
[box type=”bio”] What to Learn from this Article?[/box]
Painful swelling of Achilles tendons? Diagnosis and management.
Case Report | Volume 4 | Issue 4 | JOCR Oct-Dec 2014 | Page 40-43 | Sastri VRK, Ravindranath VS, Metikala S, Kumar M. DOI: 10.13107/jocr.2250-0685.223
Authors: Sastri VRK [1], Ravindranath VS [1], Metikala S [2], Kumar M [1]
[1] Department of Orthopaedics and Traumatology, Osmania Medical College and General Hospital, Hyderabad. Andhra Pradesh – 500012, India
[2] Department of Orthopaedics, Sri Venkateswara Orthopaedic Hospital, 1/100 & 1/101, George Reddy Street, Yerramukkapalli, Kadapa, A.P., India. PIN– 516004. India.
Address of Correspondence:
Dr. Sreenivasulu Metikala, Orthopaedics, Sri Venkateswara Orthopaedic Hospital, 1/100 & 1/101, George Reddy Street, Yerramukkapalli, Kadapa, Andhra Pradesh – 516004. India. Email: orthoseenu@yahoo.com
Abstract
Introduction: Cerebrotendinous xanthomatosis is a very rare disorder of cholesterol metabolism with autosomal recessive inheritance. It can present to the out-patient clinics of orthopaedic department with painful and swollen tendoachilles on one or both sides. It is commonly mistaken for a local disorder and excision may be recommended without realizing its systemic nature.
Case Report: We find such a rare and perplexing case in a 19 year boy who presented with painful swellings of both achilles tendons causing signification limitation of walking distance. This was initially interpreted as a localized benign disorder and was offered surgical treatment. Excision of the swollen achilles tendon followed by reconstruction using peroneus brevis tendon was done, first on the more symptomatic right side. The diagnosis of cerebrotendinous xanthomatosis was made retrospectively after histopathological as well as biochemical analyses and appropriate medical therapy was initiated.
Conclusion: Cerebrotendinous xanthomatosis commonly manifests with bilateral swollen tendoachilles, which is actually a part of systemic pathology with poor prognosis. High suspicion is warranted and surgical excision should not be the primary option without the confirmation of the cause. A detailed history with clinical assessment followed by the laboratory investigations certainly leads to the correct diagnosis. The treatment is more of medical means and appropriate medication can even retard the disease progression, if initiated early in life.
Keywords: Cerebrotendinous xanthomatosis; bilateral xanthomas; tendoachilles.
Introduction
Cerebro-tendinous xanthomatosis (CTX) is a rare disorder of cholesterol metabolism with an autosomal recessive inheritance. It is characterized by the lack of production of primary bile acids from cholesterol and accumulation of a byproduct called cholestanol in various tissues like brain, spinal cord, peripheral nerves, eyes, lungs, liver, kidneys, tendon xanthomas and bile [1]. The disease starts with chronic diarrhea and cataract in the early decades of life. The painful swellings of tendoachilles usually appear in the second decade. Full blown disorder soon follows resulting in low intelligence, convulsions and abnormal movements. Out of all, the central nervous symptoms are more disabling and the situation continues to worsen with the advancing age making them completely dependent. Here we describe a classical presentation of this rare disorder that has to be considered in the differential diagnosis of commonly occurring tendon xanthomas secondary to conditions [2,16] like familial hypercholesterolaemia and other hyperlipidemias in whom surgical excision is the correct option. Whereas the present condition is a different one with systemic nature and has poor prognosis if the diagnosis is missed. Postoperative recurrence is common if surgical excision is carried out for tendon xanthomas as happened in this case. Early diagnosis and appropriate medical therapy, instituted early in life, can not only regress the swollen tendoachilles but also controls the cerebral symptoms and arrests the disease progression [2].
Case Report
A 19 year old boy presented with bilateral slow growing and painful swellings of his achilles tendons of 4 year duration. On clinical examination each swelling was of size 5×2 cm, firm, nodular, tender and localized to the distal portion of the tendoachilles just above its insertion point to the calcaneal tuberosity (Fig. 2). He was more symptomatic on the right side. He was initially advised rest, analgesics and foot wear modification. However, the symptoms did not subside and the situation worsened resulting in significant disability with limitation of his walking distance. Initial radiographs of both ankles showed homogenous soft tissue shadow in the lower halves of tendoachilles (Fig. 3). Magnetic resonance imaging showed localized homogenous hyper intense signals with fusiform swellings of tendoachilles (Fig. 4). Surgical excision was offered and the right sided one was selected first as it was more symptomatic. The swollen tendinous portion measuring 6×3 cm was excised (Fig. 5) followed by reconstruction using the ipsilateral peroneus brevis tendon. Immediate and early post-operative period was uneventful. Biopsy of the excised specimen revealed it to be a xanthoma characterized by the accumulation of mononuclear cells with foamy cytoplasm and multinucleated giant cells with high concentration of cholestanol. Thus a diagnosis of cerebro-tendinous xanthomatosis was made. On detailed retrospective inquiry, he had surgery for bilateral juvenile cataracts at the age of 8, along with history of chronic intractable diarrhea. He was coherent and co-operative but slow cerebrated with low intelligence. There were no central nervous system symptoms like convulsions, abnormal gait or incoordination of movements. Family history revealed that he was a child of a consanguineous marriage. Other sibling, a girl was normal. He was short statured measuring 144 cm in height (Fig. 1), thin built with a peculiar yellow conjunctiva. Hematological and biochemical investigations including liver function tests, lipid profile, thyroid function tests and ultrasound examination of abdomen were normal. A special test – serum cholestanol level was elevated to 4.37 mg/dL (normal value: 0.02-0.12 mg/dL). Based on the clinical picture, pathological and serological analysis, the diagnosis of cerebro-tendinous xanthomatosis was confirmed and was kept on medical therapy with chenodeoxycholic acid (CDCA), a synthetic bile acid. RESULT: He was kept under regular follow up with neurologic and neuropsychological evaluation, musculoskeletal examination and serum cholestanol estimation. He started to improve after 3 months of continued medication. According to the latest follow up of 23 months, he achieved complete improvement in his mental status and normal values of serum cholestanol. The pain on the left (non-operated) tendoachilles disappeared completely although swelling persisted. His walking distance improved. However, had reappearance of the swelling in the reconstructed tendon on the right side, although was not painful (Fig. 6).
Discussion
Cerebrotendinous xanthomatosis (CTX) is a rare genetic metabolic disorder of cholesterol and bile acid metabolism that results in systemic and neurologic abnormalities [1,4] The primary enzymatic defect is in mitochondrial sterol 27-hydroxylase, a key enzyme in the complicated process of bile acid synthesis from cholesterol [2,7]. Defects in this enzyme result in decreased synthesis of primary bile acids, this, in turn disrupts feedback regulation on cholesterol 7-alpha-hydroxylase, which is the rate limiting step in bile acid synthesis [1,6]. Therefore, bile acid precursor – cholestanol accumulates in various tissues. Deposition of cholestanol in the central nervous system (the brain and spinal cord), muscles (including the heart and eye-lens), tendons, blood vessels and other tissues results in a degenerative process that worsens over time unless treated [3,4,5]. The disease was first described in 1937 by Van Bogaert and his colleagues [3]. In 1968, Menkes et al described the accumulation of cholestanol, the primary metabolite found in elevated concentrations in cerebrotendinous xanthomatosis, in tissues of the CNS [4]. In 1971, Salen found that chenodeoxycholic acid (CDCA), an important bile acid, was virtually absent in patients with clinical symptoms of the disease [5]. This led to successful trials of therapy with CDCA replacement by Salen and colleagues in 1975 [6]. In 1980, defects in mitochondrial 27-hydroxylase were implicated in the biochemical pathophysiology of the disease by Oftebro et al [7]. In 1991, mutations in the gene CYP27A1 were discovered as causative [8,9,10]. Since then, more than 50 mutations have been implicated. The clinical manifestations are due to lack of bile acid synthesis and accumulation of bile acid precursors. Morbidity begins with intractable diarrhea, with onset typically in infancy due to defect in the synthesis of bile acids. The diarrhea continues through adulthood if left untreated [11]. Neonatal or infantile hepatitis and prolonged jaundice have been described [12]. Juvenile cataracts seen as early as 5-6 years of age, may be the presenting sign [13], resulting in vision abnormalities due to accumulation of cholestanol in lens tissues. Xanthomas are rarely seen before the second decade. They are usually found on the achilles tendons but may also be found on the patella, elbow, hand, and neck tendons. They have also been reported on the parenchyma of the lungs and brain, as well as in the bones. Musculoskeletal xanthomas can cause motor restriction and joint deformities, resulting in ambulation disabilities. Vascular abnormalities such as premature atherosclerosis (especially in the carotid and coronary vessels) due to excess cholestanol deposition can lead to stroke and myocardial infarction. Significant neurologic impairment with low intelligence, seizures, dementia and extra pyramidal dysfunction typically begins in the third decade of life and progress until death, if left untreated. This is because of the accumulation of high serum cholestanol levels for a prolonged period which have a toxic effect on the neurons and myelinated axons leading to atrophy and secondary demyelination [14]. If CTX is not diagnosed, the life expectancy is into the fifth and sixth decades; however, deaths have been reported even in the second and third decades. This is a progressive and terminal disease if left untreated. Treated patients may have a normal life span. The differential diagnosis of tendon xanthomatosis includes familial hypercholesterolemia, leukodystrophy and sitosterolemia. These patients have accelerated atherosclerosis with tendon xanthomata, but absence of neurological symptoms and diarrhea differentiates them from CTX [15]. Our patient showed all the typical features of this rare disorder like infantile diarrhea, juvenile cataracts, tendoachilles xanthomata, low intelligence and short stature except seizures and symptoms of extra pyramidal dysfunction. The serum cholestanol level was typically elevated to 4.37 mg/dL (the normal levels range from 0.02-0.12 mg/dL). The treatment of choice in cerebrotendinous xanthomatosis is chenodeoxycholic acid (CDCA) replacement therapy. The recommended dose is 15 mg/kg/day orally in 3 divided doses would normalize the cholestanol levels after as little as 4 months of treatment. Neurological, gastrointestinal and musculoskeletal symptoms improve gradually along with the feeling of general well-being. The common order of presentation of this rare disease, as explained, is infantile intractable diarrhea, juvenile cataracts, adolescent tendon xanthomas followed by adulthood neurological manifestations. Appearance of tendon xanthomas is an important clinical hallmark of the disease. If tendon xanthomas are not present, a diagnosis of CTX often will not be made, unless biochemical tests are performed. So all the patients with achilles xanthomas need to be evaluated with a detailed history, clinical examination, followed by serum cholestanol estimation. Surgical temptation in the form of excision of the swollen achilles tendons may miss a dreadful, yet treatable condition.
Conclusion
There are different causes of tendoachilles swellings, of which one of the rare but a medically treatable condition is cerebrotendinous xanthomatosis. Early recognition of this entity is crucial as it has got an effective medical therapy that can prevent further progression and even reverse the disease manifestations. Surgery should not be the option for the tendon xanthomata without the confirmation of the cause as it could be a part of a systemic pathology.
Clinical Message
Among the different causes of tendoachilles swellings, cerebrotendinous xanthomatosis, although rare yet is a medically treatable condition. Early recognition is indispensable as it has an effective medical therapy which can not only prevent further progression but can even reverse the disease manifestations. Surgery should not be the option for the tendon xanthomata without the confirmation of its etiology as it could be a part of a systemic pathology.
References
1. Kuriyama M, Fujiyama J, Yoshidome H, et al. Cerebrotendinous Xanthomatosis: clinical and biochemical evaluation of eight patients and review of literature. J Neurol Sci 1991;102:225-32.
2. Berginer VM, Berginer J, Korczym AD, Tadmor R. Magnetic Resonance Imaging in CTX: a prospective clinical and neuroradiological study. J Neurol Sci 1994;122:102-8.
3. Van Bogaert L, Scherer HJ, Epstein E. Une forme cerebrale de la cholesterinose generalisee [dissertation/master’s thesis]. Paris: Masson et Cie. 1937.
4. Menkes JH, Schimschock JR, Swanson PD.Cerebrotendinous xanthomatosis. The storage of cholestanol within the nervous system.
Arch Neurol. Jul 1968;19(1):47-53.
5. Salen G.Cholestanol deposition in cerebrotendinous xanthomatosis. A possible mechanism. Ann Intern Med. Dec 1971;75(6):843-51.
6. Salen G, Meriwether TW, Nicolau G. Chenodeoxycholic acid inhibits increased cholesterol and cholestanol synthesis in patients with cerebrotendinous xanthomatosis. Biochem Med. Sep 1975;14(1):57-74.
7. Oftebro H, Björkhem I, Skrede S, Schreiner A, Pederson JI. Cerebrotendinous xanthomatosis: a defect in mitochondrial 26-hydroxylation required for normal biosynthesis of cholic acid. J Clin Invest. Jun 1980;65(6):1418-30.
8. Clayton PT, Verrips A, Sistermans E, Mann A, Mieli-Vergani G, Wevers R. Mutations in the sterol 27-hydroxylase gene (CYP27A) cause hepatitis of infancy as well as cerebrotendinous xanthomatosis. J Inherit Metab Dis. Oct 2002;25(6):501-13.
9. Gallus GN, Dotti MT, Federico A. Clinical and molecular diagnosis of cerebrotendinous xanthomatosis with a review of the mutations in the CYP27A1 gene. Neurol Sci. Jun 2006;27(2):143-9.
10. Sugama S, Kimura A, Chen W, et al.Frontal lobe dementia with abnormal cholesterol metabolism and heterozygous mutation in sterol 27-hydroxylase gene (CYP27). J Inherit Metab Dis. Jun 2001;24(3):379-92.
11. Moghadasian MH, Salen G, Frohlich JJ, Scudamore CH. Cerebrotendinous xanthomatosis: a rare disease with diverse manifestations. Arch Neurol. Apr 2002;59(4):527-9.
12. Cruysberg JR, Wevers RA, Tolboom JJ.Juvenile cataract associated with chronic diarrhea in pediatric cerebrotendinous xanthomatosis. Am J Ophthalmol. Nov 15 1991;112(5):606-7.
13. Monson DM, DeBarber AE, Bock CJ, Anadiotis G, Merkens LS, Steiner RD, et al. Cerebrotendinous xanthomatosis: a treatable disease with juvenile cataracts as a presenting sign. Arch Ophthalmol. Aug 2011;129(8):1087-8.
14. Dotti MT, Federico A. Cerebrotendinous xanthomatosis as a multisystem disease mimicking premature ageing. Dev Neurosci. 1991;13(4-5):371-6.
15. Vadapalli S. Cerebrotendinous xanthomatosis. Indian J Orthop. 2013 Mar;47(2):200-3.
| How to Cite This Article: Sastri VRK, Ravindranath VS, Metikala S, Kumar M.Bilateral Xanthomas of Tendoachilles in A Patient of Cerebrotendinous Xanthomatosis – A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2014 Oct-Dec;4(4): 40-43. Available from: https://www.jocr.co.in/wp/2014/10/14/2250-0685-223-fulltext/ |
(Figure 1)|(Figure 2)|(Figure 3)|(Figure 4)|(Figure 5)|(Figure 6)
[Abstract] [Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 October 14, 2014 Bilateral Xanthomas of Tendoachilles in A Patient of Cerebrotendinous Xanthomatosis – A Rare Case Report and Review of Literature
October 14, 2014 Bilateral Xanthomas of Tendoachilles in A Patient of Cerebrotendinous Xanthomatosis – A Rare Case Report and Review of Literature February 5, 2012 Osteotomy and Re-fixation for treatment of Malunited Greater Tuberosity of Humerus. Case 5 – Jan -Mar 2012. Journal of Orthopaedic Case Reports
February 5, 2012 Osteotomy and Re-fixation for treatment of Malunited Greater Tuberosity of Humerus. Case 5 – Jan -Mar 2012. Journal of Orthopaedic Case Reports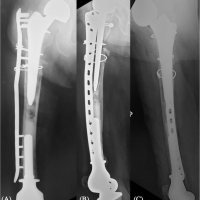 August 10, 2023 Awareness of Stress Concentration Points for Prevention and Management of Periprosthetic Fractures Following Plate Installation Reinforcement: A Case Report
August 10, 2023 Awareness of Stress Concentration Points for Prevention and Management of Periprosthetic Fractures Following Plate Installation Reinforcement: A Case Report May 10, 2019 Reverse Segond Fracture without Posterior Cruciate Ligament Injury – A report of Two Cases and Review of the Literature
May 10, 2019 Reverse Segond Fracture without Posterior Cruciate Ligament Injury – A report of Two Cases and Review of the Literature