
Magnetic resonance imaging appearances are nuanced and do not always reflect expected pathology.
Dr. Spencer M. Stein, Department of Orthopedic Surgery, NYU Langone Health, New York, United States. E-mail: spencer.stein@nyulangone.org
Abstract
Introduction: Anomalous medial menisci are rare entities compared to their lateral counterparts. These anomalies include atypical insertions, most commonly into the anterior cruciate ligament, and discoid variants among others. This case adds to the literature on anomalous medial menisci with the presentation of a variant not described in the literature before.
Case Report: Our patient is a 38-year-old female who presented to the outpatient orthopedic clinic complaining of right knee pain in the setting of a traumatic kneeling event. She had a past medical history of asthma, polycystic ovary syndrome, and anxiety, but no surgical history related to the knee. She underwent magnetic resonance imaging identified what appeared to be a bucket-handle medial meniscus tear. The patient was brought to the operating room where diagnostic arthroscopy revealed a radial tear at the posterior horn of the medial meniscus as well as an anomalous connection between the anterior and posterior roots. The band specifically ran from the posterior horn of the medial meniscus, then superiorly and along the posterior cruciate ligament, and ultimately attached to the anterior horn of the medial meniscus in an “O” shape. In addition, a large patellofemoral plica was identified overlying the lateral femoral condyle. The tear, plica, and anomalous band were all debrided. The patient was progressing well on her most recent 7-month follow-up visit.
Conclusion: To our knowledge, this is the only reported case of such an anomaly. This case highlights the fact that there are likely other unidentified meniscal variants, and if they are not correctly identified on imaging, it could lead to patient mismanagement. Further research is needed into these variants.
Keywords: Anomalous medial meniscus, plica, bucket-handle tear.
The menisci play an important role in shock absorption and stabilization of the knee joint [1,2]. Given the limited regenerative capacity of menisci, the goal of meniscal surgery is to preserve as much of the normal meniscal tissue as possible. However, this can be particularly challenging when anomalous meniscal tissue is encountered, as it may mimic pathological tears and complicate diagnosis and treatment decisions. There have been various types of meniscal anomalies documented in the literature [3-6]. Among these, the most reported have been lateral discoid menisci, which have notably been seen more commonly in Asian populations [7]. In contrast, abnormalities of the medial meniscus are rare and can include discoid variants [8-10], congenital hypoplasia [11], underdevelopment of the anterior horn [12], and absence of bony attachment of the posterior horn to the femoral condyle [13]. More recently, there have been case reports of patients who have medial menisci with anomalous insertions on the anterior cruciate ligament (ACL) and discoid medial menisci that are completely coalesced with the ACL [14,15]. However, to date, there have been no case reports of an anomalous medial meniscus with tissue arising from the posterior horn/root that extends along the posterior cruciate ligament (PCL) to the anterior horn, mimicking a bucket-handle medial meniscus tear. The goal of this case report is to present a case of an anomalous medial meniscus extending from the posterior horn/root along the PCL and to the anterior horn mimicking an “O” shape, review the literature, and present treatment for this patient.
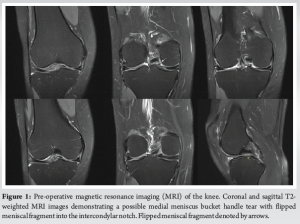
We present the case of a 38-year-old female who presented to the outpatient orthopedic clinic complaining of right knee pain. She had a past medical history of asthma, polycystic ovary syndrome, and anxiety, but no surgical history related to the knee. About 2 weeks before presentation, the patient experienced a sharp onset of knee pain after she knelt onto the affected knee. In addition to pain, the patient reported swelling, popping, and a locking sensation in the knee. She denied any prior trauma or injury to the knee, numbness, or tingling in either leg. She also denied any history of knee pain, popping, clicking, or catching before the kneeling event. On physical examination, there was a moderate effusion present and medial joint line tenderness as well as a positive medial McMurray test. Active and passive range of motion demonstrated one-degree loss of extension compared to the contralateral side. Her knee was stable to anterior, posterior, and varus/valgus stress. Patella examination was within normal limits. Magnetic resonance imaging (MRI) was performed and showed a medial meniscal fragment spanning from the posterior horn to the anterior horn within the intercondylar notch that was consistent with a flipped bucket handle tear (Fig. 1).
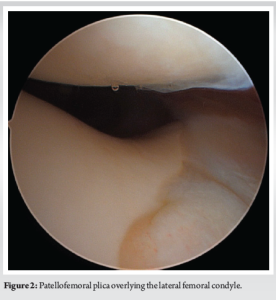
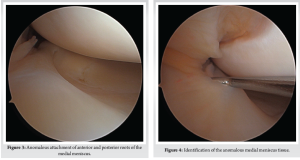
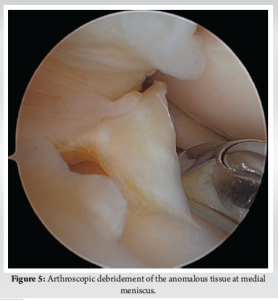
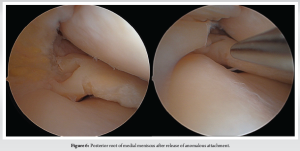
Diagnostic arthroscopy was performed secondary to pain, mechanical symptoms, and the diagnosis of a bucket-handle meniscus tear. Entry into the patellofemoral compartment revealed a large suprapatellar plica in contact with the lateral femoral condyle (Fig. 2). Within the medial compartment, diagnostic arthroscopy revealed the anomalous connection between the anterior and posterior horns (Fig. 3 and 4) and a radial tear at the posterior meniscus. The anomalous band was clearly a distinct structure from the medial meniscus with probing and became entrapped upon full extension of the knee. The band specifically ran from the posterior horn of the medial meniscus, superiorly, along the PCL, and ultimately attached to the anterior horn of the medial meniscus in an “O” shape. No chondral pathology was detected. A partial meniscectomy was performed to address the posterior radial tear located in the white–white zone, followed by debridement and removal of the anomalous attachment (Fig. 5 and 6).
After confirming there were no lesions in the lateral compartment, the large suprapatellar plica was excised. Post-operative recovery included immediate weight bearing on the affected extremity with physical therapy. The patient progressed well with physical therapy and has returned to full function, activities of daily living, and is pain free. Her most recent follow-up was at 7 months post-operatively, and she reported doing well with no issues.
Anomalies of the medial meniscus are uncommon compared to anomalies of the lateral meniscus, and they include discoid variants, hypoplasia of the anterior horn, and anomalous insertion of the anterior horn [13]. There have been limited case studies published involving anomalies of the posterior horn of the medial meniscus. One case describes a fibro-cartilaginous fold that covers the medial femoral condyle (but reports a normal posterior horn), and another case describes a fibrous band arising from the posterior horn, connecting it to the ACL [16,17]. Mariani et al. reported the first published case involving a combined anomaly of the posterior and anterior roots of the medial meniscus [13]. However, this case did not describe an anomalous connection between the horns, forming an “O” shape, and mimicking a bucket handle tear. Most reported anomalies of the medial meniscus involve insertion into the ACL, not the PCL. The overall prevalence of anomalous insertion of the medial meniscus into the ACL is 1.2–2.3%[18]. Due to the relatively high prevalence of this morphology, a classification system exists that breaks down anomalous insertion of the medial meniscus into the ACL. These three distinct subcategories are based on insertion location and include: Type 1 (into the lower portion), type 2 (into the middle portion), and type 3 (into the proximal portion; intercondylar notch), with type 2 being the most common [19]. A medial discoid meniscus was first described in 1941, about 50 years after a lateral discoid meniscus was first described by Tachibana in 1889 [20]. Since discoid menisci became a topic of research, it became abundantly clear that a lateral discoid meniscus is significantly more common than the rare medial discoid meniscus. In 10,000 meniscectomies performed by Smillie, 467 had a lateral discoid meniscus compared to just those that had a medial discoid meniscus[21]. Furthermore, in 14,731 menisci examined by Dickason et al., 10 of 8,040 (0.12%) medial menisci were discoid, whereas 102 of 6,691 (1.5%) lateral menisci were discoid [22]. Some controversy still exists regarding the pathogenesis of discoid menisci: Two predominant existing theories are Smillie’s embryological theory and Kaplan’s developmental and biomechanical hypothesis [23]. Smillie posited that a discoid meniscus is a result of an arrest in the normal development of the meniscus during embryogenesis [21,24]. Kaplan, on the other hand, proposed that abnormal mechanical forces during knee development could lead to the persistence of the discoid shape [25]. This hypothesis is supported by the observation that the lateral meniscus, which is more frequently affected by the discoid variant, covers a larger surface area of the tibial plateau during fetal development, making it more susceptible to abnormal mechanical stresses [24,25]. Given that medial discoid menisci are extremely rare, only small case series have been published in the literature. Our case, however, differs from all described anomalies in the literature as the meniscal band arising from the posterior horn of the medial meniscus connected to the anterior horn of the medial meniscus, thereby forming an “O” shape. A musculoskeletal 162 radiologist and fellowship-trained sports medicine orthopedic surgeon identified the pathology on MRI as a bucket-handle medial meniscus tear. There is literature that describes the MRI appearance of an anomalous insertion of the medial meniscus into the ACL, where there is a low signal intensity band that goes from the anterior horn of the medial meniscus, covering the ACL, and into the intercondylar notch [19,26]. That appearance, however, does not mimic that of a bucket-handle meniscus tear. The MRI appearance of our patient’s knee was likely complicated by the fact that there was an anomalous connection between the anterior and posterior roots of the medial meniscus, which appeared like a flipped meniscal fragment. An interesting aspect of this case was the lack of mechanical or painful symptoms present before the kneeling event, despite the anomalous meniscus still existing in the patient’s knee. It is very possible that this one event caused a mechanical disturbance of the anomalous tissue, displacing it into a position it was not in before the kneeling event, thereby causing new symptoms. However, it is not completely known why this one kneeling event precipitated symptoms. Finally, a large patellofemoral plica overlying the lateral femoral condyle was identified intraoperatively. This may have been an incidental finding but could have contributed as a source of pain. It also could have a potential association with the anomalous meniscus. However, there is no literature identifying an association between an anomalous medial meniscus and patellofemoral plica. Further investigation into this possible association is warranted.
Anomalous medial menisci are rare, and despite limited case studies, to our knowledge, there have been no published cases of an anomalous medial meniscus connecting the anterior and posterior horns, forming an “O” shape. The MRI appearance mimicked that of a bucket-handle meniscus tear. Despite this, the patient received appropriate care and is now symptom-free.
The anomalous medial meniscus described above is an important variant to recognize as it mimics a pathology that typically requires urgent surgical attention. Further research is warranted on techniques for identifying these variants on MRI.
References
- 1. Mameri ES, Dasari SP, Fortier LM, Verdejo FG, Gursoy S, Yanke AB, et al. Review of meniscus anatomy and biomechanics. Curr Rev Musculoskelet Med 2022;15:323-35. [Google Scholar] [PubMed]
- 2. Flandry F, Hommel G. Normal anatomy and biomechanics of the knee. Sports Med Arthrosc Rev 2011;19:82-92. [Google Scholar] [PubMed]
- 3. Jose J, Buller LT, Rivera S, Carvajal Alba JA, Baraga M. Wrisberg-variant discoid lateral meniscus: Current concepts, treatment options, and imaging features with emphasis on dynamic ultrasonography. Am J Orthop (Belle Mead NJ) 2015;44:135-9. [Google Scholar] [PubMed]
- 4. Monllau JC, León A, Cugat R, Ballester J. Ring-shaped lateral meniscus. Arthroscopy 1998;14:502-4. [Google Scholar] [PubMed]
- 5. Xu Z, Chen D, Shi D, Dai J, Yao Y, Jiang Q. Evaluation of posterior lateral femoral condylar hypoplasia using axial MRI images in patients with complete discoid meniscus. Knee Surg Sports Traumatol Arthrosc 2016;24:909-14. [Google Scholar] [PubMed]
- 6. Niu EL, Lee RJ, Joughin E, Finlayson CJ, Heyworth BE. Discoid meniscus. Clin Sports Med 2022;41:729-47. [Google Scholar] [PubMed]
- 7. Yang SJ, Zhang MZ, Li J, Xue Y, Chen G. A reliable, ultrasound-based method for the diagnosis of discoid lateral meniscus. Arthroscopy 2021;37:882-90. [Google Scholar] [PubMed]
- 8. Zheng ZR, Ma H, Yang F, Yuan L, Wang GD, Zhao XW, et al. Discoid medial meniscus of both knees: A case report. World J Clin Cases 2022;10:9020-7. [Google Scholar] [PubMed]
- 9. Anderson KG, Carsen S, Stinson Z, Kushare I, Finlayson CJ, Nault ML, et al. Medial discoid meniscus in children: A multicenter case series of clinical features and operative results. Am J Sports Med 2023;51:1171-6. [Google Scholar] [PubMed]
- 10. Rodríguez-Rodríguez IF, Navarro-Torres-Arpi P, Dryjanski-Lerner A, Gómez-Mont-Landerreche JG, Levy-Holden GA, Gil-Orbezo F. Menisco discoide medial enpaciente pediátrico. Presentación de un caso y revisión de la literatura [Medial discoid meniscus in a pediatric patient. Case report and review of the literature]. Acta Ortop Mex 2024;38:52-6. [Google Scholar] [PubMed]
- 11. Twyman RS, Ferris BD. Congenital hypoplasia of the medial meniscus: A report of two cases. Arthroscopy 1991;7:148-50. [Google Scholar] [PubMed]
- 12. Muniraj S, Congenital Hypoplastic Meniscus with Tear. Case study. Radiopaedia. Available from: https://radiopaedia.org/cases/50251/discussion?new_full_screen_viewer=true[Last accessed on 2025 Mar 13]. [Google Scholar] [PubMed]
- 13. Mariani PP, Battaglia MJ, Torre G. Anomalous insertion of anterior and posterior horns of medial meniscus. Case report. BMC Musculoskelet Disord 2021;22:823. [Google Scholar] [PubMed]
- 14. Wang JH, Wong AK, Romanowski JR 2nd, Fu FH. Meniscus tear developed by pulling of the anomalous insertion of medial meniscus on anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 2011;19:1689-92. [Google Scholar] [PubMed]
- 15. Jin G, Xin T, Weng Z, Zhu Y, Qiu H, Liu D, et al. Symptomatic complete discoid medial meniscus completely coalesced with the anterior cruciate ligament: A case report and literature review. Orthop Surg 2022;14:2391-5. [Google Scholar] [PubMed]
- 16. Riachi A, Phaires A. An unusual deformity of the medial semilunar cartilage. J Bone Joint Surg Br 1993;45:146-7. [Google Scholar] [PubMed]
- 17. Bhagava A, Ferrari DA. Posterior medial meniscus-femoral insertion into the anterior cruciate ligament. A case report. Clin Orthop Rel Res 1998;348:176-9. [Google Scholar] [PubMed]
- 18. Getzmann JM, Bohnert L, Roos JE, Agten CA. Anomalous insertion of the medial meniscus into a triple bundle anterior cruciate ligament: A rare combination of two anatomical variants. Eur J Radiol Open 2020;7:100220. [Google Scholar] [PubMed]
- 19. Cha JG, Min KD, Han JK, Hong HS, Park SJ, Park JS, et al. Anomalous insertion of the medial meniscus into the anterior cruciate ligament: The MR appearance. Br J Radiol 2008;81:20-4. [Google Scholar] [PubMed]
- 20. Tachibana Y, Yamazaki Y, Ninomiya S. Discoid medial meniscus. Arthroscopy 2003;19:E12-8. [Google Scholar] [PubMed]
- 21. Smillie IS. Injuries of the knee joint. In: Annexe Thesis Digitisation Project 2019 Block 22. United Kingdom: The University of Edinburgh; 1946. [Google Scholar] [PubMed]
- 22. Dickason JM, Del Pizzo W, Blazina ME, Fox JM, Friedman MJ, Snyder SJ. A series of ten discoid medial menisci. Clin Orthop Relat Res 1982;168:75-9. [Google Scholar] [PubMed]
- 23. Chen LX, Ao YF, Yu JK, Miao Y, Leung KK, Wang HJ, et al. Clinical features and prognosis of discoid medial meniscus. Knee Surg Sports Traumatol Arthrosc 2013;21:398-402. [Google Scholar] [PubMed]
- 24. Turati M, Anghilieri FM, Accadbled F, Piatti M, Di Benedetto P, Moltrasio F, et al. Discoid meniscus in human fetuses: A systematic review. Knee 2021;30:205-13. [Google Scholar] [PubMed]
- 25. Kaplan EB. Discoid lateral meniscus of the knee joint; Nature, mechanism, and operative treatment. J Bone Joint Surg Am 1957;39:77-87 [Google Scholar] [PubMed]
- 26. Arjun S, Takahashi S, Tang Y, Nakane N, Yonemitsu H. MR appearance of anomalous insertion of the medial meniscus. A case report. Acta Radiol 1998;39:554-6. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Arthroscopic Management of a Bucket-Handle Acetabular Labral Tear in a Pediatric Patient: A Rare Case Report with Associated Fleck Sign
April 1, 2026 Arthroscopic Management of a Bucket-Handle Acetabular Labral Tear in a Pediatric Patient: A Rare Case Report with Associated Fleck Sign August 10, 2021 A Case Report of Tarsal Navicular Body Fracture with Lateral Ankle Ligament Complex Tear – a New Injury Combination
August 10, 2021 A Case Report of Tarsal Navicular Body Fracture with Lateral Ankle Ligament Complex Tear – a New Injury Combination September 1, 2024 Posterior Aspect Fracture of Tibia after Open Wedge Distal Tuberosity Osteotomy: A Case Report
September 1, 2024 Posterior Aspect Fracture of Tibia after Open Wedge Distal Tuberosity Osteotomy: A Case Report December 4, 2020 Surgical Management of Concomitant Proximal Tibiofibular Instability and Medial Collateral Ligament Tear: A Case Report
December 4, 2020 Surgical Management of Concomitant Proximal Tibiofibular Instability and Medial Collateral Ligament Tear: A Case Report