
Understand the long-term biocompatibility of TENs implants, the challenges of delayed removal due to tissue integration, and the importance of specialized tools and regular follow-up for safe and effective implant management.
Dr. Manmohan Singh, Department of Orthopaedic Surgery, Guru Gobind Singh Medical College, Faridkot, Punjab, India. E-mail: doctormanmohan@yahoo.com
Abstract
Introduction: Elastic stable intramedullary nailing is a commonly used modality for the surgical stabilization of long-bone fractures in children, with routine implant removal recommended within 6–12 months. Delayed removal beyond this timeframe is uncommon and presents unique surgical challenges. We report a rare case of titanium elastic nails (TENs) removal performed 7 years after initial fixation, highlighting the technical considerations and successful outcome.
Case Report: A 14-year-old female presented with discomfort in the left thigh. The patient had a history of TENs nails inserted at age 7 for a mid-shaft femoral fracture. The patient was lost to follow-up due to family circumstances. The patient had remained completely asymptomatic throughout the retention period with full functional recovery. Radiograph of the left thigh showed two TENs nails. Due to anticipated extraction difficulty from prolonged retention, a screw retriever technique was successfully employed for safe nail removal without complications.
Conclusion: This case demonstrates the excellent biocompatibility of titanium implants and confirms that delayed TENs removal can be safely accomplished using specialized extraction techniques. The use of a screw retriever provides an effective solution for challenging implant removal scenarios while minimizing surgical morbidity.
Keywords: Titanium elastic nailing, delayed implant removal, pediatric femoral fracture, screw retriever technique.
Elastic stable intramedullary nailing (ESIN) is a commonly used modality for the surgical stabilization of long-bone fractures in children. It is widely used for treating unstable fractures of the radius, ulna, femur, and, occasionally, the tibia and the humerus [1]. This technique preserves the periosteum, allowing bone healing within a closed and intact biological environment [2]. Stable elastic intramedullary nailing uses two flexible nails, which are introduced percutaneously either through the lower metaphysis or the subtrochanteric area. The intramedullary nail method has advantages, such as closed application, less soft tissue injury, avoidance of nerve injury, and cosmetic benefits [3]. Titanium elastic nails (TENs) nail do not disturb the healing of the fracture. It is stable and adaptable as an internal splint, allowing for compression and micromotion at the fracture site, the ideal location for callus formation [4]. The indications for surgical stabilization of pediatric diaphyseal femur fractures are expanding, now including cases such as children with multiple system injuries or associated head injuries. Additional indications include pathological fractures or situations where spica cast application is not feasible. A routine implant removal is recommended within 6–12 months. However, clinical scenarios occasionally arise where removal is significantly delayed due to patient factors, lost follow-up, or family circumstances. Extended retention periods may present technical challenges during extraction due to bone overgrowth, tissue integration, or implant fixation. TENs is a safe and effective method for the treatment of pediatric femoral shaft fractures, because it is minimally invasive, relatively easy to use, and shows very good functional and cosmetic results [5]. Removal of TENs after ESIN is a safe procedure with a low complication rate. It also reduces the hospital stay and helps in the early mobilization of children [6]. We present a unique case of successful TENs removal performed 7 years after initial implantation, utilizing a specialized screw retriever technique to overcome extraction difficulties.
A 14-year-old female presented with discomfort in the left thigh. The patient had a history of TENs nails inserted at age 7 for a mid-shaft femoral fracture. The patient was lost to follow-up due to family circumstances. Primary treatment consisted of closed reduction and internal fixation using two 3.5 mm TENs inserted through a retrograde approach through the distal femoral metaphysis.

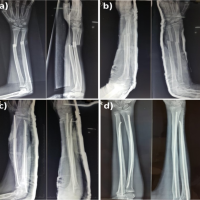
Figure 1: Pre-operative radiograph of patient reveals two intramedullary Titanium elastic nails.
The initial post-operative course was uneventful with complete fracture healing. Plans for routine implant removal at 1 year were delayed due to family circumstances and subsequent loss to follow-up. Throughout the 7-year retention period, the patient remained completely asymptomatic with full return to activities, including competitive sports. (Fig. 1).
Physical examination
Clinical assessment revealed equal limb lengths with a full range of motion at the hip and knee joints. There was no evidence of skin irritation, implant prominence, or functional limitation. The patient demonstrated normal gait pattern and muscle strength.
Radiological assessment
Pre-operative radiographs demonstrated complete fracture healing with appropriate bone remodeling. Both TENs remained in optimal position without evidence of migration into the medullary canal, loosening, or structural failure. Bone quality appeared normal with no signs of stress shielding or cortical changes around the implants.
Surgical technique
Surgery was performed under spinal anesthesia using the original lateral and medial approach. Standard surgical exposure of the nail entry points revealed significant bone overgrowth around the nail ends. Initial attempts at extraction using conventional nail extraction techniques proved challenging due to tight implant integration. A specialized screw retriever (Fig. 2), a threaded instrument typically used for the removal of broken or damaged screws – was employed over the distal ends of the TENs nails. After achieving adequate compression with the ratchet lock, controlled axial traction with gentle rotation successfully removed both nails without cortical damage or the need for extensive bone removal (Fig. 3).

Figure 2: Intraoperative trolley image demonstrating the instrument used for titanium elastic nails removal (screw retriever marked with a yellow arrow).

Figure 3: Titanium elastic nails which got removed by the screw retriever technique.
Intraoperatively, notable bone overgrowth and tight nail integration were observed, which can contribute to local irritation of the surrounding soft tissues and periosteum – factors known to cause thigh pain following implant removal. However, microdamage or stress reactions in cortical bone near the implant, which might not be apparent during surgery, but contribute to pain. While using this technique, we did not encounter any complications. Post-operative radiograph of the left thigh shows successful removal of TENs nails (Fig. 4).

Figure 4: Post-operative radiograph of the after successful removal of the titanium elastic nails.
Post-operative course
The patient experienced an uncomplicated recovery with immediate post-operative mobilization. Pain was minimal and well-controlled with standard analgesics. Wound healing was satisfactory, and the patient returned to full activities within 2 weeks. Follow-up at 2 months demonstrated no complications with maintained limb function.
This case represents one of the longest documented TENs retention periods in the pediatric literature, providing valuable insights into delayed implant removal challenges and solutions. The 7-year retention period without adverse effects supports the excellent biocompatibility profile of titanium implants in pediatric applications. Limited data exist about complications of TENs for femur fracture management in pediatric patients [7]. Extraction of the TENs nail can present certain difficulties and may result in a complex surgical procedure. Multiple factors may contribute to challenges during the removal of an elastic stable intramedullary nail. These include a short nail tip, the nail tip positioned very close to the bone surface. There are reports describing complications of ESIN removal in a healed fracture in the form of unsuccessful nail removal [8]. Various techniques for removing the elastic intramedullary nail have been outlined in the literature. These methods involve using a bone chisel around the tip of the nail [9]. Lascombes has described the use of the chisel followed by pliers [9] and the use of a hollow reamer [10].
Biocompatibility and long-term tolerance
The absence of complications throughout the extended retention period confirms the superior tissue tolerance of TENs. No evidence of local inflammatory reaction, implant degradation, or systemic effects was observed, supporting existing literature on titanium biocompatibility. TENs are a safe and effective choice for operative fixation of length-unstable femoral shaft fractures in children [11].
Technical challenges of delayed removal
Prolonged implant retention often results in bone overgrowth and tissue integration around implant surfaces, significantly increasing extraction difficulty. Standard nail extraction techniques may prove inadequate in such scenarios, necessitating alternative approaches. The use of a screw retriever provided an effective solution by establishing a secure mechanical purchase, enabling controlled extraction without excessive force or bone destruction.
Screw retriever technique
This specialized instrument (Fig. 2), traditionally employed for broken screw extraction, proved highly effective for challenging TENs nail removal. The threaded design of the jaws allows for reliable engagement with the TENs nail implant (Fig. 5), while the ratchet lock/self-centered mechanism structure facilitates controlled traction (Fig. 6). This technique minimizes surgical trauma and reduces operative time compared to alternative methods requiring extensive bone removal. Removal of TENs after ESIN is a safe procedure with a low complication rate [12].

Figure 5: Photos below showing the serrated Jaws (yellow arrow).

Figure 6: Photo below showing the screw retriever and yellow arrow pointing the ratchet lock/self centered mechanism.
Clinical implications
While routine early removal remains the standard of care, this case provides reassurance that delayed removal can be safely accomplished when proper surgical planning and specialized instrumentation are employed. The successful outcome should not discourage timely implant removal but rather inform surgical decision-making in cases where delayed removal becomes necessary. TENs is an effective, easy, fast treatment method and has minimal complications for the treatment of femoral shaft fractures in childhood. Most complications can be reduced by performing basic principles and technical directions [13].
Literature comparison
Most published series report TENs removal within 24 months, with limited data on procedures performed beyond this timeframe. This case contributes to the sparse literature on extended retention periods and demonstrates that delayed removal does not preclude successful outcomes when appropriate techniques are utilized.
Limitations of the study
This report describes a single case, which limits the generalizability of the findings to other patients or clinical scenarios. The absence of a control group restricts the ability to evaluate the relative efficacy of the screw retriever method. The unique nature of a 7-year delayed removal also limits extrapolation to standard cases where TENs nails are removed within the recommended 6–12 months. Larger case series or comparative studies would be valuable to further validate the technique and its applicability.
Delayed TENs removal after 7 years is technically feasible and can be safely accomplished using specialized extraction techniques, such as screw retrievers. This case demonstrates the excellent long-term biocompatibility of TENs while highlighting the importance of surgical preparedness for challenging implant removal scenarios. This method is simple to perform, cost-effective due to the reusability of the screw retriever, and does not require any additional equipment. The procedure is not time-consuming and has been shown to be easily adopted by surgeons across different levels of experience.
In cases of delayed removal of titanium elastic nails (TENS) in pediatric femoral fractures, surgeons should expect difficulties due to bone overgrowth and tissue integration around the implant. Using specialized tools like screw retrievers allows for safe and minimally invasive extraction of well-integrated nails without extensive bone removal, minimizing surgical trauma and complications. This method is easy to use, is inexpensive as the screw retriever is reusable after proper sterilisation , and does not require new or additional equipment. The described technique is simple, cost-effective, and can be performed by any surgeon in any setting.
References
- 1. Gautam VK, Ranade AS, Mone M, Oka GA. A novel technique for the removal of elastic intramedullary nail in pediatric long bones: A technical note. Cureus 2020;12:e9717. [Google Scholar] [PubMed]
- 2. Sinikumpu JJ, Serlo W. The shaft fractures of the radius and ulna in children: Current concepts. J Pediatr Orthop B 2015;24:200-6. [Google Scholar] [PubMed]
- 3. Huang YC, Renn JH, Tarng YW. The titanium elastic nail serves as an alternative treatment for adult proximal radial shaft fractures: A cohort study. J Orthop Surg Res 2018;13:10. [Google Scholar] [PubMed]
- 4. Flinck M, Riad J. Recovery of gait in children and adolescents after pediatric femoral shaft fracture treated with intramedullary nail fixation: A longitudinal prospective study. J Pediatr Orthop 2024;44:1-6. [Google Scholar] [PubMed]
- 5. Bhuyan BK, Mohan Singh S. Titanium elastic nailing in pediatric femoral diaphyseal fractures in the age group of 5-16 years – A short term study. J Clin Orthop Trauma 2014;5:203-10. [Google Scholar] [PubMed]
- 6. Kawalkar A, Badole CM. Percutaneous titanium elastic nail for femoral shaft fracture in patient between 5 and 15 years. J Orthop 2018;15:695-700. [Google Scholar] [PubMed]
- 7. Luhmann SJ, Schootman M, Schoenecker PL, Dobbs MB, Gordon JE. Complications of titanium elastic nails for pediatric femoral shaft fractures. J Pediatr Orthop 2003;23:443-7. [Google Scholar] [PubMed]
- 8. Sun XS, Wang B, Wang F, Tang K, Zhang ZQ, Lin G, et al. Complications of 2 133 cases of pediatric long bone fracture undergoing elastic stable intramedullary nailing in a single medical center. Zhonghua Wai Ke Za Zhi 2018;56:670-6. [Google Scholar] [PubMed]
- 9. Lascombes P. Hardware removal. In: Flexible Intramedullary Nailing in Children: The Nancy University Manual. Berlin/Heidelberg: Springer-Verlag; 2010. p. 53-7. [Google Scholar] [PubMed]
- 10. McDonnell SM, Alsousou J, Handley RC. A simple technique for easy removal of titanium elastic nails. Ann R Coll Surg Engl 2009;91:86. [Google Scholar] [PubMed]
- 11. Siddiqui AA, Abousamra O, Compton E, Meisel E, Illingworth KD. Titanium elastic nails are a safe and effective treatment for length unstable pediatric femur fractures. J Pediatr Orthop 2020;40:e560-5. [Google Scholar] [PubMed]
- 12. Lieber J, Dietzel M, Scherer S, Schäfer JF, Kirschner HJ, Fuchs J. Implant removal associated complications after ESIN osteosynthesis in pediatric fractures. Eur J Trauma Emerg Surg 2022;48:3471-8. [Google Scholar] [PubMed]
- 13. Kayaokay K, Aktuglu K. Titanium elastic nailing in pediatric femoral diaphyseal fractures in the age group of 6-15 years mid-term and long-term outcomes. Pak J Med Sci 2018;34:1529-33. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 10, 2024 Pediatric Forearm Fractures: Investigating the Functional Outcomes of Titanium Elastic Nailing for Unstable Both-Bone Fractures
May 10, 2024 Pediatric Forearm Fractures: Investigating the Functional Outcomes of Titanium Elastic Nailing for Unstable Both-Bone Fractures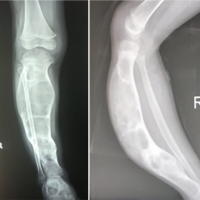 May 10, 2021 Wedge Osteotomy with Tens Nailing in Monostotic Fibrous Dysplasia of Tibia – A Case Report
May 10, 2021 Wedge Osteotomy with Tens Nailing in Monostotic Fibrous Dysplasia of Tibia – A Case Report September 1, 2025 Role of Ortho Biologics in Subtrochanteric Osteotomy Non-union in a Case of Developmental Hip Dysplasia Managed with Total Hip Replacement – A Case Report
September 1, 2025 Role of Ortho Biologics in Subtrochanteric Osteotomy Non-union in a Case of Developmental Hip Dysplasia Managed with Total Hip Replacement – A Case Report February 1, 2025 Transient Synovitis as a Sequela of COVID-19 Infection: A Case Report and Review of Literature
February 1, 2025 Transient Synovitis as a Sequela of COVID-19 Infection: A Case Report and Review of Literature