
This case report highlights a rare instance of myositis ossificans in the subscapularis muscle with intra-articular extension in a young female, illustrating the importance of accurate diagnosis, imaging, and surgical intervention for effective treatment and recovery.
Dr. Shivam Shah, Department of Arthroscopy and Foot and Ankle, Ganga Medical Center and Hospitals Pvt Ltd, Coimbatore, Tamil Nadu, India. E-mail: shivam.shah92@gmail.com
Abstract
Introduction: Many of the shoulder pathologies present with pain and stiffness; the principal diagnosis of this condition includes calcific tendonitis or rotator cuff tears. Among these, myositis ossificans is very rare.
Case Report: A 22-year-old female presented to us with a complaint of pain in the shoulder for 6 months. On clinical examination, external rotation and internal rotation were restricted. On evaluation, X-ray was normal, while magnetic resonance imaging and computed tomography scan showed 1.5 cm × 1 cm lesion in the subscapularis extending in the shoulder joint. First an ultrasound-guided biopsy was performed, which was followed by open excision biopsy revealing myositis ossificans. Post-operative period was uneventful with the patient achieving full range of motion after 15 days of surgery. Shoulder functional score Constant-Murley score (0–100) increased from 66 to 95, and University of California score (0–35) improved from 17 to 34 from pre-operative to post-operative period, respectively.
Discussion: Myositis is usually a post-traumatic benign heterotopic ossificans that involves large muscles of extremities like the thigh, elbow, etc. So far, only 3 cases have been reported with involvement of rotator cuff tendons, but none with an intra-articular extension. Treatment of this condition is usually conservative; however, surgical treatment is indicated should be considered for those with impaired joint function, continued symptoms, or neurovascular problems. Thus, our case was successfully treated operatively because of impairment in her day-to-day activities.
Conclusion: Myositis ossificans is rare around the shoulder, but when present, it demonstrates differences with respect to appearance and location as compared to other commonly reported heterotopic ossification. Its management should be according to the degree of symptoms and patient-specific complaints.
Keywords: Myositis ossificans, rotator cuff, subscapularis muscle tear, rare case.
Myositis ossificans of rotator cuff tendons is a very rare phenomenon. The pathology of this is not well understood. Although many of the radiological parameters have been discussed in literature but histopathological diagnosis remains the best parameter to confirm its diagnosis. Many of the shoulder pathologies present with pain and stiffness; the principal diagnosis of this condition includes calcific tendinitis or rotator cuff tears. Amongst these, myositis ossificans is very rare. Here, we present a case of a 22-year-old female with myositis ossificans with intra-articular extension. To the best of our knowledge, such a case has not yet been reported.
A 22-year-old female, a computer operator by profession, presented to us with on-and-off pain and stiffness of the left shoulder for 6 months. She complained of increased severity of pain for 1 month and difficulty in working. Patient recalls an episode of mild trauma 1 year back. On clinical examination, there was no swelling, scars, or tenderness. On evaluating a range of motion, it was found that external rotation was restricted and was about 10° and internal rotation was also restricted to L5 (Fig. 1). Forward flexion and abduction were normal, and there was no joint line tenderness. Job’s test, Hawkin’s test, etc., were negative.
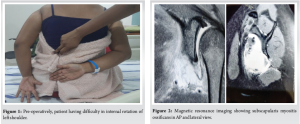
While doing radiological evaluation, X-ray conspicuously was normal, following which a computed tomography (CT) scan and magnetic resonance imaging (MRI) were done, which revealed a lesion sized 1.5 cm × 1 cm in the subscapularis muscle (Fig. 2) with extension into the antero-inferior part of the gleno-humeral joint. The first procedure done was an ultrasound-guided biopsy, which took samples from around and within the lesion. The biopsy report indicated myositis ossificans. Following this planning, open excision and biopsy were undertaken to relieve the patient of all symptoms. A standard Delto-pectoral approach was taken. Skin and soft-tissue were dissected, cephalic vein identified, and it was isolated. The arm put in external rotation to approach the deep aspect of subscapularis and the anterior part of the gleno-humeral joint. Fibrous mass excised from the deep aspect of the subscapularis. Anterior capsulotomy was done, and remaining intra-articular mass was excised and sent for biopsy. Biopsy (Fig. 3) revealed characteristic histology shows zonal pattern with the periphery of the lesion having mature trabeculae of lamellar and woven bone and center of the lesion showing an irregular mass of immature fibroblasts, confirming myositis ossificans.

Postoperatively, active as well as passive shoulder range of motion exercises was started. The patient was started on Indomethacin postoperatively to avoid recurrence.
Post-operative period was uneventful. The patient was started on active assisted as well as active shoulder range of motion exercises. Patient gained full range of motion within 15 (Fig. 4) days of surgery and had significant relief of pain, internal rotation increased from L5 level to T12, and external rotation from 10° to 40°.
Shoulder functional scores such as Constant–Murley score improved from 66 pre-operative to 95 postoperatively whereas University of California score improved from 17 preoperatively to 34 postoperatively.
Myositis ossificans is a benign heterotopic ossification that involves muscle or any other soft tissue [1,2]. 60–75% of myositis cases are found to be occurring post-trauma [3]. It occurs predominantly at sites like the large muscles of the extremities (i.e., the thigh, buttocks, and elbow), but it may occur anywhere in the body [4,5]. However, myositis ossificans in the rotator cuff muscle is extremely rare. So far, only three such cases have been reported; the other cases involved the supraspinatus tendon; one was associated with a significant cuff tear [6]; the other arose from a calcified portion of the rotator cuff tendon that expanded to the subacromial bursa [7]. In the last case, histological observation revealed that the ossified mass was embedded only in the tendinous region. With regard to the pathogenesis of myositis ossificans being associated with trauma, several theories had been proposed in the literature [8,9]: like – an ossifying process associated with hematoma or an osteoblastic formation caused by osteoblasts migrating into soft tissue from the periosteum; and ossification caused by the periosteum pushed into the muscle by mechanical injury. However, none of these studies have exactly explained the biological basis of myositis. Recently, advances in molecular biology have revealed that the hematoma caused by trauma or autolysis of scattered bone fragments present in muscle is a precursor to the release of bone morphogenetic proteins (BMPs), which induce de-differentiation of pluripotent mesenchymal stem cells into osteogenic cells [10]. On the basis of these facts, we assume that minor trauma might have led to the development of the heterotopic ossification in our case. However, its exact pathogenesis was still uncertain. Plain radiographs are conspicuously normal in the early stages. The appearance of mineralization is characterized by an increased density in the peripheral legion in the later stages. CT scan is a good imaging modality that shows zoning mineralized pattern with extensive perilesional edema in muscular tissue [11]. MRI is also a useful tool for identifying early lesions. However, most MRI features in myositis ossificans are non-specific, and may vary with the stage of its maturation [11]. Extensive muscle and perilesional edema are a typical features of myositis ossificans that may be depicted clearly on MR images [11]. Differential diagnoses of myositis include conditions such as – extra-skeletal osteosarcoma [12] and synovial sarcoma [13] as well as periosteal or extra-skeletal osteosarcoma, chondrosarcoma, and metastatic carcinoma. A biopsy examination should be considered to confirm the diagnosis. Treatment of myositis ossificans is usually conservative management because of its self-limiting character and spontaneous regression. Surgical treatment including resection of the lesion should be considered for those with impaired joint function, continued symptoms, or neurovascular problems. However, our case was successfully treated operatively because of impairment in her day-to-day activities. For post-operative prophylaxis, radiation therapy and nonsteroidal anti-inflammatory drugs (NSAIDs) remain the most widely used therapeutic modalities. But with the use of COX-2 selective NSAIDs like indomethacin most of these problems have been sought. Noggin (a BMPs inhibitor), pulsed electromagnetic fields, and free radical scavengers in the form of allopurinol and N-Acetylcysteine are considered new methods. They are in evaluated to take the place of radiation and NSAID therapy as the method of prophylaxis, with research being in early stages [14]. Considering these factors, our patient was started on oral indomethacin to prevent recurrence.
Myositis ossificans is rare around the shoulder, but when present, it demonstrates differences with respect to appearance and location as compared other commonly reported heterotopic ossification. Its management should be according to the degree of symptoms and patient-specific complaints.
Subscapularis myositis ossificans, while rare in the shoulder region, should be considered in young patients presenting with shoulder pain and restricted motion, especially after trauma; therefore an accurate imaging and histopathological confirmation are essential for diagnosis, and surgical intervention may be necessary to restore function and relieve symptoms when conservative treatment fails.
References
- 1.McCarthy EF, Sundaram M. Heterotopic ossification: A review. Skeletal Radiol 2005;34:609-19. [Google Scholar | PubMed]
- 2.Norman A, Dorfman HD. Juxtacortical circumscribed myositis ossificans: Evolution and radiographic features. Radiology 1970;96:301-6. [Google Scholar | PubMed]
- 3.Rosenberg AE. Myositis ossificans and fibro osseous pseudotumor of digits. In: Fletcher CDM, Unni KK, Mertens F, editors. World Health Organization Classification of Tumours. Pathology and genetics of tumours of soft tissue and bone. 1st ed. Lyon: IARC Press; 2002. p. 52-4. [Google Scholar | PubMed]
- 4.Johnson MK, Lawrence JF. Metaplastic bone formation (myositis ossificans) in the soft tissues of the hand. Case report. J Bone Joint Surg Am 1975;57:999-1000. [Google Scholar | PubMed]
- 5.Goto H, Hatori M, Kokubun S, Makino M. Myositis ossificans in the tip of the thumb: A case report. Tohoku J Exp Med 1998;184:67-72. [Google Scholar | PubMed]
- 6.Martin DK, Zadow SP, Pandit S, Falworth MS. Myositis ossificans of the subscapularis: An unusual case of restricted internal rotation. J Shoulder Elbow Surg 2008;17:e21-4. [Google Scholar | PubMed]
- 7.Hatta T, Hatori M, Sano H, Watanuki M, Kishimoto KN, Hosaka M, et al. Myositis ossificans of the rotator cuff muscles. J Orthop Sci 2013;18:675-8. [Google Scholar | PubMed]
- 8.Booth DW, Westers BM. The management of athletes with myositis ossificans traumatica. Can J Sport Sci 1989;14:10-6. [Google Scholar | PubMed]
- 9.Cushner FD, Morwessel RM. Myositis ossificans traumatica. Orthop Rev 1992;21:1319-26. [Google Scholar | PubMed]
- 10.Ramieri V, Bianca C, Arangio P, Cascone P. Myositis ossificans of the medial pterygoid muscle. J Craniofac Surg 2010;21:1202-4. [Google Scholar | PubMed]
- 11.Parikh J, Hyare H, Saifuddin A. The imaging features of post-traumatic myositis ossificans, with emphasis on MRI. Clin Radiol 2002;57:1058-66. [Google Scholar | PubMed]
- 12.Oonuma M, Hatori M, Hosaka M, Kokubun S. Extraskeletal osteosarcoma arising in the buttock. Ups J Med Sci 2001;106:211-5. [Google Scholar | PubMed]
- 13.Hara S, Hatori M, Hosaka M, Komatsu T, Tsuchiya T, Kimura N. Synovial sarcoma with massive ossification--a case report. Ups J Med Sci 2003;108:151-8. [Google Scholar | PubMed]
- 14.Bierd EO, Kang QK. Prophylaxis of heterotopic ossification - an updated review. J Orthop Surg Res 2009;4:12. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Chondromyxoid Fibroma of the Right Thumb: Successful Management with Wide Local Excision, Iliac Crest Bone Grafting and K-Wiring – A Rare Case Report
April 1, 2026 Chondromyxoid Fibroma of the Right Thumb: Successful Management with Wide Local Excision, Iliac Crest Bone Grafting and K-Wiring – A Rare Case Report January 1, 2026 Arthroscopic Anchorless Rotator Cuff Repair with Anterior Cruciate Ligament Jig using the “J Technique:” A Cost-Effective Alternative
January 1, 2026 Arthroscopic Anchorless Rotator Cuff Repair with Anterior Cruciate Ligament Jig using the “J Technique:” A Cost-Effective Alternative November 1, 2025 Superior Capsular Reconstruction Using Biceps Tendon Autograft with Novel Biceps Tenodesis Arthroscopic Fixation: A Case Report
November 1, 2025 Superior Capsular Reconstruction Using Biceps Tendon Autograft with Novel Biceps Tenodesis Arthroscopic Fixation: A Case Report September 1, 2025 A Silent Shoulder of Plentiful Pathology: An Uncommon Presentation of Acromioclavicular Ganglion Cyst
September 1, 2025 A Silent Shoulder of Plentiful Pathology: An Uncommon Presentation of Acromioclavicular Ganglion Cyst