
Elbow dislocation associated with severely displaced radial neck fracture and ulnar diaphyseal fracture in a child has never been reported before.
Dr. Pierre-Louis Docquier, Department of Orthopaedic Surgery, Avenue Hippocrate, 10, Cliniques Universitaires Saint-Luc, B-1200 Brussels, Belgium. E-mail: pierre-louis.docquier@uclouvain.be
Abstract
Introduction: Association of elbow dislocation, radial neck fracture (RNF), and ulnar shaft fracture has not been reported previously in the pediatric population.
Case Report: This 11-year-old girl fell from her height. She presented a severely displaced RNF, a greenstick fracture of the proximal ulnar shaft, and a posterior elbow dislocation.
Conclusion: This article describes a very rare case, shows a possible treatment, and presents the follow-up with a final good result.
Keywords: Elbow fracture-dislocation, pediatric, radial neck fracture.
Despite elbow dislocation, radial neck fracture (RNF) and ulnar diaphyseal fracture are separately quite common in pediatric patients; the association of the three has never been reported previously.
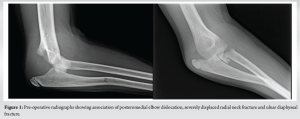
We report the case of an 11-year-old girl who fell from her height. She had a medical history of right elbow dislocation 3 years before. She had no other traumatic history. The patient tripped over a doorframe, fell, and landed on her right hand with an outstretched elbow. She went to the emergency room, where a radiograph was performed (Fig. 1). The radiograph showed an unusual association of posterior elbow dislocation, a grade 4b RNF (according to Judet), and a greenstick fracture of the proximal ulnar shaft. This association is not a terrible triad injury of the elbow as the coronoid is not injured and we have a RNF instead of a radial head fracture [1]. It is not a Monteggia association, as the ulna is not dislocated in the Monteggia.
After closed reduction of the dislocation, percutaneous anterograde nailing of the ulna was performed with a 2.5 mm-Kirschner wire, associated with a percutaneous anterograde nailing of the radius with a 1.5 mm-Kirschner wire with temporary arthrodesis of the humero-radial joint (Fig. 2). A 6-week long arm cast was applied. Six weeks later, the cast and the Kirschner wires were removed. Physiotherapy 4 times a week was started associated with a daily 30-min arthromotor (Kinetec) to help restore the range of motion of the elbow and forearm.

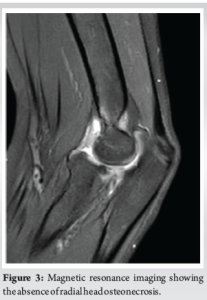
Six months after traumatism, magnetic resonance imaging was performed and showed no sign of avascular necrosis of the radial head (Fig. 3). The range of motion was still limited at that time, with a 30° lack of elbow extension and pronation limited to 20°. Radiograph showed persisting slight anterior subluxation of the radial head. A night dynamic elbow extension brace (Ultraflex) was applied to improve extension.
Fourteen months after traumatism, the patient had improved the elbow mobility, with 140° of flexion, only a 5°-lack of extension, full supination, and still 20°-lack of pronation. The radiograph (Fig. 4) showed a good healing of the fracture but persisting slight anterior subluxation of the radial head. The patient and her parents were very satisfied with the evolution of the range of motion and the absence of more severe complications (radial head necrosis, ankylosis).

The simultaneous association of a RNF, a greenstick proximal ulnar shaft fracture, and a posterior elbow dislocation has never been reported before. The treatment is not easy.
In the pediatric population, unlike in the adult population, a RNF is more likely to happen instead of a radial head fracture [2]. The RNF can be classified according to the classification of Judet and Metaizeau depending on the angulation of the radial neck displacement. If the RNF is angulated more than 30°, a reduction is preferred [2-4]. Closed reduction is preferred as an open reduction exposes to the radial head osteonecrosis. In this case, a reduction with Kirschner wire seems to be a good option [4-6], or a reduction with elastic stable intramedullary nails [7].
The greenstick fracture of the proximal ulnar shaft requires a specific treatment as there is a significant relation between the fracture angulation and the prono-supination [8]. If there is an important angulation, a reduction must be done before immobilization.
The elbow dislocation is a relatively rare injury in the pediatric population [9]. It is often accompanied by one or multiple fractures. An isolated dislocation should be reduced in the emergency room under sedation and treated orthopedically, but an elbow fracture-luxation needs to treat the associated fracture at the same time [10].
The presented case shows the complexity of an unreported association of injuries. All injuries have their own specific guidelines or recommendations and require specific attention to the different imperatives of each lesion. Immobilization is key for bone healing, but it is important to quickly start to mobilize the elbow to prevent ankylosis.
Association of elbow dislocation, RNF, and ulnar diaphyseal fracture has not been reported before. The reported treatment led to a very good functional result. It could help another orthopedic surgeon facing a comparable case.
References
- 1.Kani KK, Chew FS. Terrible triad injuries of the elbow. Emerg Radiol 2019;26:341-7. [Google Scholar | PubMed]
- 2.Kim HH, Gauguet JM. Pediatric elbow injuries. Semin Ultrasound CT MR 2018;39:384-96. [Google Scholar | PubMed]
- 3.Trabelsi A, Khalifa MA, Brahem R, Jedidi M, Bouattour K, Osman W, et al. Radial neck fracture in children: Anatomic and functional results of Metaizeau technique. Pan Afr Med J 2020;36:144. [Google Scholar | PubMed]
- 4.Cossio A, Cazzaniga C, Gridavilla G, Gallone D, Zatti G. Paediatric radial neck fractures: One-step percutaneous reduction and fixation. Injury 2014;45 Suppl 6:S80-4. [Google Scholar | PubMed]
- 5.Sapkota K, Ranjeet N, Onta PR, Thapa P. The outcome of radial neck fracture treated with closed/ open reduction and retrograde kirschner wires fixation in the paediatric age group. Kathmandu Univ Med J (KUMJ) 2022;20:467-71. [Google Scholar | PubMed]
- 6.Çevik N, Cansabuncu G, Akalın Y, Otuzbir A, Öztürk A, Özkan Y. Functional and radiological results of percutaneous K-wire aided Métaizeau technique in the treatment of displaced radial neck fractures in children. Acta Orthop Traumatol Turc 2018;52:428-34. [Google Scholar | PubMed]
- 7.Xia A, You C, Han J, Wu D, Xia Y, Wang J. Comparison of different treatments for children with radial neck fracture and analysis of prognostic factors. Arch Orthop Trauma Surg 2022;142:3301-9. [Google Scholar | PubMed]
- 8.Franklin CC, Robinson J, Noonan K, Flynn JM. Evidence-based medicine: Management of pediatric forearm fractures. J Pediatr Orthop 2012;32 Suppl 2:S131-4. [Google Scholar | PubMed]
- 9.Hyvönen H, Korhonen L, Hannonen J, Serlo W, Sinikumpu JJ. Recent trends in children’s elbow dislocation with or without a concomitant fracture. BMC Musculoskelet Disord 2019;20:294. [Google Scholar | PubMed]
- 10.Lewallen L, Elliott ME, McIntosh A, Ho CA. Pediatric elbow dislocations and associated fractures. Children (Basel) 2023;10:993. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2021 Late Presenting Pediatric Radial Neck Fracture: A Case Report and Review of the Literature
January 10, 2021 Late Presenting Pediatric Radial Neck Fracture: A Case Report and Review of the Literature May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report
May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series
May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series April 1, 2026 A Rare Case of Chronic Pan-Diaphyseal Osteomyelitis of the Fibula in a Child Treated by Near Total Fibulectomy: A Case Report
April 1, 2026 A Rare Case of Chronic Pan-Diaphyseal Osteomyelitis of the Fibula in a Child Treated by Near Total Fibulectomy: A Case Report