
Effective management of broken guidewires involves preventive techniques and minimally invasive retrieval methods, ensuring safer outcomes in hip surgeries.
Dr. Yashodhan Bhatt, Department of Orthopaedic Surgery, Pravara Rural Medical Hospital and Rural Medical College, Ahmednagar - 413736, Loni, Maharashtra, India. Email: dryashodhanbhatt@gmail.com
Abstract
Introduction: Hardware failure during orthopedic procedures is a rare but serious complication. Guidewire breakage, especially during hip surgeries, poses a risk of deep migration, potentially leading to damage to intrapelvic structures. Retrieval of a broken wire from the femoral head or acetabulum carries significant risk, including iatrogenic cartilage damage and injury to pelvic organs.
Case Report: We report a case of a 19-year-old male presenting with avascular necrosis of bilateral femoral heads (Association Research Circulation Osseous Stage II) who underwent core decompression with platelet-rich plasma injection. The guidewire used broke in the femoral head and migrated into the acetabulum during the surgery, which was successfully retrieved using a combination of over-reaming and an arthroscopic grasper.
Conclusion: Our method effectively retrieved the broken guidewire using a minimally invasive technique. Various bailout options, precautions, and prevention strategies are discussed to aid orthopedic surgeons in managing this complication safely.
Keywords: Broken hardware, core decompression, broken guidewire, avascular necrosis.
In a study of 12,601 cases, Haberal and Beyaz 2021 [1] reported orthopedic instrument breakage in 0.28% of all procedures, occurring in 0.64% of fracture fixation surgeries and 0.08% of elective orthopedic operations. The likelihood of instrument breakage was 7.44 times higher in trauma cases compared with elective procedures (P = 0.001). Among the reported incidents, 16 cases (44.4%) involved a broken K-wire, 14 (38.9%) a broken screw, and 6 (16.6%) a broken drill bit. Core decompression is a minimally invasive surgical technique primarily used in the early stages of femoral head avascular necrosis (AVN) (Ficat-Arlet/Association Research Circulation Osseous [ARCO] Stage I or II) [2]. It aims to reduce intraosseous pressure, stimulate angiogenesis, and promote bone healing [3]. The procedure involves creating tracts into the femoral head using guidewires and cannulated drills [4]. Despite its relative simplicity, complications such as iatrogenic fracture, infection, and hardware-related issues may arise. Among these, intraoperative breakage of guidewires – though rare – is a serious concern [5]. If fragments are driven into the joint cavity, acetabulum, or abdominal cavity, retrieval becomes technically demanding and time-sensitive to avoid irreversible complications, including joint damage and intrapelvic injuries [6].
A 19-year-old male presented with bilateral hip pain and gait abnormality of 1 year’s duration. He had a prior history of steroid therapy for tuberculous meningitis. Magnetic resonance imaging (MRI) revealed bilateral AVN of the femoral heads (ARCO Stage II), and he was scheduled for bilateral core decompression with platelet-rich plasma injection (Fig. 1).

Figure 1: Post-operative X-ray.
The patient was positioned supine on a traction table. A 4 mm guidewire was used to create decompression tracts. While drilling over one of the guidewires with a 4.5 mm cannulated drill bit, resistance was encountered, and upon withdrawal of the drill bit, it was noted that the guidewire had broken. Approximately 1.5 cm of the wire tip was lodged within the femoral head.
Subsequent attempts to free the broken tip using a thicker guidewire inadvertently pushed it further toward the joint cavity. Eventually, it was visualized to be lodged in the acetabulum on fluoroscopy. To retrieve the broken wire, the remaining part of the guidewire was aligned with the broken tip (Fig. 2) over which a dynamic hip screw inner reamer was gently hand-reamed (Fig. 3). This made sure the reaming did not create another tract. This maneuver facilitated mobilization of the wire but also pushed it further (Fig. 4). Finally, using an arthroscopic grasper under continuous fluoroscopic guidance, the fragment was successfully retrieved (Fig. 5).
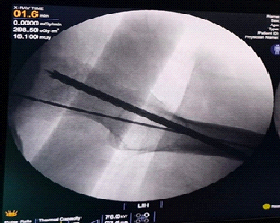
Figure 2: Broken guide wire aligned with the broken tip before trying to over-ream.
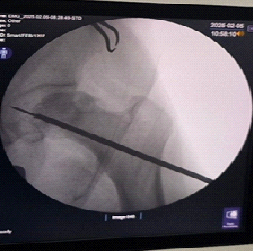
Figure 3: Guide wire pushed further inside the acetabulum cavity while trying to over-ream.
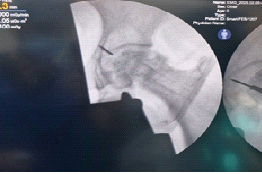
Figure 4: Broken tip migrating into the acetabulum.

Figure 5: Retrieved K-wire tip using arthroscopic grasper.
Causes of guidewire breakage
- Patient-related factors: Dense or sclerotic bone, especially in younger individuals or in AVN cases
- Implant-related factors: Reuse of guidewires; inappropriate wire diameter
- Surgical technique factors: Excessive and continuous drilling, overheating of wires, drilling at a low angle of incidence, inadvertent bending, and multiple failed attempts, increasing stress on the wire.
Retrieval techniques and bailout options
- Over-reaming
-
- Effective but risks significant bone loss and predisposes to pathological fractures. Can use an arthroscopic grasper or disc forceps for retrieval.
- 2.Pituitary forceps
-
- Useful due to the altered shape of the broken wire end (from circular to oval), which improves grip [7].
- 3. Arthroscopy
-
- Minimally invasive; however, it has a long learning curve and may not be universally available [8].
- 4. Hip arthrotomy and dislocation
-
- A last resort; associated with high morbidity, risk of AVN, and compromised hip stability.
Highlights of our approach
- Manual reaming minimized the risk of cartilage damage
- Continuous fluoroscopy enabled dynamic monitoring of the wire’s location
- Use of an arthroscopic grasper allowed minimal disruption and avoided open surgical dislocation
- There was no need to change the patient position or re-drape
- Any orthopedic surgeon can perform this technique as there is no learning curve involved.
Preventive strategies
- Use single-use or high-quality guidewires – avoid reuse
- Ensure correct wire–drill matching to reduce friction
- Limit wire insertion depth and avoid overdrilling
- Use pulsed drilling with saline irrigation to reduce thermal damage [9]
- Avoid multiple redirections through dense cortical bone [10]
- Consider pre-operative computed tomography/MRI to identify areas of sclerosis
- Employ gentle manual reaming when approaching the articular surface.
Guidewire breakage, though rare, can result in significant intraoperative challenges. Our case demonstrates that careful planning, gentle technique, and use of appropriate retrieval tools like arthroscopic graspers can prevent extensive surgical morbidity. A systematic approach to prevention and retrieval can significantly reduce complications and improve patient outcomes.
Early identification of risk factors for hardware failure and cautious, minimally invasive retrieval can prevent serious complications. Liberal use of fluoroscopy enables real-time monitoring and reduces the risk of fragment migration. Every orthopedic unit should maintain a standardized bailout protocol to manage such intraoperative events effectively.
References
- 1. Haberal B, Beyaz S, Effects of orthopedic instruments breakage during surgery: A minimum five-year follow-up. Ann Clin Anal Med 2021;12:443-6. [Google Scholar] [PubMed]
- 2. Arlet J, Ficat C. Ischemic necrosis of the femoral head. Treatment by core decompression. J Bone Joint Surg Am 1990;72:151-2. [Google Scholar] [PubMed]
- 3. Mont MA, Jones LC, Hungerford DS. Nontraumatic osteonecrosis of the femoral head: Ten years later. J Bone Joint Surg Am 2006;88:1117-32. [Google Scholar] [PubMed]
- 4. Zhu QH, Ye TW, Guo YF, Wang CL, Chen AM. Removal of a broken guide wire entrapped in a fractured femoral neck. Chin J Traumatol 2013;16:237-9. [Google Scholar] [PubMed]
- 5. Mehrotra D, Agarwal G, Asthana V. A novel technique to remove a broken guide wire during orthopaedic surgery: A case report. Cases J 2009;2:9252. [Google Scholar] [PubMed]
- 6. Egol KA, Koval KJ, Zuckerman JD. Handbook of Fractures. 5th ed. Philadelphia, PA: Wolters Kluwer; 2015. [Google Scholar] [PubMed]
- 7. Garabadi M, O’Brien S. Broken guidewire retrieval from the hip joint: A case report. Trauma Case Rep. 2021 Jul 21;35:100512. doi: 10.1016/j.tcr.2021.100512. Erratum in: Trauma Case Rep. 2023 Mar 01;45:100813. doi: 10.1016/j.tcr.2023.100813. PMID: 34377759; PMCID: PMC8329481. [Google Scholar] [PubMed] [CrossRef]
- 8. Chen YJ, Huang TW, Huang KC. Retrieval of a broken guidewire from the hip joint using an arthroscope: A case report. Kaohsiung J Med Sci 2008;24:550-4. [Google Scholar] [PubMed]
- 9. Hofmann AA, Wyatt RW, Daniels AU, Alazraki NP. Thermal effects of drilling during internal fixation. J Bone Joint Surg Am 1990;72:13-5. [Google Scholar] [PubMed]
- 10. Prasad, Pidikiti. Guidewire damage during connulated screw fixation for slipped capital femoral epiphysis. Journal of Pediatric Orthopaedics B 13(5):p 346, September 2004. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study June 1, 2026 Kienbock’s Disease in a Young Female without Classical Risk Factors: A Case Report with 1-year Functional Outcome Following Proximal Row Carpectomy
June 1, 2026 Kienbock’s Disease in a Young Female without Classical Risk Factors: A Case Report with 1-year Functional Outcome Following Proximal Row Carpectomy June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction
June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes
May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes