
Use of metal mesh in low-resource settings can save the joint.
Dr. Ashwani Mudgil, Department of Orthopaedics, Civil Hospital, Ambala Cantt, Haryana. India. E-mail: docashwanimudgil@gmail.com
Abstract
Introduction: Joint replacement surgeries have gained momentum in the recent years. Chronic negligence by the patients is very commonly seen in developing countries leading to gross deformity of the joints.
Case Report: We report a case of 59-year-old female who had avascular necrosis of the right hip with complete erosion of medial wall of acetabulum. A metal mesh, customized to this patient, was used along with the primary total hip arthroplasty to reconstruct and stabilize the acetabulum.
Conclusion: The mesh provided stability to the hip joint, and currently, the patient is under follow-up with promising results.
Keywords: Acetabulum, arthroplasty, femur head necrosis, total hip replacement.
Joint replacement surgeries have gained momentum in the recent years and proved to be a boon to patients with joint pain [1]. These surgeries directly affect their lives by leading to an improvement in their daily activities [2]. Sometimes, due to financial burden especially in middle- low-income countries like India, the patients often delay to seek proper consultation, which eventually complicate their clinical condition. We report a case of 59-year-old female who had neglected her hip pain for more than 35 years and eventually landed up with avascular necrosis of hip with complete erosion of the medial wall of acetabulum.
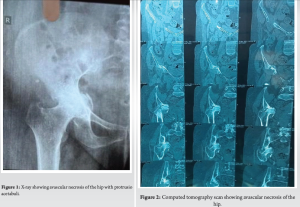
A 59 year old female presented to our outdoor clinic with complaints of pain in the hip and inability to ambulate for 3 months. She had long-standing history of steroid use due to her history of rheumatoid arthritis. She was diagnosed as a case of avascular necrosis of the right hip. She was advised by our surgical team to undergo total hip replacement. On clinical examination, the patient had restricted and painful range of motion during the abduction, adduction, flexion, and extension with fixed flexion deformity. The neurovascular examination was normal. Routine pre-operative laboratory investigations were done to rule out infection (a differential white blood cells count, erythrocyte sedimentation rate [ESR], and C-reactive protein) and were within normal ranges except ESR which was raised 32 mm/h. Plain anteroposterior radiographic imaging of the patient showed avascular necrosis of the hip with protrusio acetabuli (Fig. 1). The findings were confirmed by computed tomography which showed a lack of medial wall of acetabulum (Fig. 2). According to Rubin classification, this defect was classified as class III as femoral head has protruded medial to the iliopectineal line [3].
Surgical procedure
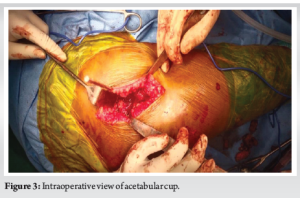
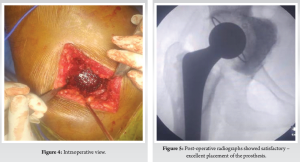
After obtaining verbal and written consent from the patient, surgery was performed under combined spinal epidural anesthesia; whereas the patient was in a lateral decubitus position, a modified direct lateral approach was utilized, after defining the proximal femur and acetabulum. The gross appearance of the tissues was normal. The surgery proceeded as per the institutional protocol. Preparation of the acetabulum was started by reaming the peripheral rim sequentially till a bleeding cancellous bony surface was obtained. An acetabular trial cup less than the last reamer by about 6–8 mm was used to determine the depth of the needed mesh and graft to restore the hip center of rotation, relying on the transverse acetabular ligament as a reference. A morselized cotical bone graft from the native femoral head was prepared as per the guidelines [3]. The mesh was customized to the patient as per the measurement after the trial acetabular cup (Fig. 3 and 4). The femoral head monobloc shell was impacted into the metal mesh as one unit. The reamed femoral part was impacted against the metal mesh and impacted inside the acetabulum with the help of an impactor and mallet. Afterward cemented acetabular cup which was 3 mm smaller than the last reamer was inserted along with antibiotic-laden cement. Cemented femoral component was inserted in the femur. Postoperative period: Post-operative radiographs showed satisfactory – excellent placement of the prosthesis (Fig. 5). The patient was allowed to toe touch weight-bearing on the second postoperative day till 1 month postoperatively using walker, then she started full weight-bearing after 1 month. Deep vein thrombosis prophylaxis as per the institutional protocol was started. The patient is currently under follow-up at regular intervals in our outpatient clinic. The patient is showing excellent outcome with a Harris Hip Score of 95.6 at 1-month postoperatively. She was walking without the help of any assistance.
Total hip arthroplasty is a common orthopedic surgery being done in various centers across the world. It leads to alleviation of pain and disability, hence leading to a normalcy in the patient’s life. Certain patients, especially in countries where the healthcare systems are overburdened or due to financial constraints, often delay to seek appropriate consultation at proper time. This leads to various complications which pose various challenges to the surgeon. Any bone defect can complicate a straightforward surgery. Mostly such bony defects are iatrogenic and seen during revision surgeries. Various studies have documented such cases and give appropriate treatment by using mesh either titanium, propylene [4-6]. Acetabulum is a richly supplied bone which derives its blood supply form iliolumbar artery, obturator artery, internal pudendal artery, superior and inferior gluteal arteries, and the external iliac artery. Erosion or avascular necrosis of this bone is rare but still documented [7]. Acetabular reconstruction has been attempted through various techniques, in which bone grafting is also combined with titanium alloy mesh. Impaction bone grafting along with the mesh can fill the bone defect and restore the anatomy of the acetabulum by dispersing the load on the bone. Mostly such measures are used during revision surgeries where iatrogenic injuries can lead to bone loss, but patients can present with bone deficit during the primary surgery too. It may be due to long standing duration of the illness, neglect by the patient, or complicated by other conditions. Primary and revision arthroplasty of the hip aims to stabilize the hip by using apt implant positioning, reduced soft tissue tension, and a good capsular repair. Additional use of a variety of liners (polyethylene, constrained) or use for large femoral heads, etc., are used to mitigate the problem of hip instability. Such patients develop chronic conditions which are often difficult to treat and predisposes the patient to revision surgeries [5]. Using a mesh to reconstruct the acetabular bony deficit may be a good solution to such patients. Bone impaction with bone grafts can restore the bone stock and provide support to the hip prosthesis. It also prevents the thermal damage of the graft and provides a good bed for the cemented cup [8]. Wire mesh or cages are also an option to be explored. Polypropylene mesh has been used in oncologic cases which require wide resection and replacements. There is a lack in literature where mesh is used for chronic hip disability. The decision to use metal or polypropylene is patient specific and at the discretion of the surgeon. Mostly, this is used on the revision stage of the surgery but if noticed prior to the primary arthroplasty, it can avoid any future revision surgery which in itself poses various issues to the patient, both physically and financially.
Limitations
The case report is limited to a single patient. To evaluate the effectiveness of metal mesh in primary arthroplasty, it needs to be researched in a larger population with longer post-operative follow up to see long term sequelae, if any. Further studies are required to explore this area and its comparison with the conventional methods.
Metal mesh can provide the stability and may be incorporated in such cases. It can also prevent major migration of cement across the medial wall of the acetabulum.
This case demonstrates the successful use of customized metal mesh in primary total hip arthroplasty for severe acetabular deficiency. The innovative surgical approach involved impaction bone grafting using morselized autograft from the native femoral head, combined with a patient specific metal mesh to reconstruct the acetabular defect. The mesh provided structural support for cement containment and prosthetic stability. In resource- constrained environments, innovative use of available materials can achieve excellent outcomes while potentially reducing long term healthcare burden through prevention of revision surgery.
References
- 1.Sukhonthamarn K, Grosso MJ, Sherman MB, Restrepo C, Parvizi J. Risk factors for unplanned admission to the intensive care unit after elective total joint arthroplasty. J Arthroplasty 2020;35:1937-40. [Google Scholar | PubMed]
- 2.Learmonth ID, Young C, Rorabeck C. The operation of the century: Total hip replacement. Lancet 2007;370:1508-19. [Google Scholar | PubMed]
- 3.Ani L, Radford Z, Rubin LE. Managing native hip protrusio: Simplified classification and surgical recommendations. Osteology 2023;3:33-46. [Google Scholar | PubMed]
- 4.Li X, Pan BQ, Wu XY, Fu M, Liao WM, Wu CH, et al. Impaction bone grafting combined with titanium mesh for acetabular bone defects reconstruction in total hip arthroplasty revision: A retrospective and mini review study. Orthopaed Surg 2022;14:902-10. [Google Scholar | PubMed]
- 5.Nessler JM, Nessler JP. The patient with chronic total hip arthroplasty dislocations: A case series of five patients who underwent revision tha using polypropylene mesh for capsular reconstruction. Arthroplast Today 2020;6:655-61. Erratum in: Arthroplast Today 2022;15:224. [Google Scholar | PubMed]
- 6.Abdelaal AA, Khalifa AA. Iatrogenic paprosky type 2 C acetabular defect, reconstruction by metal mesh, femoral head bulk allograft and a cemented cup, a case report. J Orthop Rep 2022;1:100037. [Google Scholar | PubMed]
- 7.Kandhari VK, Desai MM, Bava SS, Wade RN. Avascular necrosis of acetabulum: The hidden culprit of resistant deep wound infection and failed fixation of fracture acetabulum - a case report. J Orthop Case Rep 2015;5:36-9. [Google Scholar | PubMed]
- 8.Bobade SM, Page A. Total hip arthroplasty for hip arthritis with protrusio acetabuli using autograft reconstruction and metal wire mesh. Med J DY Patil Univ 2013;6:428-31. [Google Scholar | PubMed]
- 9.Yang C, Zhu K, Dai H, Zhang X, Wang Q, Wang Q. Mid- to Longterm Follow-up of Severe Acetabular Bone Defect after Revision Total Hip Arthroplasty Using Impaction Bone Grafting and Metal Mesh. Orthop Surg. 2023 Mar;15(3):750-757. [Google Scholar | PubMed]
- 10.Ishizu H, Shimizu T, Sasazawa F, Takahashi D, Terkawi MA, Takahashi K, Ohashi Y, Kanayama M, Iwasaki N. Comparison of re-revision rate and radiological outcomes between Kerboull-type plate and metal mesh with impaction bone grafting for revision total hip arthroplasty. BMC Musculoskelet Disord. 2023 Feb 20;24(1):134. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Determining the Accuracy of Acetabular Cup Size using Acetate Templates on Digital Radiographs in Patients Undergoing Total Hip Replacement
June 1, 2026 Determining the Accuracy of Acetabular Cup Size using Acetate Templates on Digital Radiographs in Patients Undergoing Total Hip Replacement June 1, 2026 Achieving Safe Zone Cup Positioning in Total Hip Arthroplasty using Anatomical Landmarks: A Prospective Computed Tomography-based Evaluation
June 1, 2026 Achieving Safe Zone Cup Positioning in Total Hip Arthroplasty using Anatomical Landmarks: A Prospective Computed Tomography-based Evaluation December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes
December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience
August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience