
Osteotomy and realignment relieve knee symptoms and preserve function in malunited femur with arthritis.
Dr Parvir Kuru, Department of Orthopaedics, FMHS SGT University, Gurugram, Haryana, India. E-mail: drkurupsingla@icloud.com
Abstract
Introduction: Malunited femur shaft fractures with associated deformities can lead to secondary knee osteoarthritis, often necessitating total knee replacement. Correcting these deformities can offload the knee joint and preserve function.
Case Report: A 53-year-old male presented with a 14-year history of malunited right femur shaft fracture, complicated by a broken K-nail and a 23° varus deformity. He complained of medial knee pain for the past 6 months, with a VAS score of 7. Radiographs revealed Grade 3 medial compartment osteoarthritis. Initially advised total knee replacement, the patient opted for deformity correction with realignment. Surgical management involved two-level femoral osteotomy, implant removal, and fixation with interlocking intramedullary nailing. Post-operative imaging showed normal alignment and significant opening of the medial joint space. The patient’s pain decreased to a VAS score of 3, and he began partial weight-bearing on the second post-operative day.
Conclusion: Deformity correction through osteotomy and realignment can alleviate knee symptoms and prevent further degenerative changes, thereby preserving the knee joint and avoiding total knee replacement. This approach offers a functional solution for patients with malunited femur fractures and knee arthritis, improving clinical outcomes and quality of life.
Keywords: Malunited femur, K-nail, knee arthritis, deformity correction, osteotomy, knee preservation.
Deformities of the femoral and tibial shaft and metaphysis outside the capsulo-ligamentous complex, not involving the articular surface, are known as extra-articular deformities. There are three axes, namely vertical, mechanical, and anatomical. Restoration of these ensures normal alignment and loading through the knee joint [1]. These deformities lead to secondary osteoarthritis of the knee [2]. Malunited fractures are the most common cause of extra-articular deformities. Other factors could be congenital, metabolic, and post-infective [2,3].
A 53-year-old male came to SGT hospital with gross deformity of the right thigh of 14 years duration and pain over the medial side of the knee for 6 months with a VAS score of 7. The patient gives a history of a road traffic accident in December 1991, in which he sustained a right femur shaft fracture, for which he was operated on with a K-nail. He gives a history of re-trauma after 2 months of surgery in which he sustained an injury on the operated side. He did not undergo any surgery 2nd time. The patient gives a history of gradual increase in deformity of the right thigh for a few years following re-trauma. Now, the patient came with a complaint of pain over the medial side of the knee joint for the last 6 months and deformity for 14 years. No other significant history or any comorbidities. Clinical assessment reveals a short limb gait and limb length discrepancy of 3 cm. He had gross varus deformity of the right thigh with right knee medial joint line tenderness. There was no significant muscle atrophy. He had a full knee range of motion and was able to squat and sit on a crossed leg. Spine, bilateral hip, and ipsilateral ankle examination findings were normal. Plain radiograph in two views demonstrated gross varus deformity of 23⁰ of the right middle third femur following malunion with broken K-nail at two places in situ (Fig. 1) with Kellgren–Lawrence Grade 3 knee osteoarthritis (Fig. 2). The deformity angle was 23°.
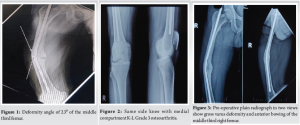
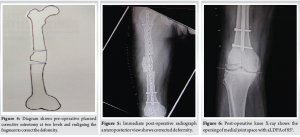
The apex of the deformity was at the middle third of the right femur. The lateral view of the femur revealed anterior bowing of the femur in the sagittal plane (Fig. 3). Malunited right femur shaft fracture with broken K-nail in situ with 3 cm shortening with secondary degenerative arthritis medial compartment right knee. Osteotomy at two levels (Fig. 4), realigning implant removal and internal fixation with interlocking nailing.
Surgical procedure
The patient was positioned supine over the fracture table. Through the vastus lateralis splitting lateral approach, the deformed site of the femur bone is exposed. Under image guidance, upper and lower levels of deformity were identified, and then osteotomy was done at two levels 7 cm apart. The broken nail was removed from the osteotomy site, and the fragment was rotated by 180° to correct the deformity. Fixation was done with interlocking intramedullary nailing. Clinically and radiologically confirmed, deformity correction, normal anatomical axis, and opening of medial joint space right .
Outcome and follow-up
Post-operative radiograph demonstrates normal anatomical axis (Fig. 5), deformity corrected, and significant opening of medial joint space of right knee (Fig. 6).
The aLDFA measured was 85° (Fig. 6). In the lateral view, there was no deformity, and clinically assessed, there was no rotational component.
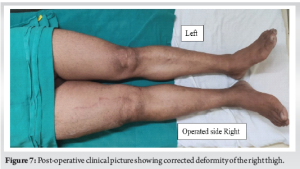
Clinically, the deformity was corrected and the patient was started on partial weight bearing on Post-operative day 2 and his main symptoms of medial side knee pain were significantly improved with a VAS score of 3 (Fig.7).
At the 6-month follow-up, the patient was walking full weight bearing with a mild limp, and there were no complaints of medial side knee pain, which was his main complaint preoperatively (Fig. 8).

The radiologically distal level osteotomy site was united, but the proximal level was not united, which might be the reason for his limp. The implant was in position without failure (Fig. 9).
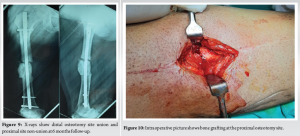
At 6 months follow-up, he underwent bone grafting at the proximal site of osteotomy (Fig. 10).
In post-traumatic deformity of the lower limb, an angulation of more than 12° in valgus deformity, 6° in varus deformity, 15° in external rotation, and 10° in internal rotation should be corrected [4]. If it is not corrected, degenerative changes will progress over time in the knee joint. In such cases, options are extra-articular corrective osteotomy only, extra-articular corrective osteotomy with total knee replacement in one or two stages [5], and intra-articular corrective osteotomy with total knee replacement [5]. In the present case, the patient was advised total knee replacement with corrective osteotomy at another center. After discussing with the patient, it was planned that the only corrective osteotomy with the aim of regaining normal alignment and length. It will help to preserve the knee by off-loading the medial compartment. After deformity correction and fixation with interlocking nailing, it was observed intra-operatively that there was an opening of the medial joint space of the knee. Preoperatively, radiological arthritis was of Grade 3, and immediately after correction, radiological arthritis was labeled as Grade 1. Symptomatically also, on weight-bearing, there was a significant improvement in medial side knee pain. Correcting the deformity on time and regaining the alignment can preserve the knee and prevent further progress in arthritis, which alleviates the need for total knee replacement. The limitation of our case report are we are yet to see long-term follow-up and outcome assessment [6]. In addition, studies indicate that the impact of mechanical axis alignment plays a crucial role in post-operative outcomes in knee surgeries [8], and understanding the biomechanical implications of post-traumatic loading on the knee can provide further insights into joint preservation strategies [9,10].
With only deformity correction and realigning the anatomical axis, the knee joint can be preserved. Correcting the deformity on time and regaining alignment helps prevent the progression of arthritis, thereby alleviating the need for total knee replacement.
This Article emphasizes that timely correction of deformities and proper alignment of the anatomical axis can effectively preserve the knee joint. This approach not only alleviates the symptoms associated with various deformities and degenerative arthritis but also can prevent the need for more invasive procedures, such as total knee replacement.
References
- 1.Paley D, Tetsworth K. Mechanical axis deviation of the lower limbs. Preoperative planning of uniapical angular deformities of the tibia or femur. Clin Orthop Relat Res 1992;280:48-64. [Google Scholar | PubMed]
- 2.Khanna V, Sambandam SN, Ashraf M, Mounasamy V. Extra-articular deformities in arthritic knees-a grueling challenge for arthroplasty surgeons: An evidence-based update. Orthop Rev (Pavia) 2017;9:7374. [Google Scholar | PubMed]
- 3.Catonné Y, Khiami F, Sariali E, Ettori MA, Delattre O, Tillie B. Same-stage total knee arthroplasty and osteotomy for osteoarthritis with extra-articular deformity. Part II: Femoral osteotomy, prospective study of 6 cases. Orthop Traumatol Surg Res 2019;105:1055-60. [Google Scholar | PubMed]
- 4.Rosemeyer B, Pförringer W. Basic principles of treatment in pseudarthroses and malunion of fractures of the leg. Arch Orthop Trauma Surg (1978) 1979;95:57-64. [Google Scholar | PubMed]
- 5.Koenig JH, Maheshwari AV, Ranawat AS, Ranawat CS. Extra-articular deformity is always correctable intra-articularly: In the affirmative. Orthopedics 2009;32:((9):10.3928/01477447-20090728-22. [Google Scholar | PubMed | CrossRef]
- 6.Bhandari M, Swiontkowski MF. Management of acute fractures of the femur: An overview. J Bone Joint Surg Am 2017;99:2097-106. [Google Scholar | PubMed]
- 7.Paley D. Principles of deformity correction. In: Paley D, editor. Principles of Deformity Correction. Berlin: Springer-Verlag; 2002. p. 1-64. [Google Scholar | PubMed]
- 8.Lange J, Gamblin J, Eidelman M. The impact of mechanical axis alignment on the outcomes of total knee arthroplasty: A systematic review. J Arthroplasty 2018;33:2453-60. [Google Scholar | PubMed]
- 9.Kettunen J, Rusanen T, Laine S. The effect of post-traumatic knee joint loading on degenerative changes: A biomechanical approach. Knee 2017;24:1037-45. [Google Scholar | PubMed]
- 10.Patel VR, Nair AG, Harsulkar A. Orthoplastic management of complex lower limb injuries: A comprehensive review. Injury 2020;51:2145-57. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series
May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series April 1, 2026 Late-onset Legg-Calvé-Perthes Disease Treated with Varus Derotation Femoral Osteotomy: A Case Report
April 1, 2026 Late-onset Legg-Calvé-Perthes Disease Treated with Varus Derotation Femoral Osteotomy: A Case Report December 1, 2025 Double Angle Varus Corrective Osteotomy in a Case of Severe Coxa Vara – A Case Report
December 1, 2025 Double Angle Varus Corrective Osteotomy in a Case of Severe Coxa Vara – A Case Report December 1, 2025 “Less is More”- A Minimalistic Surgical Intervention to Correct the Right Upper Limb Deformity in an Isolated Right Radial Club Hand: A Case Report
December 1, 2025 “Less is More”- A Minimalistic Surgical Intervention to Correct the Right Upper Limb Deformity in an Isolated Right Radial Club Hand: A Case Report