
To describe a novel finding in routine hand surgery, and to promote the importance anatomical knowledge and surgeon inventiveness in non-routine cases.
Mr. William F McCormick, Research Fellow, Department of Orthopaedic Surgery, University of Alabama at Birmingham, 1313 13th St. S, Birmingham, AL 35205, USA. E-mail: wilmccormick@augusta.edu
Abstract
Introduction: Incidental discovery of anomalous muscles and anatomical variants within the forearm and wrist through surgical exposure and advanced imaging techniques is relatively common.
Case Report: The patient presented with pain and swelling in her hand that was refractory to rest and anti-inflammatory medications. Here, we describe the intraoperative discovery of an anatomical variant of the flexor carpi radialis (FCR), as well as an anomalous flexor carpi radialis brevis (FCRB) in a 58-year-old patient being treated for thumb carpometacarpal joint (CMCJ) arthritis.
Conclusion: To the best of our knowledge, this is the first description of both anomalies within a single patient and the first use of the surgical technique, described here, in treating the patient’s thumb CMCJ arthritis. This report reinforces the importance of meticulous dissection and identification of individual anatomy to optimize patient outcomes.
Keywords: Hand, tendon, surgery, anatomy.
The flexor carpi radialis brevis (FCRB) was first described in 1851 by Fano in his cadaveric studies, and later given the name FCRB vel profundus by Woods in 1867 [1,2]. Its prevalence at this time was found to be roughly 14 of every 347 cases, or 4%, by Le Double and Macalister [3]. The muscle described originated from the volo-radial border of the distal radius, just distal to the origin of the FPL, and coursed distally outside of the carpal tunnel, inserting into the base of the second, third, or fourth metacarpals. Although not clinically relevant at the time, advances in modern surgical technique involving the wrist and hand have restored interest in this seemingly rare anomalous muscle. Since 2006, there have been 16 published articles to our knowledge describing the FCRB and its clinical implications. Andring et al. found the estimated prevalence of the FCRB to be somewhere between 2 and 8% [4]. Although rarely associated with symptoms [4], the FCRB is subject to incidental discovery during surgical approaches to the volar forearm and wrist, most notably the FCR approach to the wrist for volar plating of distal radius fractures, and as described in our case, FCR tendon harvest for thumb CMCJ arthroplasty. With this in mind, it is imperative that hand and wrist surgeons are aware of this anatomical anomaly to be comfortable during routine surgical exposure and effectively treat their patients. Although anatomical variants of the FCR have been documented, to the best of our knowledge, no previous studies have described the FCR tendon inserting into the palmar fascia.
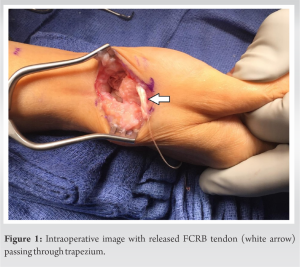
A 58-year-old right-hand-dominant female presented to the clinic complaining of a 1-year history of non-traumatic right hand and thumb pain and swelling. She reported worsening pain with activity, particularly with typing and gripping. The patient found minimal relief of pain with non-steroidal anti-inflammatory drugs. A physical examination revealed mild swelling and tenderness to palpation of the right thumb carpometacarpal joint (CMCJ) with crepitus. The grind test was positive. Sensation was intact to light touch distally, with capillary refill less than two seconds. Her range of motion was not limited, with full extension and flexion intact. Radiographs revealed a chronic-appearing trapezium fracture with thumb CMCJ arthritis. The patient received a corticosteroid injection and was placed in a thumb spica splint. She returned to the clinic 6 weeks later, endorsing approximately 3 weeks of relief following her injection, but the pain had since returned despite compliance with her thumb spica splint. After the risks and benefits of surgical and non-surgical management were discussed with the patient, she decided to proceed with surgical treatment. The patient was taken to the operating room for right thumb CMCJ arthroplasty with flexor carpi radialis (FCR) tendon transfer. Using a longitudinal incision over the radial thumb base, the thumb CMCJ was exposed with identification and protection of the radial sensory nerve and radial artery. After the trapezium was identified, fully dissected, and excised, the FCR tendon was visualized and found to be intact and in its usual position. Next, 3 1 cm transverse incisions were made on the volar wrist and forearm for FCR tendon harvesting. The tendon was divided proximally and brought distally into the thumb wound. At that time, it was found that this tendon did not continue and insert at the base of the index metacarpal. Instead, the harvested tendon merged with the radial palmar fascia. With further dissection at the wrist crease incision, another tendon was discovered deep to the FCR that continued distally beneath the transverse carpal ligament. In addition, this tendon was found to have a muscle belly coming from the distal radius (Fig. 1) and was assumed to be the flexor carpi radialis brevis (FCRB). The functions of these two tendons were tested with tensioning, which showed wrist flexion without thumb motion for the FCR and wrist flexion and radial deviation without thumb motion for the FCRB. Deep to the FCRB, the flexor pollicis longus (FPL) was identified and found to be functioning properly through tensioning. Given the irregular insertion of the FCR, it was decided that using the FCRB tendon for suspensionoplasty and harvesting the FCR tendon for interposition was the best approach. The FCRB tendon was excised at its proximal myotendinous junction and brought into the thumb wound. Using a freer elevator, the tendon was dissected all the way to its insertion on the index finger metacarpal base and was found to be the original tendon visualized following trapeziectomy. In addition, no tendon was found superficial to the FCRB, reaffirming our initial finding of anomalous FCR insertion into the palmar fascia (Fig. 2). After a bone tunnel was created through the thumb metacarpal base, the FCRB tendon was retrieved from a volar-ulnar to a dorsal-radial direction and secured with a biotenodesis screw. After the stable suspension was confirmed, the harvested FCR tendon was then placed into the space between the thumb MC and scaphoid, serving as an interpositional graft. The wound was then irrigated, and the capsule was closed with 4-0 vicryl suture. After skin closure and deflation of the tourniquet, a brisk capillary refill was noted in all fingers, and the patient was placed in a thumb spica splint. The patient experienced mild post-operative edema and an increase in pain at her 1-month follow-up visit after a fall at home. Otherwise, her recovery was uneventful, and her pain and edema improved over the course of 3 months with continued physical therapy and conservative management. Six months following surgery, her incision was well-healed with painless full range of motion, no tenderness to palpation, and no patient complaints. Table 1.
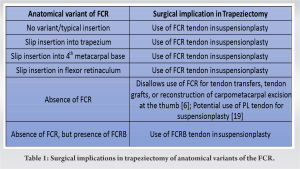
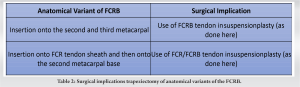
This case report describes and illustrates the unique anatomy of a woman with persistent thumb pain who was successfully treated with an interpositional graft. The FCRB in this case report was unique due to its anomalous insertion point. In comparison to the native wrist, where the FCR inserts at the bases of the second and third metacarpals [5,6]. The most common insertional variant is a small slip inserting onto the trapezium, but slips onto the fourth metacarpal base and into the flexor retinaculum may also be found. The origin of the FCR may have multiple variants as well, including slips from the biceps brachii, the brachialis, the ulnar coronoid process, and the radius at the anterior oblique line [7]. Some cases have even reported the absence of the FCR [6,8], including a case by Irie et al., which reports the absence of the FCR but the presence of an FCRB [8]. Among cases of FCRB specifically, many FCR tendons insert normally onto the second and third metacarpal. However, the FCRB often inserts into the FCR tendon sheath, running parallel with the FCR tendon and creating an anomalous shared insertion onto the second metacarpal base [9-11]. The FCR tendon serves as an important anatomical landmark in several procedures performed on the volar aspect of the distal upper extremity [12]. Therefore, awareness of possible anatomical variants is essential to safely performing these procedures and avoiding iatrogenic injury to soft tissues and surrounding neurovascular structures. Table 2. Surgical intervention for osteoarthritis of the CMC joint is indicated in cases of persistent pain or joint instability refractory to conservative management, and a variety of operative techniques have been described. Trapeziectomy, or excisional arthroplasty, may be utilized in combination with or without interposition. In this procedure, the trapezium is resected either partially or completely. Interposition consists of harvesting part of the FCR tendon with preservation of the distal insertion on the base of the second metacarpal, followed by transfer and folding of the transected tendon within the void left by the removed trapezium. Although this technique can be effective for pain relief, it does not address joint laxity and has been associated with weakened pinch strength and instability [12,13]. To address this shortcoming, excisional arthroplasty with interposition may be combined with suspension arthroplasty or ligament reconstruction, both of which entail stabilization of the first metacarpal by the harvested FCR tendon [13].
In ligament reconstruction, as described by Burton and Pellegrini, the trapezium is excised and the FCR tendon is harvested to the metacarpal base as previously described. The transected tendon is then passed through a hole drilled at the base of the first metacarpal and secured. This creates a sling between the first and second metacarpal, which provides support and prevents subluxation of the first [14]. After pulling the FCR tendon through the hole, the remainder may then be folded for interposition [15]. In traditional suspensionplasty as described by Weilby, the harvested FCR tendon is wrapped around the abductor pollicis longus (APL) and FCR rather than passed through the first metacarpal for stabilization [16]. However, several variants of suspensionplasty have been developed. Other commonly used techniques for the treatment of CMCJ arthritis include carpometacarpal arthrodesis, joint replacement, metacarpal osteotomy, and volar ligament reconstruction [17]. Although appropriate technique may be at the surgeon’s discretion based on patient- and pathology-specific factors [12], trapeziectomy with interposition and ligament reconstruction is the most commonly performed operation for CMCJ osteoarthritis in the United States [18].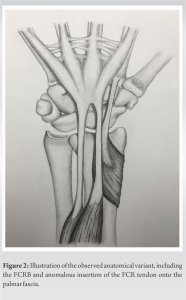
The goal of trapeziectomy with interposition and suspensionplasty as performed in our patient is to provide symptomatic relief through removal of diseased bone while maintaining strength, motion, and functionality of the hand and distal forearm. Although the FCR tendon is typically used for suspensionplasty, the anatomical variant in this patient presented a unique challenge to performing the procedure in its traditional context. Due to its anomalous insertion into the radial aspect of the palmar fascia, the harvested FCR was in close proximity to the void of the trapezium. The FCRB tendon, however, inserted on the base of the second metacarpal in a manner similar to an anatomically normal FCR tendon, making it a viable graft choice for suspensionplasty. Interposition prevents subsidence, and suspensionplasty provides subluxation of the first metacarpal, both of which contribute to improved patient outcomes and prevention of complications. Therefore, it was determined to be in the best interest of the patient to utilize the FCRB tendon for suspensionplasty and the FCR for interposition to maximize post-operative stability and functionality, regardless of deviation from the traditional technique.
While there are many known common anomalous slip insertions of the FCR tendon, the tendon will most commonly still proceed to attach to the second and third metacarpals where it can be used as an anchor in suspensionplasty. Research has shown that in the instance of a ruptured FCR, the palmaris longus tendon [19], as well as the abductor pollicis longus [20] can be used in suspensionplasty and produce similar outcomes. This once again emphasizes the importance of anatomical knowledge, observation, and resourcefulness in the operating room, as there are various effective alternative techniques when an irregularity prohibits any given one.
This unique case of FCRB and FCR with anomalous insertion onto the palmar fascia highlights the notion that a multitude of anatomical variants may be encountered when utilizing a volar approach in hand and wrist surgeries. Surgeons should remain observant when using this approach and take care to carefully dissect and identify individual anatomy to effectively perform procedures, prevent iatrogenic injury, and optimize patient outcomes.
In the instance of anomalous flexor carpi radialis insertion, other tendons including a flexor carpi radialis brevis when present, can be harvested and utilized for suspensionplasty, resulting in a pain-free wrist.
References
- 1.Wood J. On human muscular variations and their relation to comparative anatomy. J Anat Physiol 1867;1:44-59. [Google Scholar | PubMed]
- 2.Lee YM, Song SW, Sur YJ, Ahn CY. Flexor carpi radialis brevis: An unusual anomalous muscle of the wrist. Clin Orthop Surg 2014;6:361-4. [Google Scholar | PubMed]
- 3.Carleton A. Flexor carpi radialis brevis vel profundus. J Anat 1935;69:292-3. [Google Scholar | PubMed]
- 4.Andring N, Kennedy SA, Iannuzzi NP. Anomalous forearm muscles and their clinical relevance. J Hand Surg Am 2018;43:455-63. [Google Scholar | PubMed]
- 5.Bishop AT, Gabel G, Carmichael SW. Flexor carpi radialis tendinitis. Part I: Operative anatomy. J Bone Joint Surg Am 1994;76:1009-14. [Google Scholar | PubMed]
- 6.Sofos SS, Riaz M. Absence of flexor carpi radialis during an elective carpometacarpal arthroplasty of the thumb: A rare anatomical variation. Case Rep Med 2016;2016:7853487. [Google Scholar | PubMed]
- 7.Bergman RA, Afifi AK, Miyauchi R. Flexor Carpi Radialis. Illustrated Encyclopedia of Human Anatomic Variation. Available from: https://www.anatomyatlases.org/anatomicvariants/muscularsystem/text/f/05flexor.shtml [Last accessed on Mar 2024]. [Google Scholar | PubMed]
- 8.Irie T, Motomiya M, Iwasaki N. Absence of flexor carpi radialis identified during volar approach for fixation of distal radius fracture: A case report. BMC Res Notes 2018;11:240. [Google Scholar | PubMed]
- 9.Mantovani G, Lino W, Fukushima WY, Cho AB, Aita MA. Anomalous presentation of flexor carpi radialis brevis: A report of six cases. J Hand Surg 2009;35:234-5. [Google Scholar | PubMed]
- 10.Dodds SD. A flexor carpi radialis brevis muscle with an anomalous origin on the distal radius. J Hand Surg Am 2006;31:1507-0. [Google Scholar | PubMed]
- 11.Chong SJ, Al-Ani S, Pinto C, Peat B. Bilateral flexor carpi radialis brevis and unilateral flexor carpi ulnaris brevis muscle: Case report. J Hand Surg Am 2009;34:1868-71. [Google Scholar | PubMed]
- 12.Matullo KS, Ilyas A, Thoder JJ. CMC arthroplasty of the thumb: A review. Hand (N Y) 2007;2:232-9. [Google Scholar | PubMed]
- 13.Jones DB Jr., Rhee PC, Shin AY, Kakar S. Salvage options for flexor carpi radialis tendon disruption during ligament reconstruction and tendon interposition or suspension arthroplasty of the trapeziometacarpal joint. J Hand Surg Am 2013;38:1806-11. [Google Scholar | PubMed]
- 14.Burton RI, Pellegrini VD Jr. Surgical management of basal Joint arthritis of the thumb. Part II. Ligament reconstruction with tendon interposition arthroplast. J Hand Surg Am 1986;11:324-32. [Google Scholar | PubMed]
- 15.Johnson J, Goitz RJ. Ligament reconstruction and tendon interposition. Oper Tech Orthop 2018;28:16-22. [Google Scholar | PubMed]
- 16.Weilby A. Tendon interposition arthroplast of the first carpo-metacarpal joint. J Hand Surg Br Eur 1988;13:421-5. [Google Scholar | PubMed]
- 17.Vermeulen GM, Slijper H, Feitz R, Hovius SE, Moojen TM, Selles RW. Surgical management of primary thumb carpometacarpal osteoarthritis: A systematic review. J Hand Surg Am 2011;36:157-69. [Google Scholar | PubMed]
- 18.Yuan F, Aliu O, Chung KC, Mahmoudi E. Evidence-based practice in the surgical treatment of thumb carpometacarpal joint arthritis. J Hand Surg Am 2017;42:104-12.e1. [Google Scholar | PubMed]
- 19.Kawamura D, Funakoshi T, Iwasaki N. Trapeziectomy with ligament reconstruction and interposition arthroplasty using the palmaris longus tendon: An average 5-year follow-up. Clin Orthop Surg 2019;11:453-8. [Google Scholar | PubMed]
- 20.Soejima O, Hanamura T, Kikuta T, Iida H, Naito M. Suspensionplasty with the abductor pollicis longus tendon for osteoarthritis in the carpometacarpal joint of the thumb. J Hand Surg Am 2006;31:425-8. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center
June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center June 1, 2026 Acute Calcific Periarthritis of the 1st Metacarpophalangeal Joint: A Rare Diagnostic Challenge
June 1, 2026 Acute Calcific Periarthritis of the 1st Metacarpophalangeal Joint: A Rare Diagnostic Challenge April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients
April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients November 1, 2025 Case Study and Literature Review: Patient-Controlled Opioid-Free Surgical Pathway for Right Total Hip Arthroplasty
November 1, 2025 Case Study and Literature Review: Patient-Controlled Opioid-Free Surgical Pathway for Right Total Hip Arthroplasty