
Good outcomes can be obtained with bilateral arthroplasty through the direct anterior approach in cases of bilateral neck or femur fractures, in a single sitting, which can facilitate early mobilization and reduce hospital stay.
Dr. Aashiket Sable, Department of Orthopaedics, Wockhardt Hospital, Mumbai, Maharashtra, India. E-mail: aashiketsable67@gmail.com
Abstract
Introduction: Bilateral intracapsular neck of femur fractures are rare and are usually associated with underlying metabolic bone diseases such as osteomalacia or osteoporosis. Direct anterior approach (DAA) total hip arthroplasty (THA) is considered the treatment of choice for displaced intracapsular fractures of the femoral neck in both elderly and selected young patients with poor bone quality. Performing THA on both sides in a single sitting can facilitate early mobilization and reduce hospital stay.
Case Report: We report a case of a 40-year-old male who presented with bilateral displaced intracapsular neck of femur fractures following a fall from bed at home. The patient underwent bilateral THA through the DAA in a single sitting. The post-operative course was uneventful. Full weight-bearing mobilization with walker support was started on the 1st post-operative day. By 3–4 weeks post-surgery, the patient had resumed independent activities of daily living.
Conclusion: Simultaneous bilateral DAA-THA can provide excellent clinical and functional outcomes in carefully selected patients with bilateral neck of femur fractures of metabolic origin. Performing arthroplasty on both sides in a single sitting enables early rehabilitation and better functional recovery.
Keywords: Bilateral neck of femur fracture, direct anterior approach, total hip arthroplasty, metabolic bone disease.
Simultaneous bilateral femoral neck fractures are exceedingly rare, especially following low-energy trauma. Typically associated with metabolic bone disorders such as osteomalacia or renal osteodystrophy, bilateral fractures may also result from seizures, electrical injuries, or high-energy impacts [1]. While unilateral femoral neck fractures are common in young patients after high-energy trauma and in the elderly after low-energy trauma, bilateral fractures following trivial injuries, such as a fall at home, are exceptionally rare [1]. With this report, we present a case of a 40-year-old male who sustained simultaneous bilateral intracapsular femoral neck fractures after a trivial fall at home, treated with single-stage bilateral total hip arthroplasty (THA) using the direct anterior approach (DAA).
A 40-year-old male presented to our emergency department with an acute onset of pain in both his hips with inability to walk, after a fall from his bed, sustained at home the same day. On examination, the patient has bilateral hip joint tenderness and an inability to perform the straight leg test, with no distal neuromuscular deficit observed in both lower extremities. The patient did not have any other comorbidities. Plain radiographs revealed bilateral displaced intracapsular fractures of the femoral neck (Fig. 1).

Figure 1: Pre-operative anteroposterior pelvis X-ray showing bilateral displaced intracapsular fractures of the femoral neck.
Routine blood investigations were within normal limits with reduced serum calcium (6.43 mg/dL), phosphorus (1.51 mg/dL), and Vitamin D3 (<3 mg/dL) levels and raised serum PTH levels (580.3 pg/mL). The metabolic panel showed poor bone quality, raising suspicion of an underlying metabolic disorder.
The symptoms warranted urgent surgical intervention due to young age, poor bone stock, a trivial trauma mechanism, and bilateral displaced fractures. Bilateral arthroplasty was favored over osteosynthesis for similar reasons. After physician clearance for surgery, and adequate deep vein thrombosis and antibiotic prophylaxis, the plan of action was to proceed with bilateral THA with DAA, to reduce muscle trauma associated with the posterior approach and allow early mobilization. The patient was positioned supine on a fracture traction table. The left hip was operated on first through DAA, starting the incision two finger breadths lateral to the anterior superior iliac spine and extending into the proximal femur (Fig. 2).
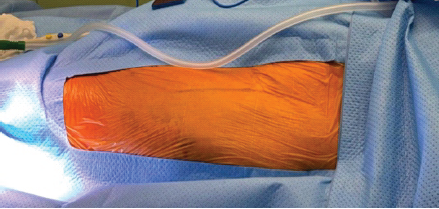
Figure 2: Incision landmark – 2 finger breadths lateral to the anterior superior iliac spine, extending to the proximal femur.
The tensor fascia lata (TFL) muscle fibers were split, avoiding any form of muscle trauma, especially to the short external rotators – as encountered in the traditional posterior approach (Fig. 3).
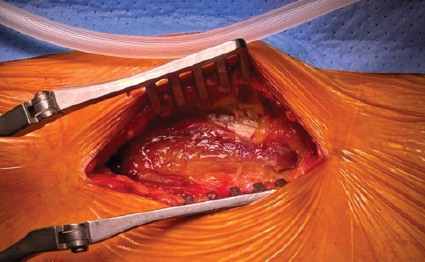
Figure 3: The tensor fascia lata (TFL) muscle fibers are separated after lifting the TFL fascia.
The lateral circumflex femoral vessels were spared, and the head was removed en masse, cauterizing the foveal ligament (Figs. 4 and 5).
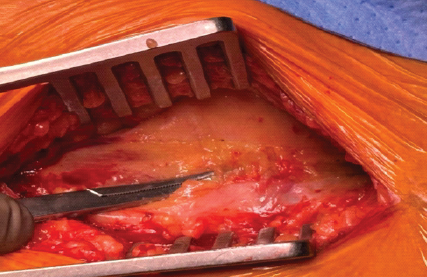
Figure 4: Lateral circumflex femoral vessels spared.
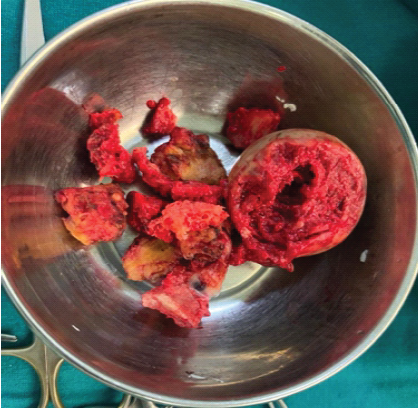
Figure 5: Head removed en masse.
An uncemented distally loading long femoral stem with an uncemented acetabular cup was inserted and firmly fixed. The right hip was operated on subsequently with similar implants, just that the acetabular cup on the right side was fixed with two screws. Post-operative radiograph showed acceptable implant positioning (Fig. 6).
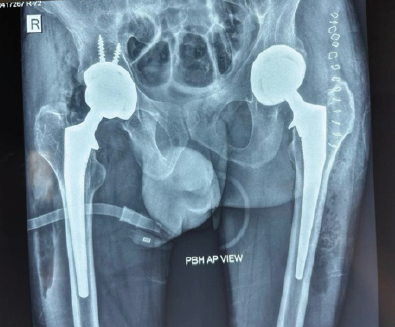
Figure 6: Post-operative radiograph.
The post-operative course was uneventful. Hip and knee range of motion exercises were started from the day of surgery, along with protected weight bearing with a walker from post-operative day 1. The patient was discharged on the 7th post-operative day and was advised walker-assisted protected weight-bearing walking for 7 weeks, after which he started walking full-weight bearing with comfort using a tripod stick initially for the first few weeks. Staircase climbing was started in 2 weeks. By the end of 2 months, the patient walked comfortably without any support and started performing his activities of daily living independently. At 4 months follow-up (Fig. 7), the Harris Hip Score was calculated to be 86, which was considered to be excellent, 100 being the highest score [2].
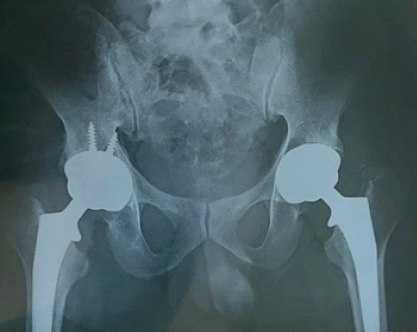
Figure 7: Four-month follow-up.
Femoral neck fractures in young patients are usually a result of high-impact traumatic events, and these fractures are typically unilateral – except in the case of pre-existing medical conditions such as osteoporosis, renal osteodystrophy, or hypocalcemic convulsions with epileptic attacks – wherein bilateral involvement may be seen after low-energy trauma [1]. In this case report, we show a similar case of a 40-year-old male with deranged blood parameters, pointing toward a metabolic bone disorder, who sustained bilateral femoral neck fractures following a trivial fall at home. Blomfeldt et al., in 2011, performed a large randomized controlled trial and compared the results of primary internal fixation and THA following femoral neck fractures – the authors noted that primary THA provides better outcomes over internal fixation in displaced femoral neck fractures [3]. Ben and Gordon compared the results of THA and bipolar hemiarthroplasty, and still found THA to have superior outcomes [4]. Furthermore, bilateral THA done in a single sitting, and not staged, in patients who are fit for surgery, yields better functional outcomes with an opportunity to offer early out-of-bed mobilization to the patient [5], since our patient was a 40-year-old male with no major comorbidities and was fit for surgery, who decided to proceed with bilateral THA in the same sitting. The DAA to the hip is unique, with its internervous and intermuscular plane between the sartorius and TFL, the advantages being shorter hospital stay [6], earlier functional recovery [7], and lower dislocation risks [8]. Some disadvantages are also associated with it, such as risk of injury to the lateral femoral cutaneous nerve [9], periprosthetic fractures [10], and a long learning curve [11,12]. In a review article by Ming Ang et al. in 2023, the DAA was proven to be a better approach as compared to the posterior or lateral approach, subject to surgeon experience and training [13]. Hence, we went forward with the DAA in our case. Since no muscles are actually cut, but only split in the DAA, we could mobilize the patient immediately from the next post-operative day, which helped avoid a lot of complications associated with a patient being bedridden for a prolonged period after a bilateral hip procedure. Due to this, the patient was able to walk without support and perform his activities of daily living within 2 months. The Harris Hip Score is a 100-point system that assesses pain, function, range of motion, and deformity, with a higher score indicating a better outcome [2]. At 4 months follow-up, the Harris Hip Score in our case was 86, which was categorized as excellent.
Low-energy bilateral femoral neck fractures in young adults should be evaluated thoroughly for metabolic bone disease. Simultaneous bilateral THA using DAA, performed in a single sitting, can offer excellent functional recovery, early mobilization, high patient satisfaction, reduced hospital stay, and patient morbidity. However, larger prospective studies and randomized controlled trials are needed before universal adoption of this technique.
Low-energy bilateral NOF fractures need prompt evaluation for metabolic bone disease. THA is a superior option in younger patients with poor bone quality. Single-stage bilateral THA, though technically demanding, is safe and effective with proper planning. DAA offers muscle-sparing benefits and allows for early ambulation.
References
- 1. Moghamis IS, Mudawi A, Babikir E, Elamin MH, Samhadaneh MA, Hameed SA. Bilateral femoral neck fracture following a convulsion in the presence of chronic kidney disease. A case report. Int J Surg Case Rep 2021;89:106545. [Google Scholar] [PubMed]
- 2. Li F, Zhu L, Geng Y, Wang G. Effect of hip replacement surgery on clinical efficacy, VAS score and Harris hip score in patients with femoral head necrosis. Am J Transl Res 2021;13:3851-5. [Google Scholar] [PubMed]
- 3. Blomfeldt R, Törnkvist H, Ponzer S, Söderqvist A, Tidermark J. Comparison of internal fixation with total hip replacement for displaced femoral neck fractures. Randomized, controlled trial performed at four years. J Bone Joint Surg Am 2011;93:445-50. [Google Scholar] [PubMed]
- 4. Ben S, Gordon B. Displaced intracapsular neck of femur fractures in mobile independent patients: Total hip replacement or hemiarthroplasty. Injury 2007;30:345-8. [Google Scholar] [PubMed]
- 5. Mathur H, Shah S. A rare case of bilateral fracture neck femur treated with bilateral distal loading stem total hip arthroplasty, in a single sitting. J Orthop Case Rep 2020;10:9-11. [Google Scholar] [PubMed]
- 6. Christensen CP, Karthikeyan T, Jacobs CA. Greater prevalence of wound complications requiring reoperation with direct anterior approach total hip arthroplasty. J Arthroplasty 2014;29:1839-41. [Google Scholar] [PubMed]
- 7. Wang Z, Hou JZ, Wu CH, Zhou YJ, Gu XM, Wang HH, et al. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J Orthop Surg Res 2018;13:229. [Google Scholar] [PubMed]
- 8. Sheth D, Cafri G, Inacio MC, Paxton EW, Namba RS. Anterior and anterolateral approaches for THA are associated with lower dislocation risk without higher revision risk. Clin Orthop Relat Res 2015;473:3401-8. [Google Scholar] [PubMed]
- 9. Barton C, Kim PR. Complications of the direct anterior approach for total hip arthroplasty. Orthop Clin North Am 2009;40:371-5. [Google Scholar] [PubMed]
- 10. Jia F, Guo B, Xu F, Hou Y, Tang X, Huang L. A comparison of clinical, radiographic and surgical outcomes of total hip arthroplasty between direct anterior and posterior approaches: A systematic review and meta-analysis. Hip Int 2018;29:584-96. [Google Scholar] [PubMed]
- 11. Anterior Total Hip Arthroplasty Collaborative Investigators, Bhandari M, Matta JM, Dodgin D, Clark C, Kregor P, et al. Outcomes following the single-incision anterior approach to total hip arthroplasty: A multicenter observational study. Orthop Clin North Am 2009;40:329-42. [Google Scholar] [PubMed]
- 12. Hartford JM, Bellino MJ. The learning curve for the direct anterior approach for total hip arthroplasty: A single surgeon’s first 500 cases. Hip Int 2017;27:483-8. [Google Scholar] [PubMed]
- 13. Ang JJM, Onggo JR, Stokes CM, Ambikaipalan A. Comparing direct anterior approach versus posterior approach or lateral approach in total hip arthroplasty: a systematic review and meta-analysis. Eur J Orthop Surg Traumatol. 2023 Oct;33(7):2773-2792. doi: 10.1007/s00590-023-03528-8. Epub 2023 Apr 3. PMID: 37010580; PMCID: PMC10504117. [Google Scholar] [PubMed] [CrossRef]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes
May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes