
Comprehensive evaluation of traumatic injuries should consider underlying congenital anomalies, emphasizing the importance of understanding both the anatomy and function of complex skeletal structures to inform treatment decisions effectively.
Dr. Mainak Roy, Department of Orthopaedics, All India Institute of Medical Sciences, Mahindra Bloomdale, Tower 1B, Room 505, 5th Floor, MIHAN, Nagpur - 441 108, Maharashtra, India. E-mail: mainakroy30@gmail.com
Abstract
Introduction: Congenital radioulnar synostosis (CRUS) is a rare condition characterized by the fusion of the radius and ulna bones in the forearm, resulting in limited forearm rotational movement.
Case Report: We present a unique case of a 26-year-old male who suffered a forearm injury following a road traffic accident. Initial evaluation revealed a malformed proximal radius and distal radioulnar joint, and the presence of radioulnar synostosis, along with a fracture at the junction of the radius and ulna. Open reduction internal fixation was performed, followed by structured rehabilitation. At 6-month follow-up, significant improvement in forearm motion was observed, enabling the patient to perform daily activities independently.
Conclusion: This case underscores the importance of comprehensive evaluation in traumatic injuries and understanding the anatomy and function of the forearm complex. It also highlights the efficacy of surgical intervention and rehabilitation in restoring function and quality of life for patients with this rare condition. This report contributes to the limited literature on managing fractures in the context of CRUS and emphasizes the need for further research in this area.
Keywords: Radioulnar synostosis, fracture fixation, road traffic accident, surgical intervention.
Congenital radioulnar synostosis (CRUS) is a rare condition where the proximal ends of the radius and ulna bones are fused [1]. Although uncommon, it is frequently seen in congenital elbow abnormalities, with around 60–80% of cases affecting both upper extremities [2]. This condition limits forearm rotation and can severely impact daily activities. It is attributed due to developmental issues in utero, particularly during the period when the radius and ulna are forming between the 5th and 8th weeks of pregnancy [3]. The exact cause is believed to be a combination of genetic factors and multifactorial [1]. While most patients do not experience pain or restrictions in elbow movements, they typically present with fixed pronation of the forearm, and the ability to supinate is usually compromised to varying degrees [4]. Here, we present a very rare case of fracture in CRUS with malformed distal radioulnar joint (DRUJ) and proximal radius which was treated with internal fixation and lead to good return of function and bony healing. To the best of our knowledge, this is the first case reported of this kind in the medical literature.
A 26-year-old male presented to the emergency department with complaints of severe pain and deformity in his left forearm following a road traffic accident. Initial evaluation revealed tenderness and crepitus in the mid-shaft of the forearm. X-rays revealed a malformed proximal radius and a malformed DRUJ with radioulnar synostosis. In addition, a nondisplaced fracture was observed at the radioulnar synostosis (Fig. 1).
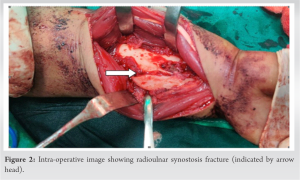
The patient claimed to have near complete pronation and supination before injury. The reason could have been due to the lack of development of the proximal radius and the DRUJ, resulting in essentially one solid bone in the forearm. The contralateral forearm was also examined and an X-ray was obtained. It was found to be normally developed both clinically and radiographically. No similar deformity was noted in any other limb. After obtaining informed consent, the patient agreed to undergo surgery. The volar approach was taken. The fracture was exposed, without extra difficulty (Fig. 2).
Open reduction internal fixation, using a 3.5 mm reconstruction plate bent intra-operatively to match the contour of the synostosis segment, was done (Fig. 3). Immediate post-operative X-ray showed satisfactory synostosis fracture reduction with implant (Fig. 4).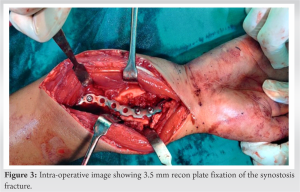
Post-operative course
Following surgery, the patient was placed on a structured rehabilitation program under the supervision of a physiotherapist. An above elbow splint was applied immediately post-operatively and the patient was allowed finger and hand movements until suture removal. After suture removal, the splint was removed and passive and active range of motion exercises were started as tolerated, including gentle supination and pronation. Passive and active-assisted range of motion exercises were initiated early to promote optimal functional recovery. The patient was followed up frequently at regular intervals.

At 6-month follow-up, the patient demonstrated significant improvement in forearm movement, with restoration of near-normal range of motion (Fig. 5). He was able to perform activities of daily living independently. The fracture showed successful union on radiological imaging at 6-month follow-up.

The forearm is a complex structure responsible for enabling the rotation of the hand and facilitating the redistribution of forces during various activities. This functionality is crucial for tasks requiring dexterity and manipulation. Any disruption or abnormality in the components of the forearm can potentially lead to limitations in its rotation and overall function [5]. CRUS is a rare condition characterized by the fusion of the radius and ulna bones in the forearm [2]. It is believed to result from an anomaly in the longitudinal segmentation process during early fetal development [1]. This fusion typically occurs bilaterally, affecting both arms and often follows an autosomal dominant inheritance pattern [6]. In addition, CRUS is often seen in conjunction with other malformation syndromes associated with chromosomal abnormalities. Researchers suggest a genetic basis for CRUS, evidenced by its familial occurrence and its association with various congenital syndromes. These include conditions such as acrocephalosyndactyly, microcephaly, Apert’s syndrome, Carpenter’s syndrome, and others [7]. Such evidence indicates that CRUS may be linked to broader genetic anomalies affecting skeletal development. One notable aspect of CRUS is that it often goes undiagnosed in early childhood. This is because children can adapt and compensate for the limited rotational capabilities caused by the fused forearm bones [8]. While movements such as pronation and supination are restricted, flexion and extension of the elbow are usually preserved. Patients with CRUS commonly rely on overuse and compensation from the shoulder and wrist joints to perform daily activities [4]. Despite these adaptations, individuals with CRUS may experience challenges in certain tasks, particularly those requiring intricate hand movements. These are two types of surgical procedures described: Operations aimed at improving the rotation of the forearm by removing fused bones (synostosis resection), sometimes using natural or synthetic materials to separate them, and operations intended to correct the fixed position of the forearm [9]. The goal of these surgeries is to bring the forearm back to its normal alignment, thus maintaining its natural movement [10]. Our case highlights a unique encounter where the patient adapted well to his forearm rotation limitations before the traumatic incident and had minimal impact on his daily activities. As a result, we made the decision of fixing the synostosis surgically. The patient was having considerable difficulties in doing his activities of daily living, hence definitive, stable fixation was considered a better treatment option. CRUS is itself a rare occurrence and a fracture at the same place that underwent fixation to achieve a good functional outcome is not yet documented in the medical literature.
This case offers several valuable lessons. First, it emphasizes the importance of a thorough evaluation of traumatic injuries, as underlying congenital anomalies may influence treatment decisions. Second, it highlights the significance of understanding the anatomy and function of the forearm complex, particularly in the context of rare conditions like CRUS. Third, it underscores the potential for adaptation and compensation in individuals with CRUS, which may mask the condition until a traumatic event reveals its presence. In addition, this case demonstrates the effectiveness of surgical intervention and structured rehabilitation in restoring function and quality of life for patients with CRUS.
Our case study of a 26-year-old male who experienced a forearm injury following a road traffic accident highlights the importance of thorough evaluation in traumatic injuries, understanding forearm anatomy, and the effectiveness of surgical intervention with rehabilitation in restoring function. This report contributes to the understanding of managing fractures in the context of CRUS, emphasizing the need for further research in this area.
References
- 1.Siemianowicz A, Wawrzynek W, Besler K. Congenital radioulnar synostosis-case report. Pol J Radiol 2010;75:51-4. [Google Scholar | PubMed]
- 2.Lescault E, Mulligan J, Williams G. Congenital radioulnar synostosis in an active duty soldier: Case report and literature review. Mil Med 2000;165:425-8. [Google Scholar | PubMed]
- 3.Sachar K, Akelman E, Ehrlich MG. Radioulnar synostosis. Hand Clin 1994;10:399-404. [Google Scholar | PubMed]
- 4.Kasten P, Rettig O, Loew M, Wolf S, Raiss P. Three-dimensional motion analysis of compensatory movements in patients with radioulnar synostosis performing activities of daily living. J Orthop Sci Off J Jpn Orthop Assoc 2009;14:307-12. [Google Scholar | PubMed]
- 5.LaStayo PC, Lee MJ. The forearm complex: Anatomy, biomechanics and clinical considerations. J Hand Ther 2006;19:137-45. [Google Scholar | PubMed]
- 6.Rizzo R, Pavone V, Corsello G, Sorge G, Neri G, Opitz JM. Autosomal dominant and sporadic radio-ulnar synostosis. Am J Med Genet 1997;68:127-34. [Google Scholar | PubMed]
- 7.A MECOM Variant in an African American Child with Radioulnar: Clinical Dysmorphology. Available from: https://journals.lww.com/clindysmorphol/citation/2018/01000/a_mecom_variant_in_an_african_american_child_with.4.aspx [Last accessed on 2024 Feb 25]. [Google Scholar | PubMed]
- 8.Yang ZY, Ni JD, Long Z, Kuang LT, Tao SB. Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: A case report and review of literature. World J Clin Cases 2020;8:1538-46. [Google Scholar | PubMed]
- 9.Barrera-Ochoa S, Campillo-Recio D, Mir-Bullo X. Treating bilateral congenital radioulnar synostosis using the reverse Sauvé-Kapandji procedure. J Hand Surg Eur Vol 2019;44:430-2. [Google Scholar | PubMed]
- 10.VanHeest AE, Lin TE, Bohn D. Treatment of blocked elbow flexion in congenital radioulnar synostosis with radial head excision: A case series. J Pediatr Orthop 2013;33:540-3. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Fracture Fixation Sequencing in Polyskeletal Trauma: Clinical Experience from a Five-Patient Retrospective Series
July 1, 2026 Fracture Fixation Sequencing in Polyskeletal Trauma: Clinical Experience from a Five-Patient Retrospective Series June 1, 2026 Comparison of Surgical Outcomes and Perioperative Laboratory Parameters Following Minimally Invasive Plate Osteosynthesis versus Conventional Plating in Long Bone Fractures
June 1, 2026 Comparison of Surgical Outcomes and Perioperative Laboratory Parameters Following Minimally Invasive Plate Osteosynthesis versus Conventional Plating in Long Bone Fractures May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing
May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing May 1, 2026 Anterior Bridge Plate Through Minimally Invasive Approach: A Game-changer for Humeral Shaft Fracture: A Clinical Case Series
May 1, 2026 Anterior Bridge Plate Through Minimally Invasive Approach: A Game-changer for Humeral Shaft Fracture: A Clinical Case Series