
This article will enable learners about the novel approach to assess the severity of knee osteoarthritis.
Dr. Arun Kumar K V Associate Professor in Department of Orthopedics, Chettinad academy of Research and Education, Rajiv Gandhi Salai, Kelambakkam - 603 103, Chengalpattu District, Chennai, Tamil Nadu, India. Email: arun5684@gmail.com
Abstract
Introduction: Conventional radiography has always been cited as the gold standard for assessing the structural changes associated with osteoarthritis (OA) of the knee. The purpose of the study was to compare the joint space width between both leg-standing and one-leg-standing radiographs in an assessment of the severity of OA of the knee.
Materials and Methods: Fifty patients with medial compartment OA were deployed for the study. Patients underwent both leg standing radiographs and one-leg standing radiograph on the affected leg. Kellgren–Lawrence (KL) radiographic classification was used to assess the severity of OA using joint space width.
Conclusion: The mean medial joint space width decreased from 3.26 mm in both legs of the standing radiograph to 1.98 mm in the one-leg standing radiograph. Patients on both leg standing radiographs appreciated an increase in grade during the single leg radiograph. Nearly 52% of patients with both leg standing radiographs have changed the KL grading to a more severe grade when undergone a single leg standing radiograph. One-leg standing radiograph was found to be a better representation of joint space width than both-leg standing radiographs.
Keywords: Knee osteoarthritis, imaging, one-leg standing radiography, both leg standing radiography.
Osteoarthritis (OA) is one of the most common manifesting forms of arthritis and has been described as a degenerative joint disease or “wear and tear” arthritis [1]. Accompanied by varying degrees of functional limitations and decreased quality of life. Globally, it affects around 500 million people, which constitutes around 7% of the world’s population [2]. It is the second most commonly occurring rheumatologic problem, with a prevalence ranging from 22% to 39% in India [3]. Eighty percent of people above 75 years and older suffer from OA. The pathology begins with the breaking down of the cartilage within a joint, and changes take place in the underlying bone, which are usually chronic and get worse over time. It causes pain, decreased or limited joint mobility, and swelling in some. On clinical examinations, patients present with crepitus, bony enlargement, periarticular tenderness, muscle weakness, reduced volume of movements, and instability. The structural changes are characterized by the presence of osteophyte formation, subchondral cysts, reduced hyaline cartilage, subchondral osteosclerosis, synovial thickening, and inflammation. Rather than clinical manifestation, the diagnosis of OA has been pre-dominantly based on radiographic appearances. Radiographic assessment has been primarily used for skeletal changes, and these radiographic changes have been codified into the 5-point Kellgren-Lawrence (KL) grading scale, which is ubiquitous in OA clinical research [4-6]. For assessing the structural changes associated with OA, conventional radiography has always been cited as the gold standard. Narrow joint space measurement radiography has been the method of choice in assessing cartilage loss, while other radiographic findings include the presence of subchondral cysts, subchondral osteosclerosis, and osteophytes [7]. Weight-bearing knee radiographs have better outcomes compared to supine radiographs in the evaluation of joint space [8]. The standing anteroposterior (AP) is the preferred technique where the knees are in an extended and weight-bearing position. Recently, one-leg standing radiograph has been found to have effective compartmental loading in the stance phase of the gait and to derange the KL grades I and II recorded to KL grades III and IV, which warrants immediate surgery rather than treating KL grades I and II in a conservative manner. Inaccurate assessment of the joint space has been found to postpone clinical decision-making. The purpose of the current study was to evaluate the severity of joint space narrowing and KL grading between one-leg and both leg standing radiographs in the primary compartment OA of the knee. (Fig. 2 and 3).
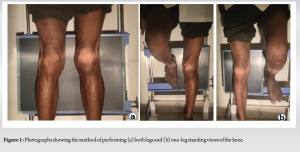
After getting approval from the Ethics Committee, Institutional Review Board, and Chettinad Health and Research Institute, the study was conducted from a time period between June to August 2023 at the Orthopedics Departments, Chettinad Health and Research Institute, Chennai. Totally 50 patients—100 knees—diagnosed with primary medial compartment knee OA by the American College of Rheumatology clinical criteria and with symptoms of bilateral knee pain. Among the selected patients with medial knee pain, the selection criteria include at least three of the following six criteria: anterior or medial joint line tenderness, had exhibited crepitus, bony enlargement, no palpable warmth of the synovium, stiffness lasting more than 30 min, and above 50 years. The exclusion criteria included patients who could not bear weight on one-leg, previous history of knee injury who underwent surgery, valgus OA, and any form of inflammatory arthritis. All patients underwent digital radiographs of both knees (Fig. 1a). The AP radiographs for both legs were performed in full extension with equal weight bearing on both legs. While performing a one-leg standing radiograph, the patient was instructed to stand on the affected leg while elevating the contralateral leg (Fig. 1b). KL classification was used to grade the severity of OA knee. The medial and lateral joint space widths were recorded, and two independent orthopedic surgeons assessed the reliability of the measurements with two measurements taken at a monthly interval. The chi-square test and paired t-test were used for the parametric data and the Mann–Whitney U test for non-parametric data. SPSS version 25 was used for statistical analysis.
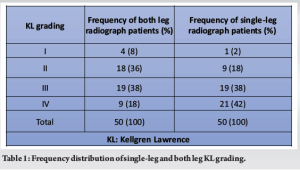
Of the 50 patients, 25 were males and 25 were females. The mean age was 62 years (the standard deviation [SD] was 5.2), and the minimum and maximal age were 52 years and 70 years, respectively. The mean body mass index was 26.48 kg/m2 (SD 3.56). With the standard two-leg standing view, it was found that 8% were at KL grade I, 36% at KL grade II, 38% at KL grade III, and 18% at KL grade IV (Table 1). The mean single leg tibiofemoral angle was measured to be 3.52° (SD 0.82°), while for both leg tibiofemoral angles measured, it was 3.37° (SD 1.11°) (P = 0.23).
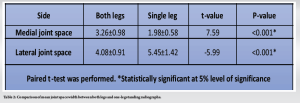
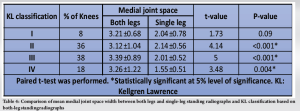
The mean medial joint space width decreased from 3.26 mm in both legs of the standing radiograph to 1.98 mm in the one-leg standing radiograph, while the mean lateral joint space width increased from 4.08 mm in both legs of the standing radiograph to 5.45 mm in the one-leg standing radiograph (Table 2). Table 3 showed that based on KL grading, most of the patients on both leg standing radiographs showed an increased severity in grading classification in single leg radiographs. 13 patients in grade 2 in both leg radiographs were classified into grades 3 and 4 in single leg radiographs, and 10 patients in grade 3 in both leg radiographs were classified as grade 4 in single leg radiographs. There were three patients in grade 1 in both legs who moved up to grade 2 and 3 in single-leg KL grading. However, there were nine patients classified as grade 4 in a single-leg radiograph who were not classified in both leg KL grading. Statistical significance (p<0.001) was only appreciated for association between KL classification grade 2 and 3 with medial joint space width for both single and both legs standing radiography (Table 4).


OA is considered the most prevalent joint disease and has been on the rise in an aging society with a paramount health and economic impact. In defiance of its growing prevalence, OA is still an underrecognized chronic ailment since it does not result in mortality despite its significant effect on morbidity and quality of life. Research data reveals that one in seven adults has OA, and more than 50% (18.7 million) of those with OA are of working age. The annual medical costs are around $65.5 billion, with average per person per year medical expenses costing $2018 [9]. OA is more common in women than men, and 45% of women above the age of 65 have symptoms, and 70% over 65 have radiological evidence. It was estimated to be the 10th leading cause of non-fatal burden [10,11]. According to global burden disease [3], in 2000, it was found to be the fourth leading cause of years lived with disability, accounting for 3%. Radiography is basically a two-dimensional projection of a three-dimensional joint structure, which is considered the gold standard for assessing associated structural changes in OA. Radiograph image variations depend on joint positioning in space, which is essential since variations in measurement alter the grading of the condition and change in the modality of treatment. Misdiagnosis among patients with OA based on joint space width in both leg standing radiographs (from mild to moderate rather than severe OA) has delayed the surgical intervention. This misdiagnosis has been overcome in the present study in assessing the severity of knee OA by evaluating joint space narrowing, which is found to be cost-effective considering other diagnostic options such as magnetic resonance imaging (MRI) and its easy practicability. In patients with knee OA, radiographic joint space measurements are found to be reliable and constitute cartilage erosion [12,13]. In the present study, it was found that increased KL grading in one-leg compared to both legs standing radiograph in KL staging I to III and not in stage IV. This implies the fact that standing on both legs does not make the patient to bear their full weight on the affected knee, leading to errors in the evaluation of joint space width and cartilage. Slight flexion of the knee might contribute to narrow joint space in a one-leg standing radiograph. A 7° to 10° flexion weight bearing provided more accurate narrowing of joint space measurement than Lyon Schuss and both knee extension views [14]. A one-leg standing radiograph provides more accurate joint space measurement among mild to moderate OA patients with good inter- and intra-observer reliability but only represents the distal articulating surface. To increase better accuracy, Rosenberg et al. [15] preferred the 45° posteroanterior (PA) knee flexion weight-bearing technique, which provides good accuracy and anteroposterior view in evaluating joint space narrowing. Fewer studies have suggested a 30° PA knee flexion weight-bearing view in assessing joint space narrowing [16,17]. Piperno et al. [18] in their study, which compared three radiographic views for evaluating medial compartment OA, found that the lowest joint space width was appreciated in the 30° knee flexion PA view, followed by one-leg AP standing in full extension view, and both legs standing in full extension view. However, in our study, we preferred the one-leg standing radiograph over the knee flexion weight-bearing technique, as the latter technique was felt to be difficult to control angle and maintain flexion among OA patients.
The one-leg radiograph is not possible to be taken for all patients. Elderly patients with severe knee pain and those who are unable to stand on one-leg are not ideal candidates for single-leg radiography. For patients whose weight bearing is not possible for other reasons, standing radiography is the choice of diagnostic investigation. The posterior femoral condyle articulation cannot be evaluated with this technique since this technique permits to assess only distal femoral articulation in the standing position due to full extension. Clinical correlation may be needed to plan for treatment for patients in whom standing radiographs with decreased joint space may not represent the actual severity of knee pain in OA.
Even though MRI has been the best diagnostic tool for direct visualization of ligaments, meniscus, bone, and cartilage, conventional radiography is still considered the gold standard for assessing knee OA in clinical and epidemiological settings. In conclusion, nearly 52% of patients with both leg standing radiographs have changed the KL grading to a more severe grade when undergone a single-leg standing radiograph, indicating the need for early intervention leading to better and earlier patient recovery. Moreover, it was also appreciated that one-leg standing radiograph was found to be a better representation of knee alignment and joint space width than both leg standing radiographs in the management of OA.
This study will enable treating doctors in early diagnosing the severity of knee OA by using single-leg radiography instead of conventional two-leg radiography. And by this, the treatment modality can be started in an earlier phase, and patients can be treated at the primitive level itself.
References
- 1.Available from: https://www.cdc.gov/arthritis/basics/osteoarthritis.htm. Accessed January 15,2024 [Google Scholar | PubMed]
- 2.Available from: https://www.medicalnewstoday.com/articles/prevalence-of-osteoarthritis. Accessed January 17,2024 [Google Scholar | PubMed]
- 3.Symmons D, Mathers C, Pfleger B. Global Burden of Osteoarthritis in Year 2000: Global Burden of Disease 2000 Study. World Health Report. Vol. 5., Version 2; 2002. [Google Scholar | PubMed]
- 4.Culvenor AG, Engen CN, Oiestad BE, Engebretsen L, Risberg MA. Defining the presence of radiographic knee osteoarthritis: A comparison between the Kellgren and Lawrence system and OARSI atlas criteria. Knee Surg Sports Traumatol Arthrosc 2015;23:3532-9. [Google Scholar | PubMed]
- 5.Sheehy L, Cooke TD. Radiographic assessment of leg alignment and grading of knee osteoarthritis: A critical review. World J Rheumatol 2015;5:69-81. [Google Scholar | PubMed]
- 6.Wright RW. Osteoarthritis classification scales: Interobserver reliability and arthroscopic correlation. J Bone Joint Surg Am 2014;96:1145-51. [Google Scholar | PubMed]
- 7.Georgiev T, Stoilov R, Penkov M, Ivanova M, Trifonov A. Radiographic assessment of knee osteoarthritis. Revmatologiia (Bulgaria) 2016;24(2): 16-24 [Google Scholar | PubMed]
- 8.Leach RE, Gregg T, Siber FJ. Weight-bearing radiography in osteoarthritis of the knee. Radiology 1970;97:265-8. [Google Scholar | PubMed]
- 9.Available from: https://www.cdc.gov/arthritis/docs/oaagenda2020.pdf. Accessed January 17,2024 [Google Scholar | PubMed]
- 10.Akinpelu AO, Alonge TO, Adekanla BA, Odole AC. Prevalence and pattern of symptomatic knee osteoarthritis in Nigeria: A community-based study. Internet J Allied Health Sci Pract 2009;7:3. [Google Scholar | PubMed]
- 11.Solomon L, Beighton P, Lawrence JS. Rheumatic disorders in the South African Negro. Patrt II. Osteo-arthrosis. S Afr Med J 1975;49:1737-40. [Google Scholar | PubMed]
- 12.Ravaud P, Giraudeau B, Auleley GR, Chastang C, Poiraudeau S, Ayral X, et al. Radiographic assessment of knee osteoarthritis: Reproducibility and sensitivity to change. J Rheumatol 1996;23:1756-64. [Google Scholar | PubMed]
- 13.Reichmann WM, Maillefert JF, Hunter DJ, Katz JN, Conaghan PG, Losina E. Responsiveness to change and reliability of measurement of radiographic joint space width in osteoarthritis of the knee: A systematic review. Osteoarthritis Cartilage 2011;19:550-6. [Google Scholar | PubMed]
- 14.Buckland-Wright JC, Wolfe F, Ward RJ, Flowers N, Hayne C. Substantial superiority of semiflexed (MTP) views in knee osteoarthritis: A comparative radiographic study, without fluoroscopy, of standing extended, semiflexed (MTP), and schuss views. J Rheumatol 1999;26:2664-74. [Google Scholar | PubMed]
- 15.Rosenberg TD, Paulos LE, Parker RD, Coward DB, Scott SM. The forty-five-degree posteroanterior flexion weight-bearing radiograph of the knee. J Bone Joint Surg Am 1988;70:1479-83. [Google Scholar | PubMed]
- 16.Guermazi A, Roemer FW, Burstein D, Hayashi D. Why radiography should no longer be considered a surrogate outcome measure for longitudinal assessment of cartilage in knee osteoarthritis. Arthritis Res Ther 2011;13:247. [Google Scholar | PubMed]
- 17.Vignon E, Piperno M, Le Graverand MP, Mazzuca SA, Brandt KD, Mathieu P, et al. Measurement of radiographic joint space width in the tibiofemoral compartment of the osteoarthritic knee: Comparison of standing anteroposterior and Lyon schuss views. Arthritis Rheum 2003;48:378-84. [Google Scholar | PubMed]
- 18.Piperno M, Le Graverand MP, Conrozier T, Bochu M, Mathieu P, Vignon E. Quantitative evaluation of joint space width in femorotibial osteoarthritis: Comparison of three radiographic views. Osteoarthritis Cartilage 1998;6:252-9. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Effect of Intraarticular Platelet-Rich Plasma Injection in Knee Osteoarthritis
August 1, 2026 The Effect of Intraarticular Platelet-Rich Plasma Injection in Knee Osteoarthritis August 1, 2026 Comparative Efficacy of Intra-Articular Growth Factor Concentrate and Platelet-Rich Plasma Injections in Knee Osteoarthritis: An Evaluation of Clinical, Radiological, and Biomarker Outcomes
August 1, 2026 Comparative Efficacy of Intra-Articular Growth Factor Concentrate and Platelet-Rich Plasma Injections in Knee Osteoarthritis: An Evaluation of Clinical, Radiological, and Biomarker Outcomes August 1, 2026 Arthroscopic Repair of Meniscal Medial Root Tears: The Necessity of Concomitant Realignment Osteotomy
August 1, 2026 Arthroscopic Repair of Meniscal Medial Root Tears: The Necessity of Concomitant Realignment Osteotomy July 1, 2026 Efficacy of Intra-articular Growth Factor Concentrate in Knee Osteoarthritis: A Randomized Controlled Trial
July 1, 2026 Efficacy of Intra-articular Growth Factor Concentrate in Knee Osteoarthritis: A Randomized Controlled Trial