
Endobutton fixation for Type 2 Neer Lateral end clavicle fracture is a valuable surgical technique, offering a minimally invasive approach with good clinical outcomes.
Dr. Tushar Ranjan Dalei, Department of Orthopaedics, Veer Surendra Sai Institute of Medical Sciences and Research, Burla, Sambalpur, Odisha, India. E-mail: tusharranjan3009@gmail.com
Abstract
Introduction: To evaluate the clinical and radiological outcomes following coracoclavicular (CC) reconstruction with the endobutton for Neer type 2 lateral end clavicle fracture. Clavicular fracture is one of the commonest injuries encountered routinely in orthopedic practice, with an incidence ranging from 44 to 66% of all fractures. Based on the location of fractures, they may be the middle third being most common or the lateral and medial third being least common. Fractures of the lateral end of the clavicle are troublesome to manage given their instability, ligamentous disruptions and with a wide array of treatment options including fixation by means of plates, screws, K-wires, tapes and buttons making the decision often difficult for the surgeon based on the apprehended pros and cons of individual fixation methods.
Materials and Methods: A prospective cohort study on 30 cases of adult Neer type 2 lateral end clavicle fractures was carried out, which were fixed with CC endobutton under fluoroscopic guidance. Postoperatively, patients were given an arm sling pouch for 2 weeks with graded physiotherapy and a range of exercises commencing after 2 weeks. Cases were followed up at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year intervals each. Functional and radiological outcomes were observed and documented.
Results: All 30 patients were assessed with a mean follow-up 12 months. The mean age group under the study was 34.70 years. Most of the patients had a constant shoulder score above 90 with excellent disabilities of the arm, shoulder, and hand scores. Mean fracture union time was 15 weeks without any major complication such as infection, revision surgeries, implant migration and stress fractures.
Discussion and Conclusion: Endobutton technique for fixation of type 2 lateral end clavicle stands as a promising and effective option demonstrating significant improvements in terms of clinico-radiological perspective and patient satisfaction. The current method of treatment exhibits stronger biomechanics with good fixation with almost no implant-related complications. It also supports an early mobilization crucial for maintaining shoulder function and preventing stiffness.
Keywords: Lateral end clavicle fracture, coracoclavicular reconstruction, endobutton, fibertape.
Clavicle fractures are common injuries in adults (2–5%) and children (10–15%) and constitute 44–66% of all shoulder fractures [1,2].
Allman classified clavicle fractures into three types based on anatomical location [3]..The most common type is the middle third fractures (group I) about 80% cases, lateral clavicular fractures constituting group II, approximately 15–25%, and proximal third clavicular fractures (group III), the least about 5% only [4,5,6].
Neer further classified distal clavicle fractures into three groups based on the adhesion location of the coracoclavicular (CC) ligament [7]. Out of which, type 2 is the unstable ones which has many controversies in their management. In Type 2 fractures, the distal clavicle fragment is subjected to the distal pull by the weight of the arm as well as a medial pull by the strong pectoral muscles and latissimus dorsi, while the proximal fragment is dragged posteriorly by the trapezius. These disturbing forces contribute to the fracture displacement and the unstable nature of Type 2 fractures.
Neer’s type II fractures disrupt the integrity of the CC ligament andtherefore, are inherently unstable, requiring an extended period of time to achieve bone union and are associated with a high rate of non- or malunion [8].
For the surgical treatment of unstable Neer type 2 distal clavicle fractures, several techniques have been introduced, such as Steinmann pin (S-pin) or Kirschner wire fixation from acromion to clavicle, anatomic locking plate fixation, hook plate fixation, CC screw fixation, which include rigid fixation [9,10]. Flexible fixation methods include CC sutures, tapes, wires, anchors, or cortical buttons with or without arthroscopic assistance [10,11,12,13].
The endobutton technique is a new and simple technique that has been proposed to overcome the complications of rigid fixation methods [14].The advantages of CC button fixation result in greater strength than the traditional locking plate and lower hardware-related complications [15,16].
Due to the unstable nature of fracture morphology and fixation with the endobutton generates a higher strength with minimal complications. This motivates us to perform a prospective study to evaluate the clinical and radiological outcomes following CC reconstruction with the endobutton for Neer’s type II lateral end clavicle fracture in our institute between 2022 and 2024.
A hospital-based prospective cohort study was undertaken following Institutional Ethical Committee approval bearing IRB no.058-2022/I-S-T/083/DT March 01, 2023, taking around 30 adult patients with acute, unilateral closed Neer’s type 2 distal clavicle fractures. A convenient sampling technique was used. Multiple injuries, open fractures, and age group <18 years were excluded from the study.
All the surgeries were performed either under general anesthesia or inter-scalene block. The surgical technique is a modification of the double endobutton technique described by Steven [17]. The patient was positioned in the supine position with a bolster underneath the interscapular area and a vertical 6-cm bra-strap incision centered over the coracoid and extending upwards to the clavicle was made. Medial and lateral skin flaps were developed, and after the separation of the delto-trapezial fascia, the coracoid was exposed and cleared off all the way to the base. The medial and lateral edges of the coracoid at the base are clearly identified. A vertical tunnel was made in the coracoid in a cephalocaudal direction with a 3.2 mm drill-bit over a guide wire. The drill hole was directly over the base of the coracoid, and the drill was aimed slightly anteriorly. Endobutton with fiberwire loop was passed through this tunnel and manually flipped to hook the endobutton beneath the coracoid. The lateral portion of the clavicle was exposed. The clavicle is manually reduced, and while the reduction is being held with a 2.0 mm K-wire, another drill hole of size 3.2 mm was made in the medial fragment of the clavicle midway between the anterior and posterior border of the clavicle. Another endo-button from the same fiber-wire loop was passed through the clavicular tunnel in an upward direction and flipped to rest over the superior surface of the clavicle. The achieved reduction was secured after tying the knot of the fiber-wire over the clavicle endobutton. Intra-operative reduction was confirmed fluoroscopically before wound closure. An arm pouch sling was used for support of the clavicle in the immediate post-operative period till the suture removal at 2 weeks. Pendulum exercise was started 2 weeks after surgery when pain had subsided. Arc of pendulum swing was gradually increased to 90° up to 4 weeks after surgery, after which abduction of the shoulder was allowed and active range of shoulder motion was started to achieve normal shoulder motion within 3 months. Patients were followed up in the outpatient department at 2nd week (stitch removal), 6 weeks, 3rd month, 6th month, 1 year. In each visit, a radiograph with an anteroposterior view of the shoulder joint was taken to evaluate fracture union. Functional outcomes were assessed based on Constant–Murley [18,19] and disabilities of the arm, shoulder, and hand (DASH) score [20].
Statistical analysis
Data were collected and graphics were designed using Microsoft Office Excel 2019. The data were analyzed with Statistical Package for the Social Sciences (IBM, Armonk, NY, USA) version 23.0 for Windows. The categorical and continuous variables are represented as frequency (percentage) and mean ± standard deviation respectively.
All 30 patients were (23 males and 7 females, most of them were aged below 40 years) studied between August 2022 and July 2024. All patients had a mean of approximately 12 months of follow-up. Demographic characteristics of the patients are reported in Table 1. The mean age of the patient was 34.70 ± 8.13 years (range 16–54). The highest proportion of cases was seen in 31–35 years of age group.

Table 1 : Demographic characteristics of the patients
Mean functional outcomes scores are analyzed by the Constant–Murley score and DASH score. Constant score, those are lying between 86 and 100 points designated as “very good”, 71 and 85 points – “good,” 56–70 points – “fair,” and whereas <56 points were “poor.” Similarly, DASH score with a minimal detectable change (MCD) of more than 10% is taken to be significant. MCD is the smallest amount of change that has to occur before the change can be considered a true change and not error [20]. Outcome scores are reported in Table 2 and Fig. 1 and 2.
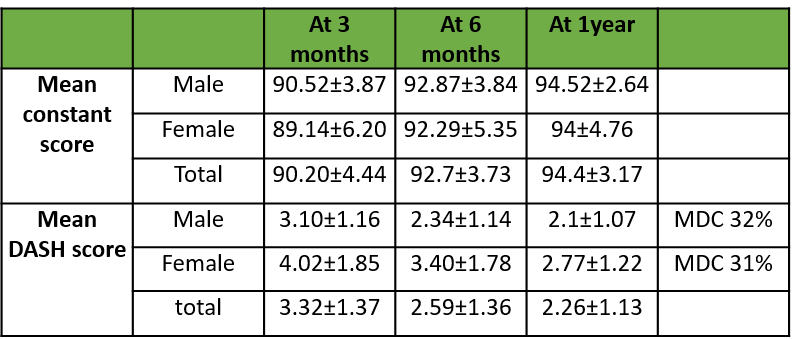
Table 2: Mean scoring system
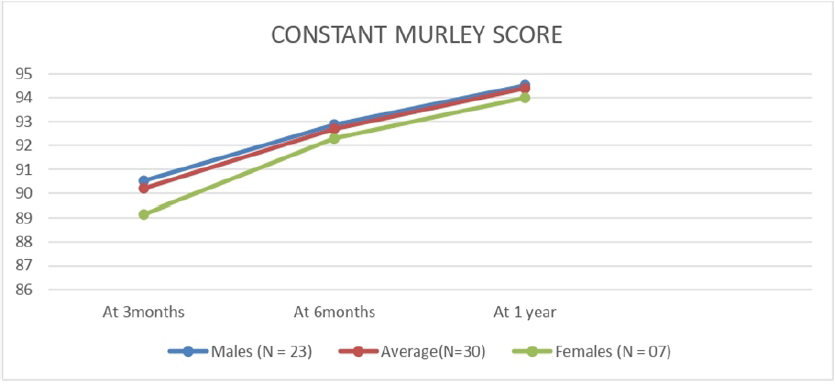
Figure 1: Graphical presentation of constant Murley score.
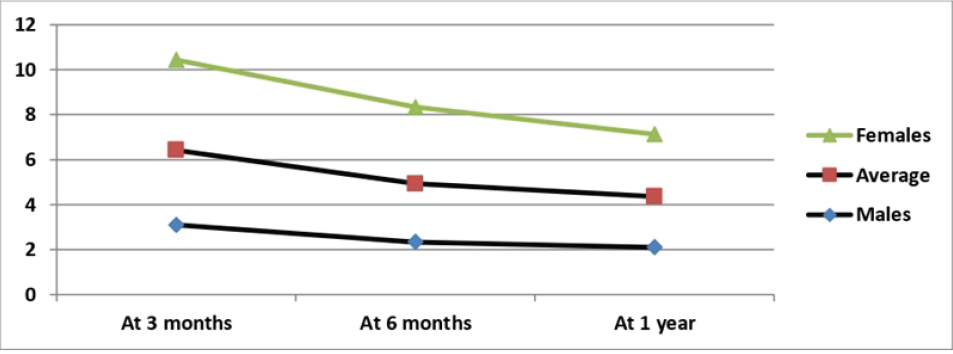
Figure 2: Graphical presentation of mean disabilities of the arm, shoulder, and hand score.
All patients were satisfied with the results and had excellent results at final follow-up. Most of the patients had a constant shoulder score above 90 with an excellent grade, except for two patients. Of these, one of had a superficial surgical site infection which resolved with local wound care. Another patient was an old lady who developed shoulder stiffness due to improper physiotherapy following surgical fixation. Three patients post-surgery developed parasthesia around the surgical site, which improved in due course of time.
All patients had fracture union in a mean of 15 weeks (Figs. 3a, b, c).

Figure 3: (a) X-ray showing Neers type 2 lateral end clavicle fracture. (b) X-ray showing 2 month post endobutton fixation. (c) X-ray showing 6-month post endobutton fixation.
There were no hardware-related complications such as implant migration, stress fracture detected on final follow-up radiographs. No patients complained of hardware irritation or prominence. There were no cases of reoperation or revision.
It is quite difficult to achieve stable fixation and early mobilization with previously proposed treatment methods in cases of fractures of the lateral third of the clavicle, where the distal fragment is small and deforming forces are great [21]. No consensus has been established regarding the optimal operative treatment for these fractures [22]. According to the literature, the incidence of failure of conservative treatment of clavicle fractures ranges from 4.4% to 31% in terms of pain, loss of force, rapid fatigue, paresthesia, pain when lying on the affected shoulder, and esthetic defects [23,24,25]. De Giorgi et al., in their case series observed these symptoms in 21 patients (29.6%) out of 71 cases studied [26]. Similarly, Robinson and Cairns in their cohort study of 127 patients of displaced lateral end clavicle fractures, 7 patients underwent immediate surgical fixation and 14 patients underwent delayed surgery due to severe symptoms and of the remaining 87 patients who were managed conservatively 21 of them (21% of the whole cohort) had a nonunion of the clavicular fracture [27].
Various methods of surgical treatment are available at present such as K-wire fixation, tension band wiring (TBW), screw fixation, locking and non-locking plates and flexible fixation methods such as CC stabilisation using non-absorbable sutures or endobutton and fibertape fixation. Patients managed by TBW complications like K-wire migration, loss of reduction, superficial infection, asymptomatic non-union, and wire breakage were observed, and all patients needed implant removal [28].
Patients managed with precontoured locking plates have complications like fracture at the medial end of the plate, deep and superficial infection which leads to symptomatic non-union, hardware symptoms requiring repeat surgery for plate removal have been noticed [29,30,31]. In patients managed with hook-plate fixation, although shoulder functions range from good to excellent, they are associated with major complications such as dislocation of hook, fracture of the medial end of the clavicle, symptomatic non-union, severe acromioclavicular (AC) joint arthrosis, rotator cuff tear, acromion fracture, acromial osteolysis, hypertrophic scar and frozen shoulder. Furthermore most of the patients have to remove their plates by a second surgery [32,33,34].
In patients managed with a CC screw, all patients require screw removal. Complications such as superficial infection, screw back out, and implant failure are also noticed [35,36]. In studies with flexible CC fixation nearly all patients have excellent results. Few minor complications are observed in the form of frozen shoulder, asymptomatic non-union, minor infections, titanium wire breakage, and uncomfortable subcutaneous tenting of the Mersilene tape [37,38,39].
In our study, we prospectively evaluate the clinical and radiological outcomes of CC reconstruction using the endobutton system, a technique that may gain popularity due to its minimally invasive nature and promising results. It provides stable fixation of a small-sized lateral fragment, allowing early mobilization and hence secured bony union. Stable fixation and immediate post-operative shoulder motion can be achieved even in osteoporotic bone without impinging the AC joint or sub-acromial space. The clinical outcomes in this study are assessed using standard metrics such as the Constant–Murley score and the DASH score. The results demonstrate significant improvements in shoulder function and patient satisfaction postoperatively. Patients typically report marked improvements in pain relief, range of motion and overall shoulder function within the first 3–6 months post-surgery. The use of the endobutton system allows early mobilization, which is crucial in maintaining shoulder function and preventing stiffness.
The complication rate in this study is relatively low, with no cases of hardware irritation. No major complications that necessitate revision surgery occurred in our study. Some minor complications, like one case with superficial infection which was not associated with any loss of reduction and subsequently led to bony union, one case of transient stiffness of the shoulder treated by physiotherapy, and three cases of paresthesia observed over the shoulder which improved in the due course of time. Importantly, there are no reports of coracoid fracture, a potential complication when using other methods of CC ligament reconstruction [40,41]. There are no cases with malunion or nonunion in our study.
Majority of the fractures in our study have achieved radiological union at an average of 15 ± 2.86 weeks, which is little higher as compared to Panagopoulos A et al. [12] (mean time of 2.7 ± 0.6 months) and Vikas et al. [13] (mean union was 11 ± 2.8 weeks) study.
Stress fracture of the clavicle is insignificant in this technique compared with hook plate fixation because of the lack of a stress riser at its medial end. There are less complications such as fixation failures, iatrogenic rotator cuff injury, AC joint osteoarthritis, and subacromial bursitis.
The procedure is less invasive, leading to reduced soft-tissue damage, quicker recovery time, and potentially less post-operative pain. Biomechanically, the endobutton provides superior strength and stability, which is particularly important in active patients or those with high functional demands. The lower complication rates, especially concerning hardware-related issues, make the endobutton system a safer option for many patients.
High levels of patient satisfaction were reported, likely due to quick return to daily activities and the strong functional outcomes. The results of our study are quite promising and supported well by a few other studies in the literature. The mean constant score at the end of 1 year was found to be 94.4 ± 3.17, which is higher than that of Ahmad et al. [42] (85.9 ± 6.9), probably due to lesser sample size (10 cases of lateral end clavicle fractures). It is also higher than that of Kuner et al. (81.8 ± 8) and Kraus et al. (89%), who also used an arthroscopic endobutton for fixation of lateral clavicle fractures [43,44]. Zheng et al. reported a score of 92.33 ± 4.89 using the double endobutton with open technique [8],Whereas Struhl et al in his study of closed loop double endobottom technique achieved a constant score of 95.6 ± 8.4 [22]. The mean CS was 96.6 ± 3.4 for Panagopoulos A et al. [12].
The DASH score in our study was observed to have a significant change postoperatively from 3 months to 1 year, i.e., 32% and 31% among males and females, respectively. Unlike purely clinical or radiological assessments, the DASH score reflects the patient’s subjective experience, capturing aspects such as pain, weakness, and difficulty in performing specific tasks. Following surgery, there was a marked reduction in DASH scores reflecting the restoration of shoulder function and alleviation of symptoms.
Although the results are promising, the study does have limitations. The sample size, though adequate for initial findings, is relatively small, which may limit the generalizability of the study. Second, although the short to mid-term results are encouraging, the study’s follow-up period may not be long enough to fully capture the long-term durability of the endobutton system and the potential for late-onset complications. A long-term follow-up is necessary to fully assess the durability of the endobutton system and to monitor late complications such as post-traumatic arthritis, coracoid, and clavicular osteolysis [40,41]. The study design is prospective and observational but not randomized, which introduces potential bias. A randomized controlled trial would be ideal to compare the endobutton system directly with other fixation techniques.
The use of the endobutton system for CC reconstruction in Neer’s Type II distal clavicle fractures presents itself as a promising and effective treatment option. This technique has demonstrated significant improvements in clinical outcomes, particularly in terms of pain relief, functional recovery and patient satisfaction. The strong biomechanical properties of the endobutton system ensure that the reduction is well-maintained and the healing process is effectively supported with most fractures achieving union within a satisfactory timeframe. The minimally invasive nature of the procedure further enhances its appeal as it reduces soft-tissue damage, allows for quicker recovery and minimizes the risk of postoperative complications such as hardware irritation or migration. Endobutton supports early mobilization, which is crucial for maintaining shoulder function and preventing long-term stiffness. These factors contribute to the high levels of patient satisfaction observed in our study.
Despite the positive outcomes, it is important to acknowledge the limitations of the study. The relatively small sample size, shorter duration of follow-up and lack of randomization limit the broader applicability of the findings and introduce potential bias.
Moving forward, it is essential that future research involves larger, randomized controlled trials with extended follow-up periods to more comprehensively evaluate the endobutton system’s performance. These studies should also compare the endobutton with other fixation techniques to determine the best practices for treating Neer’s Type II distal clavicle fractures. If these promising early results are validated, the endobutton system could well become the preferred method of treatment, offering patients a reliable, safe, and effective solution for a notoriously difficult fracture type.
Endo button fixation for type 2 lateral end clavicle fracture promises to be a safe, minimally invasive technique with satisfactory clinical outcome in terms of pain relief and shoulder function.
References
- 1. Van Der Meijden OA, Gaskill TR, Millett PJ. Treatment of clavicle fractures: Current concepts review. J Shoulder Elbow Surg 2012;21:423-9. [Google Scholar] [PubMed]
- 2. Toogood P, Horst P, Samagh S, Feeley BT. Clavicle fractures: A review of the literature and update on treatment. Phys Sportsmed 2011;39:142-50. [Google Scholar] [PubMed]
- 3. Allman FL Jr. Fractures and ligamentous injuries of the clavicle and its articulation. J Bone Joint Surg Am 1967;49:774-84. [Google Scholar] [PubMed]
- 4. Nordquit A, Peterson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res 1994;300:127-32. [Google Scholar] [PubMed]
- 5. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80:476-84. [Google Scholar] [PubMed]
- 6. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg 2002;11:452-6. [Google Scholar] [PubMed]
- 7. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res 1968;58:43-50. [Google Scholar] [PubMed]
- 8. Zheng YR, Lu YC, Liu CT. Treatment of unstable distal-third clavicule fractures using minimal invasive closed-loop double endobutton technique. J Orthop Surg Res 2019;14:37. [Google Scholar] [PubMed]
- 9. Asadollahi S, Bucknill A. Hook plate fixation for acute unstable distal clavicle fracture: A systematic review and meta-analysis. J Orthop Trauma 2019;33:417-22. [Google Scholar] [PubMed]
- 10. Stegeman SA, Nacak H, Huvenaars KH, Stijnen T, Krijnen P, Schipper IB. Surgical treatment of Neer type-II fractures of the distal clavicle: A meta-analysis. Acta Orthop 2013;84:184-90. [Google Scholar] [PubMed]
- 11. Yagnik GP, Seiler JR, Vargas LA, Saxena A, Narvel RI, Hassan R. Outcomes of arthroscopic fixation of unstable distal clavicle fractures: A systematic review. Orthop J Sports Med 2021;9(5):1-10. [Google Scholar] [PubMed]
- 12. Panagopoulos A, Tatani I, Kattou C, et al. (May 22, 2022) Clinical and Radiological Outcomes of Closed-Loop, Double Button, Coracoclavicular Fixation for Extralateral (Neer Type IIC) Fractures of the Distal Clavicle. Cureus 14(5): e25228. doi:10.7759/cureus.25228 [Google Scholar] [PubMed] [CrossRef]
- 13. Vikas V, Bhatia N, Jalan D, Prakash J, Singh J, Khare S. Clinical outcome of Neer type II lateral end clavicle fractures with coracoclavicular ligament disruption treated with pre-contoured locking plate and endobutton. Cureus 2021;13:e12585. [Google Scholar] [PubMed]
- 14. Dalei TR, Samal BP, Gupta AK, Senapati R, Sahoo TP. Coraco-clavicular endobutton and fiber tape fixation for Neer’s type II unstable lateral clavicular fracture: A case series with literature review. J Surg Case Rep 2022;2022:rjac120. [Google Scholar] [PubMed]
- 15. Yagnik GP, Brady PC, Zimmerman JP, Jordan CJ, Porter DA. A biomechanical comparison of new techniques for distal clavicular fracture repair versus locked plating. J Shoulder Elbow Surg 2019;28:982-8. [Google Scholar] [PubMed]
- 16. Xu Y, Guo X, Peng H, Dai H, Huang Z, Zhao J. Different internal fixation methods for unstable distal clavicle fractures in adults: A systematic review and network meta-analysis. J Orthop Surg Res 2022;17:43. [Google Scholar] [PubMed]
- 17. Steven S. Double endobutton technique for repair of complete acromioclavicular joint dislocations. Tech Shoulder Elbow Surg 2007;8:175-9. [Google Scholar] [PubMed]
- 18. Conboy VB, Morris RW, Kiss J, Carr AJ. An evaluation of the constant-Murley shoulder assessment. J Bone Joint Surg 1996;78-B:229-32. [Google Scholar] [PubMed]
- 19. Ziegler P, Kühle L, Stöckle U, Wintermeyer E, Stollhof LE, Ihle C, et al. Evaluation of the Constant score: Which is the method to assess the objective strength? BMC Musculoskelet Disord 2019;20:403. [Google Scholar] [PubMed]
- 20. Beaton DE, Davis AM, Hudak P, McConnell S. The dash (disabilities of the arm, shoulder and hand) outcome measure: What do we know about it now? Br J Hand Ther 2001;6:109-18. [Google Scholar] [PubMed]
- 21. Yoo JH, Chang JD, Seo YJ, Shin JH. Stable fixation of distal clavicle fracture with comminuted superior cortex using oblique T-plate and cerclage wiring. Injury 2009;40:455-7. [Google Scholar] [PubMed]
- 22. Struhl S, Wolfson TS. Closed-loop double endobutton technique for repair of unstable distal clavicle fractures. Orthop J Sports Med 2016;4:2325967116657810.1-7 [Google Scholar] [PubMed]
- 23. Nowak J, Holgersson M, Larsson S. Sequelae from clavicular fractures are common: A prospective study of 222 patients. Acta Orthop 2005;76:496-502. [Google Scholar] [PubMed]
- 24. Inman VT, Saunders JB. Observations on the function of the clavicle. Calif Med 1946;65:158-66. [Google Scholar] [PubMed]
- 25. Lazarides S, Zafiropoulos G. Conservative treatment of fractures at the middle third of the clavicle: The relevance of shortening and clinical outcome. J Shoulder Elbow Surg 2006;15:191-4. [Google Scholar] [PubMed]
- 26. De Giorgi S, Notarnicola A, Tafuri S, Solarino G, Moretti L, Moretti B. Conservative treatment of fractures of the clavicle. BMC Res Notes 2011;4:333. [Google Scholar] [PubMed]
- 27. Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg 2004;86:778-82. [Google Scholar] [PubMed]
- 28. Lee YS, Lau MJ, Tseng YC, Chen WC, Kao HY, Wei JD. Comparison of the efficacy of hook plate versus tension band wire in the treatment of unstable fractures of the distal clavicle. Int Orthop 2009;33:1401-5. [Google Scholar] [PubMed]
- 29. Lee SK, Lee JW, Song DG, Choy WS. Precontoured locking plate fixation for displaced lateral clavicle fractures. Orthopedics 2013;36:801-7. [Google Scholar] [PubMed]
- 30. Anderson JR, Willis MP, Nelson R, Mighell MA. Precontoured superior locked plating of distal clavicle fractures: A new strategy. Clin Orthop Relat Res 2011;469:3344-50. [Google Scholar] [PubMed]
- 31. Tiren D, Vroemen JP. Superior clavicle plate with lateral extension for displaced lateral clavicle fractures: A prospective study. J Orthop Traumatol 2013;14:115-20. [Google Scholar] [PubMed]
- 32. Tiren D, Van Bemmel AJ, Swank DJ, Van Der Linden FM. Hook plate fixation of acute displaced lateral clavicle fractures: Mid-term results and a brief literature overview. J Orthop Surg Res 2012;7:2. [Google Scholar] [PubMed]
- 33. Haidar SG, Krishnan KM, Deshmukh SC. Hook plate fixation for type II fractures of the lateral end of the clavicle. J Shoulder Elbow Surg 2006;15:419-23. [Google Scholar] [PubMed]
- 34. Flinkkila T, Ristiniemi J, Lakovaara M, Hyvonen P, Leppilahti J. Hook-plate fixation of unstable lateral clavicle fractures: A report on 63 patients. Acta Orthop 2006;77:644-9. [Google Scholar] [PubMed]
- 35. Macheras G, Kateros KT, Savvidou OD, Sofianos J, Fawzy EA, Papagelopoulos PJ. Coracoclavicular screw fixation for unstable distal clavicle fractures. Orthopaedics 2005;28:693-6. [Google Scholar] [PubMed]
- 36. Esenyel CZ, Ceylan HH, Ayanoglu S, Kebudi A, Adanir O, Bülbül M. Treatment of Neer type 2 fractures of the distal clavicle with coracoclavicular screw. Acta Orthop Traumatol Turc 2011;45:291-6. [Google Scholar] [PubMed]
- 37. Yang SW, Lin LC, Chang SJ, Kuo SM, Hwang LC. Treatment of acute unstable distal clavicle fractures with single coracoclavicular suture fixation. Orthopedics 2011;34:e172-7. [Google Scholar] [PubMed]
- 38. Soliman O, Koptan W, Zarad A. Under-coracoid-around-clavicle (UCAC) loop in type II distal clavicle fractures. Bone Joint J 2013;95-B:983-7. [Google Scholar] [PubMed]
- 39. Li Y, Shi S, Ou-Yang YP, Liu TL. Minimally invasive treatment for Neer IIb distal clavicle fractures with titanium cable. J Trauma 2011;71:E37-40. [Google Scholar] [PubMed]
- 40. Sambandam B, Gupta R, Kumar S, Maini L. Fracture of distal end clavicle: A review. J Clin Orthop Trauma 2014;5:65-73. [Google Scholar] [PubMed]
- 41. Hou Z, Graham J, Zhang Y, Strohecker K, Feldmann D, Bowen TR, et al. Comparison of single and two-tunnel techniques during open treatment of acromioclavicular joint disruption. BMC Surg 2014;14:53. [Google Scholar] [PubMed]
- 42. Ahmad S, Sinha S, Narang A, Kalra M, Arshad A. Open double endobutton loop fixation, a one-stop solution for both; Lateral end clavicle fractures and acromioclavicular joint dislocations. Int J Orthop Res 2022;4:89-94. [Google Scholar] [PubMed]
- 43. Kuner E, Beeres FJ, Babst R, Schoeniger R. Which lateral clavicle fractures can be treated by an arthroscopic-assisted endobutton procedure? An analysis of risk factors. Arch Orthop Trauma Surg 2019;139:331-7. [Google Scholar] [PubMed]
- 44. Kraus N, Stein V, Gerhardt C, Scheibel M. Arthroscopically assisted stabilization of displaced lateral clavicle fractures with coracoclavicular instability. Arch Orthop Trauma Surg 2015;135:1283-90. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Pull Out Suture Technique for Fixing Coronoid Fractures using a Single Lateral Extensor Digitorum Communis Split Approach and Fiberwire Endobutton Fixation by Retrograde Drilling – A Case Series
March 1, 2026 Pull Out Suture Technique for Fixing Coronoid Fractures using a Single Lateral Extensor Digitorum Communis Split Approach and Fiberwire Endobutton Fixation by Retrograde Drilling – A Case Series October 1, 2025 Evaluation of Combined Use of Pre-contoured Locking Distal Clavicle Plate and Tunneled Suspensory Device Fixation for Unstable Lateral End Clavicle Fracture
October 1, 2025 Evaluation of Combined Use of Pre-contoured Locking Distal Clavicle Plate and Tunneled Suspensory Device Fixation for Unstable Lateral End Clavicle Fracture October 10, 2015 Predatory Journals: What are they?
October 10, 2015 Predatory Journals: What are they? March 10, 2022 Onchycobacter anthropi Pyomyositis in Immunocompetent Patient: Case Report
March 10, 2022 Onchycobacter anthropi Pyomyositis in Immunocompetent Patient: Case Report