
Neglected central hip fracture dislocations with incarcerated head are often irreducible by ORIF, making THA a reliable salvage option. Successful outcomes require proper medial wall reconstruction with bone graft ± titanium mesh and restoration of hip center of rotation.
Dr. Somok Banerjee, Department of Orthopaedics, AIIMS Raipur, Chhattisgarh, India. E-mail: somokbanerjee964@gmail.com
Abstract
Introduction: Isolated quadrilateral plate fracture with central hip dislocation is a rare occurrence. Such difficult-to-treat fractures can be managed with both open reduction and internal fixation (ORIF) and total hip arthroplasty (THA). We hereby describe the management of such a case of neglected irreducible central hip dislocation with quadrilateral plate fracture with THA in this case report.
Case Report: A 55-year-old male patient presented to our outpatient department with 5 month old neglected post-traumatic central dislocation of the hip with a quadrilateral plate fracture. Initially, ORIF with infrapectineal plating was planned by anterior intra-pelvic approach. But despite best efforts (lateral and longitudinal traction along with reduction tools and maneuvers) it was not possible to reduce the head femur back into the native acetabular floor due to the long-standing napkin ring constriction. It was decided intra-operatively to proceed with THA. The patient was subsequently repositioned for THA using a standard posterior approach. The head femur was removed piecemeal and the medial wall defect was reconstructed using contoured titanium mesh with impaction bone grafting and rest THA was done in the usual manner. The patient was mobilized from 2nd post-operative day and allowed partial weight bearing with gradual progression to full weight bearing by 3rd week. He could return to his daily activities by 6 months and had a Modified Harris Hip Score of 91 in 1 year follow-up. Radiographs revealed well incorporation of the bone graft with no evidence of loosening. The patient didn’t have any complications such as infection. Heterotopic ossification or dislocation.
Conclusion: THA in neglected irreducible central hip dislocation with quadrilateral plate fracture has good functional and radiological outcome.
Key words: Central hip dislocation, quadilateral plate fracture, total hip arthroplasty, impaction bone grafting.
Hip dislocation has been traditionally classified as anterior and posterior based on the location of the head femur with respect to the acetabular plane. Central dislocation though considered a misnomer by some authors is an established clinical entity with much ambiguity in classification, approach, and treatment options [1]. It has been described by Chung et al. as an intrapelvic migration of the head femur due to medial disruption of the hip capsule with subsequent quadrilateral plate fracture [2]. We report a case of a neglected 5-month-old quadrilateral plate fracture with irreducible central dislocation of the head femur in an active patient treated with total hip arthroplasty (THA).
History
A 55-year-old male patient, a farmer by occupation sustained an injury to his right hip 5 months back due to a road traffic accident for which he resorted to analgesics and bed rest as suggested by a local bone setter in his village. He started mobilizing 2 months later using a stick. After 3 months, he presented with a painful shortened right hip with the inability to bear weight in his right hip.
Examination
On examination, both his anterior superior iliac spines (ASIS) were at the same level. He had a 20° fixed external rotation deformity of his right hip with 2 cm shortening of his right lower limb. Movements in the right hip were restricted and painful. He had a modified Harris hip score (mHHS) of 20.
Investigations
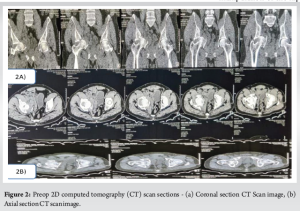
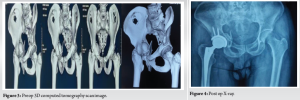
Xray (Fig. 1) and computed tomography (CT) scan (Figs. 2 and 3) were done to find out that he had an isolated Quadrilateral plate fracture with intrapelvic dislocation of the head femur with a napkin ring constriction around the dislocated head femur. However, both the anterior and posterior acetabulum columns were intact.

 “““““““““““““““““`
“““““““““““““““““`
Treatment
Owing to the neglected and complex nature of the fracture along with incarcerated head femur we counseled the patient about the prognosis associated with the possible treatment options – Open reduction and internal fixation (ORIF) of the quadrilateral plate and THA with medial wall reconstruction. Initially, we planned for ORIF with Quadilateral plate fixation for which we had positioned him supine. Closed reduction was first attempted using lateral traction by a Schanz pin inserted in Greater trochanter along with longitudinal traction and closed manipulation of the hip. As anticipated, the closed reduction maneuvers were unsuccessful, following which we used the anterior intrapelvic approach to reduce the quadrilateral plate. Hereby the acetabular columns were found to be intact with a comminuted quadrilateral plate fracture. Furthermore, the fractured quadrilateral plate was osteopenic and friable owing to the delayed presentation. There was a napkin ring constriction and dense fibrosis around the head femur. The fibrosis was cleared and using ball spike it was tried to reduce the head femur back into the acetabular cavity, but due to the napkin ring constriction, it wasn’t possible to reduce the head femur despite the best reduction maneuvers and traction. Furthermore, the fractured quadrilateral plate was too osteopenic for a robust buttress fixation. The only option left for reduction was to do a double anterior column osteotomy or proceed for primary THA. Keeping in mind, the age of the patient, long-standing nature of the dislocated head femur, necrotic patch in the superomedial aspect of the head femur along with the incarcerated head, osteopenic quadrilateral plate it was decided to proceed with THA. Subsequently the patient was positioned in lateral decubitus position for THA. The hip joint was exposed using standard posterior approach. In situ napkin osteotomy of the neck femur done and the head femur was taken out piecemeal using a corkscrew, blunt hohmann retractors and bone nibbler with utmost care of not causing any inadvertent injury to the acetabular fossa. Once the entire head was taken out as further confirmed by C-arm, acetabular reaming was done in the peripheral rim to obtain a good viable host bone interface for using an uncemented cup. Now we had a Paprosky type 2C defect (medial defect to deal with for which we used a titanium mesh secured to the medial defect after appropriate contouring over which morselized autograft (obtained from extracted head femur) was placed. Reverse reaming of the acetabular floor was done to get an evenly distributed graft over the cavity and uncemented acetabular cup size 52 was used to obtain a line-to-line fit which was further augmented with 3 acetabular screws in the iliac buttress. A stable acetabular component insertion was thus obtained with the quadrilateral plate left untouched. The Highly crosslinked Polyethylene liner was next inserted into the acetabular cup and thereafter femoral preparation was done using the standard technique – uncemented Hydroxyapatite-coated Femur stem size 4 was thereby used for femoral component with head size 32. The prosthetic hip was reduced and adequate stability with a good range of motion without impingement was confirmed. The patient was mobilized from postoperative day 2 and allowed toe touch weight bearing gradually progressing to partial weight bearing and then to full weight bearing by 3 weeks. There was no limb length discrepancy and the patient was able to do straight leg raise and abduction against gravity by 6 weeks. Radiographs revealed well incorporation of the bone graft with no evidence of loosening (Fig. 4). He could return to his daily activities at 6-month follow-up with mHHS of 91 after year (Fig. 5). The patient did not have any complications such as infection. Heterotopic ossification or dislocation.
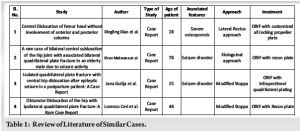
Isolated quadrilateral plate fractures with central dislocation of the head femur is an extremely rare occurrence. Till date only 5 such cases have been reported including the present one (Table 1) [1,3-5]. Quadilateral plate fractures are classified by many authors like ElNahal et al., Yang et al., and Chen et al. but there is wide disparity in the existing treatment options for this fracture especially if there is a napkin ring constriction around the dislocated head femur as seen in neglected cases [6,7]. Its extremely difficult to reduce the incarcerated head femur back into the native acetabulum in chronic cases. The feasibility of the Double osteotomy of the Anterior column for irreducible central fracture dislocation of head femur also is doubtful in such cases due to the risk of- osteonecrosis of the head femur, osteopenic fractured quadrilateral plate, and non viability of fracture fragments [8]. The existing treatment options for these fracture dislocations include ORIF with recon plate, infrapectineal plate, propeller plates, etc, and THA in irreducible cases [9]. In our case, we had a 55-year-old patient with 5-month-old irreducible central dislocation of the head femur with quadilateral plate fracture for which we decided to proceed with THA after failed attempts of open reduction. The head femur was taken out piecemeal and was used as autograft over a titanium mesh contoured overlying the medial wall defect. The management options for medial wall defects include- impaction bone grafting ± mesh with large uncemented porous-coated hemispherical cups, cemented cups, jumbo cups, antiprotrusio cages and cup-cage construct [10,11].
 Impaction bone grafting with hemispherical cup alone has been successfully used for the management of medial wall defects in THA, but there has been concerns about resorption of bone graft with time leading to migration and failure of cups [12,13]. To prevent this, the use of titanium mesh has been long advocated along with impaction bone grafting. It has been postulated that titanium mesh when used to cover the defect along with impaction bone grafting helps in the even distribution of stress in the impact-graft interface and also promotes better osseointegration along with less peri-implant osteolysis in the long run [14]. We thereby successfully reconstructed the medial wall and did THA with restoration of the center of rotation, sufficient stability, and a good range of motion without impingement in the hip joint.
Impaction bone grafting with hemispherical cup alone has been successfully used for the management of medial wall defects in THA, but there has been concerns about resorption of bone graft with time leading to migration and failure of cups [12,13]. To prevent this, the use of titanium mesh has been long advocated along with impaction bone grafting. It has been postulated that titanium mesh when used to cover the defect along with impaction bone grafting helps in the even distribution of stress in the impact-graft interface and also promotes better osseointegration along with less peri-implant osteolysis in the long run [14]. We thereby successfully reconstructed the medial wall and did THA with restoration of the center of rotation, sufficient stability, and a good range of motion without impingement in the hip joint.
Our Case report highlights the management of a neglected quadrilateral plate fracture with central hip dislocation in an elderly patient with THA. Although ORIF of such fracture dislocation should be attempted in viable cases, the option of THA should always be kept for neglected cases. The results of THA is equivalent to that of ORIF for such complex fracture-dislocation cases.
THA is a good option for chronic irreducible central dislocation of femur head with isolated quadrilateral plate fractures with good functional outcomes. Restoration of the center of rotation of the hip should be given importance along with adequate reconstruction of the medial defect in such cases.
References
- 1.Xiao X, Chen J, Wang C, Liu H, Li T, Wang H, et al. Central dislocation of femoral head without involvement of acetabular anterior and posterior columns. J Int Med Res 2018;46:3388-93. [Google Scholar | PubMed]
- 2.Chung H, Sohn HS, Oh JK, Lee S, Kim D. Biomechanical comparison of fixation methods for posterior wall fractures of the acetabulum: Conventional reconstruction plate vs. Spring plate vs. Variable angle locking compression plate. Medicina (Kaunas) 2024;60:882. [Google Scholar | PubMed]
- 3.Makwana K, Vijayvargiya M, Agarwal N, Desai K, Shetty V. A rare case of bilateral central subluxation of the hip joint with associated bilateral quadrilateral plate fracture in an elderly male due to seizure activity. Rev Bras Ortop 2017;53:489-92. [Google Scholar | PubMed]
- 4.Gulija J, Žigman T, Dobrić I, Bobovec D, Gusić N. Isolated quadrilateral plate fracture with central hip dislocation after epileptic seizure in a postpartum patient: A case report. Chin J Traumatol 2024;27:410-3. [Google Scholar | PubMed]
- 5.Ceri L, Zanna L, Buzzi R, De Biase P. Obturator dislocation of the hip associated with ipsilateral quadrilateral plate fracture: A rare case report. Trauma Case Rep 2021;32:100451. [Google Scholar | PubMed]
- 6.Chen CM, Chiu FY, Lo WH, Chung TY. Cerclage wiring in displaced both-column fractures of the acetabulum. Injury 2001;32:391-4. [Google Scholar | PubMed]
- 7.Chen K, Yao S, Yin Y, Wan Y, Ahn J, Zhu S, et al. A new classification for quadrilateral plate fracture of acetabulum. Injury 2023;54:110762. [Google Scholar | PubMed]
- 8.Kumar A, Clayson AD. Irreducible central fracture-dislocation of the hip: Using an anterior column osteotomy for operative reduction. Injury Extra 2005;36:199-202. [Google Scholar | PubMed]
- 9.Freude T, Gänsslen A, Krappinger D, Lindahl J. Quadrilateral plate fractures. Arch Orthop Trauma Surg 2024;145:51. [Google Scholar | PubMed]
- 10.Ansari S, Gupta K, Gupta T, Raja BS, Pranav J, Kalia RB. Total hip arthroplasty in protrusio acetabuli: A systematic review. Hip Pelvis 2024;36:12-25. [Google Scholar | PubMed]
- 11.Berry DJ. Acetabular component revision with jumbo uncemented hemispherical cups. Curr Opin Orthop 2002;13:38-42. [Google Scholar | PubMed]
- 12.Ibrahim MS, Raja S, Haddad FS. Acetabular impaction bone grafting in total hip replacement. Bone Joint J 2013;95-B:98-102. [Google Scholar | PubMed]
- 13.Abu-Zeid MY, Habib ME, Marei SM, Elbarbary AN, Ebied AA, Mesregah MK. Impaction bone grafting for contained acetabular defects in total hip arthroplasty. J Orthop Surg 2023;18:671. [Google Scholar | PubMed]
- 14.García-Rey E, Madero R, García-Cimbrelo E. THA revisions using impaction allografting with mesh is durable for medial but not lateral acetabular defects. Clin Orthop Relat Res 2015;473:3882-91. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study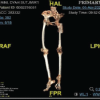 June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review
June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review June 1, 2026 A Case of Bilateral Steroid Arthropathy of the Hip Following Repeated Intra-articular Steroid Injections
June 1, 2026 A Case of Bilateral Steroid Arthropathy of the Hip Following Repeated Intra-articular Steroid Injections June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report
June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report