchymosis was observed around the knee. There was no open wound, joint line tenderness, or joint effusion around the knee. The extensor mechanism was disrupted, and a high-ridding patella was noticed. The maximum point of tenderness was provoked over the PT insertion with a palpable defect, specifically at the tibial tubercle. No tenderness was elicited over the patella or quadriceps tendon. The patient had a decreased ROM in his right knee, which ranged between 30 and 80 flexions. All other ligaments, including anterior cruciate ligament, posterior cruciate ligaments, and collaterals, were intact by examination. Moreover, his distal neurovascular structures were intact and the popliteal artery was palpable. A plain radiograph of the right knee revealed a high-riding patella (patella alta) without any avulsion fracture or bony abnormalities (Fig. 1). Moreover, the patella alta was confirmed by the decrease in the Insall Salvati ratio, which was about 1.95 (Fig. 2).
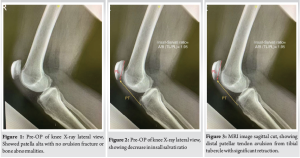
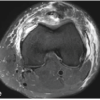
A magnetic resonance imaging scan showed complete avulsion of the distal attachment of the PT from the tibial tuberosity with retraction of the PT about 2.8 cm (Fig. 3). The patient was informed about his condition and treatment plan. He provided consent for the publication of the case.
The patient was supine for surgery, with a standard operating table with all bony prominences well padded. A tourniquet around the thigh was used. The skin was incised along the midline of the knee joint and moved slightly medial to avoid the incision lying directly anterior. It was approximately 5 cm in length. Starting from the center of the patella and downward to the tibial tubercle (Fig. 4).
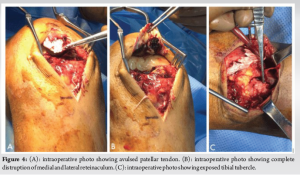
Dissection through the subcutaneous tissues was performed until the tibial tubercle was reached, and all intra-articular structures were evaluated. After that, the insertion site of the PT, specifically at the tibial tubercle, was identified and the retracted PT was held from the distal part. Using a non-absorbable FiberTape® (Arthrex, Naples, USA) sutures to run over the PT and to secure it (Fig. 5).
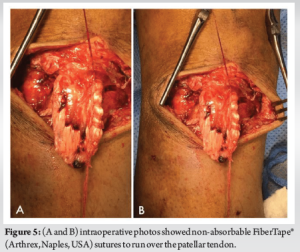
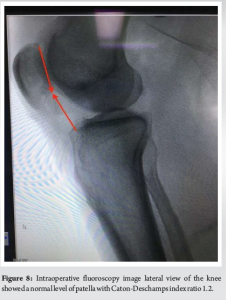
Suturing was done by locking suture technique over the two edges of PT, starting from the distal ends and up to the proximal part of PT and fashioned in a Krackow whipstitch suturing method. Notably, the sutures were tied while the knee was almost fully extended. Moreover, about 1.5 cm was left at the distal end of PT to leave space for its fixation inside the tibial tuberosity. Then, the footprint of the tibial tuberosity was mildly debrided with a curette to make a rough surface to enhance healing. Two knotless anchors, 4.5 (PEEK SwiveLock® C-Vented, Arthrex), were placed at the distal edge of the footprint. One medial and the other one lateral to the tibial tuberosity, with a 1 cm space between them to avoid unintentional fractures (Fig. 6). A running locking suture was done from each anchor with the adjacent retinaculum sides (Fig. 7). The stability of the repair was then checked through the knee ROM and skin closure followed (Fig. 8).

The patient was kept in a knee immobilizer with full knee extension for 6 weeks and allowed to bear weight on his right knee as tolerated. His recovery was uneventful, and he was discharged on the 3rd-day post-surgery. Regarding post-operative protocol, the knee immobilizer was kept for 6 weeks. Then, he gradually started knee flexion (active and active assisted) under the supervision of a physical therapist. 2 years post-surgery, the patient had full knee ROM and it was stable on both varus and valgus stress tests without extensor mechanism deficiency (Fig. 9). His patella was in place and was confirmed radiographically (Fig. 10).


In general, PT rupture occurs due to forceful and sudden eccentric contraction of the extensor mechanism of the knee, especially in athletes, where the knee is fixed in flexion while landing or falling [11,12]. Most of the PT ruptures occur at the inferior pole of the patella and are mostly associated with an avulsion fracture. Pure PT rupture without an avulsion fracture at either the patella or the tibial tuberosity is an extremely rare injury [3,5,7,10,13]. However, the spontaneous occurrence of the distal site PT rupture, without avulsion fracture in our patient, was unique in comparison with the ruptures reported previously [1-13]. Typically, surgical repair of the PT ruptures is the prevailing treatment method. Although several surgical methods have been described in the literature, there is a deficiency in relation to the repair methods in pure avulsed distal end PT rupture [9-11]. Practically, managing avulsed PT rupture without a fracture at the insertion site poses difficulties considering the negligible soft-tissue remnant for repair and its location. Moreover, the anatomy of the PT differs at its distal end as the PT becomes narrower and thicker substantially [9,14]. Furthermore, knowing that this rupture was a tendinopathy associated mostly with steroid use. Our technique was conceived to address and manage these problems and achieve the desired outcomes of proper fixation and optimal knee function. Several surgical fixation techniques have been used for fixing a ruptured tendon in various anatomic sites, including transosseous tunnels and suture anchors. However, both techniques showed comparable outcomes in strength and load to failure in various biomechanical studies [9,15,16]. In our patient, we decided to repurpose knotless anchors with non-absorbable FiberTape® sutures, usually used in other tendon fixation surgeries such as quadriceps, biceps, and rotator cuff tendons. Different biomechanical studies suggested that fixing tendons with knotless anchors was stronger and stiffer [17-19]. As it has a higher load at clinical failure, lesser slippage, and the highest stiffness compared to all other constructs. We believe using knotless anchors will provide further fixation strength since it will expand the contact area and minimize the contact pressure at the repair site. In addition, it will add extra strength to the fixation by tightly sealing the tendon over the footprint. Using FiberTape®, which is an ultra-high molecular weight polyethylene with a braided cover of polyester tape, showed better long-term durability as it has a low probability of stretching throughout the years. Moreover, its greater thickness provides an enhanced interference fit between the bone and anchor.
In conclusion, we described a technique to manage a rare presentation of pure distal PT rupture without an avulsion fracture. Our technique was unique and based on using knotless anchors with FiberTape® sutures. To the best of our knowledge, this technique has never been used before in such injury and anatomical location. At 2 years of follow-up, the patient is free of complaints with almost full ROM at the knee and back to his standard daily life activity.
Knotless anchors showed excellent results in the fixation of pure distal PT rupture.
References
- 1.Kasten P, Schewe B, Maurer F, Gösling T, Krettek C, Weise K. Rupture of the patellar tendon: A review of 68 cases and a retrospective study of 29 ruptures comparing two methods of augmentation. Arch Orthop Trauma Surg 2001;121:578-82. [Google Scholar | PubMed]
- 2.Zernicke RF, Garhammer J, Jobe FW. Human patellar-tendon rupture. J Bone Joint Surg Am 1977;59:179-83. [Google Scholar | PubMed]
- 3.Cooper ME, Selesnick FH. Partial rupture of the distal insertion of the patellar tendon: A report of two cases in professional athletes. Am J Sports Med 2000;28:402-6. [Google Scholar | PubMed]
- 4.Siwek, CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am 1981;63:932-7. [Google Scholar | PubMed]
- 5.Chloros GD, Razavi A, Cheatham SA. Complete avulsion of the patellar tendon from the tibial tubercle in an adult without predisposing factors. J Orthop Sci 2014;19:351-3. [Google Scholar | PubMed]
- 6.Stinner DJ, Orr JD, Hsu JR. Fluoroquinolone-associated bilateral patellar tendon rupture: A case report and review of the literature. Mil Med 2010;175:457-9. [Google Scholar | PubMed]
- 7.Matava MJ. Patellar tendon ruptures. J Am Acad Orthop Surg 1996;4:287-96. [Google Scholar | PubMed]
- 8.Enad JG. Patellar tendon ruptures. South Med J 1999;92:563-6. [Google Scholar | PubMed]
- 9.Galos DK, Konda SR, Kaplan DJ, Ryan WE, Alaia MJ. Transosseous-equivalent repair for distal patellar tendon avulsion. Arthrosc Techn 2016;5:e385-9. [Google Scholar | PubMed]
- 10.Capogna B, Strauss E, Konda S, Dayan A, Alaia M. Distal patellar tendon avulsion in association with high-energy knee trauma: A case series and review of the literature. Knee 2017;24:468-76. [Google Scholar | PubMed]
- 11.Kaneko K, Miyazaki H, Yamaguchi T. Avulsion fracture of the tibial tubercle with avulsion of the patellar ligament in an adolescent female athlete. Clin J Sport Med 2000;10:144-5. [Google Scholar | PubMed]
- 12.Agarwalla A, Puzzitiello R, Stone AV, Forsythe B. Tibial tubercle avulsion fracture with multiple concomitant injuries in an adolescent male athlete. Case Rep Orthop 2018;2018:1070628. [Google Scholar | PubMed]
- 13.Di Giacomo LM, Khan MS, Bisaccia M, Rende R, Rinonapoli G, Caraffa A. Surgical repair of an atraumatic avulsion of patellar tendon at the tibial tuberosity in an adult patient. Case Rep Orthop 2015;2015:192023. [Google Scholar | PubMed]
- 14.Benjamin M, Toumi H, Ralphs JR, Bydder G, Best TM, Milz S. Where tendons and ligaments meet bone: Attachment sites (“entheses”) in relation to exercise and/or mechanical load. J Anat 2006;208:471-90. [Google Scholar | PubMed]
- 15.Lighthart WA, Cohen DA, Levine RG, Parks BG, Boucher HR. Suture anchor versus suture through tunnel fixation for quadriceps tendon rupture: A biomechanical study. Orthopedics 2008;31:441-1. [Google Scholar | PubMed]
- 16.Park MC, Cadet ER, Levine WN, Bigliani LU, Ahmad CS. Tendon-to-bone pressure distributions at a repaired rotator cuff footprint using transosseous suture and suture anchor fixation techniques. Am J Sports Med 2005;33:1154-9. [Google Scholar | PubMed]
- 17.Cox JT, Shorten PL, Gould GC, Markert RJ, Barnett MD Jr., Laughlin RT. Knotted versus knotless suture bridge repair of the Achilles tendon insertion: A biomechanical study. Am J Sports Med 2014;42:2727-33. [Google Scholar | PubMed]
- 18.Kindya MC, Konicek J, Rizzi A, Komatsu DE, Paci JM. Knotless suture anchor with suture tape quadriceps tendon repair is biomechanically superior to transosseous and traditional suture anchor-based repairs in a cadaveric model. Arthroscopy 2017;33:190-8. [Google Scholar | PubMed]
- 19.Burkhart SS, Denard PJ, Konicek J, Hanypsiak BT. Biomechanical validation of load-sharing rip-stop fixation for the repair of tissue-deficient rotator cuff tears. Am J Sports Med 2014;42:457-62. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Bilateral Patellar Tendon and Unilateral Syndesmotic Injury in a Recreational Athlete
July 1, 2026 Bilateral Patellar Tendon and Unilateral Syndesmotic Injury in a Recreational Athlete April 1, 2026 Neglected Ruptures of the Patellar Tendon: Report of Three Cases in the Orthopedic Trauma Department of Dalal Jamm Hospital, Dakar
April 1, 2026 Neglected Ruptures of the Patellar Tendon: Report of Three Cases in the Orthopedic Trauma Department of Dalal Jamm Hospital, Dakar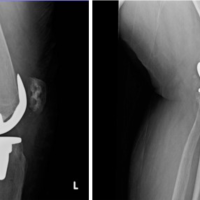 December 10, 2022 A Unique Patellar Tendon Rupture and Small Tibial Avulsion fracture in a Post-Menopausal Patient
December 10, 2022 A Unique Patellar Tendon Rupture and Small Tibial Avulsion fracture in a Post-Menopausal Patient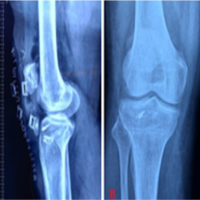 November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report
November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report