
This rare case of bilateral Galeazzi fractures with dorsal displacement, unclassified by the Walsh system, was successfully managed with ORIF using LCDCP. Spontaneous DRUJ realignment and early mobilization led to excellent 1-year functional outcomes.
Dr. Amit Chaudhari, Sportsmed, Parel, Mumbai-400025, Maharashtra, India. E-mail: dramitschaudhari@gmail.com
Abstract
Introduction: This case report presents an exceptionally rare occurrence of bilateral Galeazzi fractures with dorsal displacement of both distal radius fragments and the distal ulna in a 39-year-old male following a high-impact motorcycle accident. This specific injury configuration, which has not been categorized within the Walsh system, was effectively managed through open reduction and internal fixation utilizing limited contact dynamic compression plates.
Case Report: Fracture reduction was achieved using a bilateral Henry’s approach, which resulted in spontaneous realignment of the distal radioulnar joints without requiring supplementary stabilization. Intraoperative stability was evaluated using the piano key test, and post-operative immobilization with above-elbow back slabs supported optimal recovery.
Conclusion: At the 1-year follow-up, the patient demonstrated full functional recovery, including complete forearm range of motion and excellent grip strength. This case emphasizes the importance of prompt surgical management, precise anatomical realignment, and individualized intraoperative assessment in treating complex and rare bilateral forearm fractures. It also highlights the potential for excellent recovery outcomes with early and accurate intervention.
Keywords: Bilateral Galeazzi fractures, dorsal displacement, rare, open reduction internal fixation, limited contact dynamic compression plate, functional recovery.
A Galeazzi fracture is characterized by a fracture of the distal third of the radius accompanied by either dislocation or subluxation of the distal radioulnar joint (DRUJ) [1-4]. While uncommon, these injuries represent approximately 3% of forearm fractures in children and up to 7% in adults [5]. First described by Sir Ashley Cooper in 1833, Riccardo Galeazzi later reported 18 cases in 1934 [4]. These fractures typically occur due to high-energy trauma, such as motor vehicle accidents or falls, where axial loading and rotational forces impact the forearm. Due to the complex anatomy of the DRUJ, Galeazzi fractures can be overlooked, particularly in cases where joint disruption is subtle [10]. Precise anatomical restoration of both the radius and DRUJ is crucial to regaining normal forearm function. In adults, non-surgical treatment has led to unsatisfactory outcomes in up to 80% of cases, reinforcing the necessity of surgical management [6]. This report outlines a rare instance of bilateral Galeazzi fractures with dorsal displacement of both the distal radius and ulna fragments – an injury pattern not previously included in the Walsh classification system.
A 39-year-old male presented to the emergency department after being involved in a high-speed motorcycle collision. He was thrown from his motorcycle, landing on both outstretched arms. He reported severe pain, swelling, and deformity in both forearms. Despite the extent of his injuries, he remained hemodynamically stable and had no neurovascular deficits in either limb. On physical examination, gross deformities and tenderness were observed over both distal radii. Radiographs confirmed bilateral Galeazzi fractures with dorsal displacement of the distal radius and ulna fragments, a pattern not previously classified in the Walsh system [7] (Fig. 1).

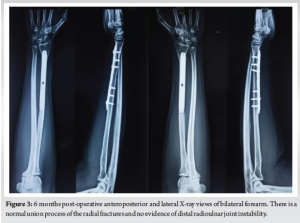
Initial management included bilateral above-elbow splints and intravenous analgesia. Following a detailed discussion with the patient, surgical intervention was planned. Open reduction and internal fixation (ORIF) was performed bilaterally under general anesthesia using a standard Henry’s approach. Both fractures were stabilized using 7-hole limited contact dynamic compression plates (LCDCPs). During surgery, anatomical fracture reduction led to spontaneous DRUJ realignment, confirmed intraoperatively through the piano key test. Fluoroscopy verified proper alignment (Fig. 2). Postoperatively, the patient was immobilized in supination with above-elbow back slabs. Three weeks later, controlled range-of-motion exercises for the wrist, elbow, and shoulder were initiated. Follow-up radiographs showed satisfactory healing. At 1 year, the patient achieved full bony union and functional recovery, scoring 95 on the Mayo wrist score.
Galeazzi fractures occur due to axial compression combined with rotational forces acting on the wrist [10]. The radius, being the primary load-bearing bone in the forearm, is particularly susceptible to fractures under these conditions. Disruption of the DRUJ occurs due to tension imbalances in the triangular fibrocartilage complex, a key stabilizing structure [1]. High-impact trauma, such as motorcycle accidents, is a frequent cause of these injuries. The transition zone between the radial shaft’s thick cortical bone and the thinner metaphyseal bone predisposes this region to fractures [2]. The bilateral nature and dorsal displacement of both distal radius and ulna fragments in this case represent an unclassified variation within the Walsh system (Fig. 1). The Walsh classification [7,10] categorizes Galeazzi fractures as follows:
- Type I: Dorsal displacement of the distal radius with volar ulna dislocation
- Type II: Volar displacement of the distal radius with dorsal ulna dislocation.
This fracture pattern did not fit either category, highlighting the importance of meticulous radiographic evaluation for detecting unusual presentations. In pediatric patients, closed reduction and casting are often sufficient for managing Galeazzi fractures, yielding favorable results. However, in adults, surgical intervention is essential due to the strong deforming forces acting on the radius and DRUJ instability [6]. ORIF using a volar (Henry’s) approach remains the standard technique for treating Galeazzi fractures, allowing direct visualization and precise fracture stabilization [9]. In this case, 7-hole LCDCPs provided stable fixation, enabling controlled early mobilization (Fig. 2). DRUJ integrity was confirmed intraoperatively, with fluoroscopic imaging verifying proper realignment [8]. Post-operative care included immobilization in a long-arm cast for 3 weeks to prevent redislocation, followed by progressive range-of-motion exercises to minimize stiffness and optimize function. Potential complications include non-union, malunion, chronic DRUJ instability, and neuropathy. If inadequately treated, DRUJ injuries can lead to chronic pain and functional impairment, sometimes requiring salvage procedures such as the Sauvé-Kapandji or Darrach operations [10]. This patient achieved an excellent functional outcome without complications. Intraoperative assessment, including the piano key test, confirmed DRUJ stability, negating the need for additional fixation. At the 1-year follow-up, the patient exhibited full range of motion and grip strength (Fig. 3-5).


This case describes an extremely rare presentation of bilateral Galeazzi fractures with dorsal displacement of both the distal radius and ulna fragments, a pattern not previously documented. Early surgical intervention, precise anatomical reduction, and intraoperative assessment of DRUJ stability were crucial in achieving successful management. LCDCPs provided rigid fixation, facilitating early mobilization and an excellent recovery outcome. This report highlights the importance of individualized evaluation in complex forearm injuries. Prompt recognition, appropriate surgical intervention, and structured rehabilitation are essential for achieving optimal results. Further documentation of similar cases may contribute to refining classification systems and treatment strategies for atypical Galeazzi fractures.
This case presents a rare, unclassified variant of bilateral Galeazzi fractures with dorsal displacement of both the distal radius and ulna fragments, managed successfully with ORIF using LCDCP. Notably, spontaneous DRUJ realignment occurred without additional fixation, confirmed intraoperatively through the piano key test. Early mobilization following structured immobilization played a crucial role in achieving full functional recovery. This report highlights the need to recognize atypical fracture patterns and refine classification systems for complex forearm injuries.
References
- 1.Rettig ME, Raskin KB. Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-35. [Google Scholar | PubMed]
- 2.Atesok KI, Jupiter JB, Weiss AP. Galeazzi fracture. J Am Acad Orthop Surg 2011;19:623-33. [Google Scholar | PubMed]
- 3.Magill P, Harrington P. Complex volar dislocation of the distal radioulnar joint in a Galleazi variant associated with interposition of the ulnar neurovascular bundle. Eur J Orthop Surg Traumatol 2009;19:265-7. [Google Scholar | PubMed]
- 4.Sebastin SJ, Chung KC. A historical report on Riccardo Galeazzi and the management of Galeazzi fractures. J Hand Surg Am 2010;35:1870-7. [Google Scholar | PubMed]
- 5.Eberl R, Singer G, Schalamon J, Petnehazy T, Hoellwarth ME. Galeazzi lesions in children and adolescents: Treatment and outcome. Clin Orthop Relat Res 2008;466:1705-9. [Google Scholar | PubMed]
- 6.Giannoulis FS, Sotereanos DG. Galeazzi fractures and dislocations. Hand Clin 2007;23:153-63, v. [Google Scholar | PubMed]
- 7.Tsai PC, Paksima N. The distal radioulnar joint. Bull NYU Hosp Jt Dis 2009;67:90-6. [Google Scholar | PubMed]
- 8.Mikić ZD. Galeazzi fracture-dislocations. J Bone Joint Surg Am 1975;57:1071-80. [Google Scholar | PubMed]
- 9.Chu PJ, Lee HM, Hung ST, Shih JT. Stabilization of the proximal ulnar stump after the Darrach or Sauvé-Kapandji procedure by using the extensor carpi ulnaris tendon. Hand (N Y) 2008;3:346-51. [Google Scholar | PubMed]
- 10.Sivakumaran D, Pathinathan K, Madushanger SR, Gunawardena PM, Dimantha WH, Munidasa D. Bilateral symmetrical pronation type of Galeazzi fracture following high-speed motor traffic crash: A case report. Int J Surg Case Rep 2021;85:106284. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Case Report of Simultaneous Galeazzi Fracture Dislocation and Ipsilateral Scaphoid
June 1, 2026 Case Report of Simultaneous Galeazzi Fracture Dislocation and Ipsilateral Scaphoid May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures
May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures April 1, 2026 Modified Posterior Approach for Scapular Body Non-union: A Case Report
April 1, 2026 Modified Posterior Approach for Scapular Body Non-union: A Case Report March 1, 2026 Surgical and Functional outcome of Infective Knee Operated with Arthrotomy
March 1, 2026 Surgical and Functional outcome of Infective Knee Operated with Arthrotomy