
It is imperative to identify these complex lesions and appropriate approach has to be planned.
Dr. Karthik D, Department of Orthopaedics, Manipal Hospital, Bengaluru, Karnataka, India. E-mail: Karthikdsetty1994@gmail.com
Abstract
Introduction: Although bucket-handle meniscal tears are common injuries, simultaneous bicompartmental displaced bucket-handle tears involving both the medial and lateral menisci are exceedingly rare. This study highlights the challenges posed by bicompartmental bucket handle tears in terms of anatomical considerations and the technical challenges for repairing the menisci in a previously reconstructed anterior cruciate ligament (ACL) knee.
Case Report: We report the case of a 31-year-old man who presented with acute knee pain during trampoline sports. The patient had undergone arthroscopic ACL reconstruction using a hamstring graft 2 years prior. On clinical examination, the patient had a knee range of motion of 10–90°, medial and lateral joint line tenderness, and positive McMurray tests for the medial and lateral menisci. Magnetic resonance imaging revealed bicompartmental displaced bucket handle tears and an ACL graft in situ with intact tunnels. Arthroscopic surgery was performed using a combination of all-inside and outside-in techniques to repair both tears. Outcomes: The patient underwent clinical examination at 1, 3, 6, and 12 months postoperatively. The patient achieved a knee flexion of up to 130° and hyperextension of 10° (same as the other knee) by the end of 2 months. The Lachman test after 2 months revealed no laxity of the ACL. The patient returned to unrestricted sports activity by 6 months postoperatively. At the 12-month follow-up, he remained symptom free, with a Lysholm score of 96.
Conclusion: A hybrid surgical technique combining all-inside and outside-in methods allows successful management of complex bicompartmental meniscal tears, preserving meniscal function while minimizing surgical risks. Level of Evidence: Level V, Expert Opinion/Case Report.
Keywords: Bicompartmental meniscal tear, trampoline-related knee injury, Meniscal repair techniques.
Meniscal injuries are among the most frequent intra-articular knee pathologies, particularly in young and athletic populations. Bucket-handle tears represent severe longitudinal tears in which a central fragment is displaced toward the intercondylar notch. These are typically observed in the medial meniscus and are often associated with anterior cruciate ligament (ACL) injuries. Bicompartmental bucket-handle tears are exceedingly rare, with only a few cases documented in the literature so far [1]. To the best of our knowledge, this is the first reported case of a bi-compartmental bucket-handle meniscus tear in a previously reconstructed intact ACL sustained due to trampoline use. Various surgical techniques have been developed to manage meniscal tears, with arthroscopic all-inside, outside-in, and inside-out techniques all having roles depending on tear location and morphology [2]. This case highlights the successful use of a combined arthroscopic all-inside and outside-in approach to treat a bicompartmental displaced bucket handle tear in a previously reconstructed ACL.
A 31-year-old male sustained a twisting injury to his left knee following a mis-landing of a flip while landing on a trampoline. The patient reported immediate pain, joint locking, and inability to fully extend the knee. The patient had a history of ACL reconstruction performed a year ago at another center. Physical examination revealed medial and lateral joint line tenderness, a positive McMurray test, and a fixed flexion deformity of 10°. Stability testing revealed negative Lachman and Anterior Drawer tests. Distal neurovascular deficits were ruled out. Plain knee radiography showed no abnormality in the bone structure. Sagittal sections of magnetic resonance imaging (MRI) revealed displaced bucket-handle tears involving both the medial and lateral menisci, exhibiting the classical “Double PCL” sign (Fig. 1).
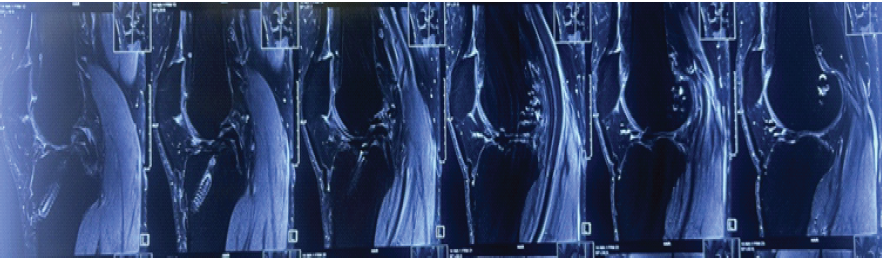
Figure 1: Double posterior cruciate ligament sign indicative of bucket handle medial meniscus tear.
The medial fragment was displaced into the intercondylar notch; the lateral tear extended into the anterior horn. There was no tunnel widening. The reconstructed ACL graft appeared to be intact. However, the femoral tunnel is more vertical, indicating the trans-tibial technique for the graft placement. Arthroscopy was performed under spinal anesthesia with the patient in the supine position and under tourniquet. Standard anterolateral and anteromedial portals were used. During the first view of diagnostic arthroscopy, the displaced medial and lateral meniscus bucket-handle fragments with the intact ACL were visualized (Fig. 2). No cartilage changes were encountered.
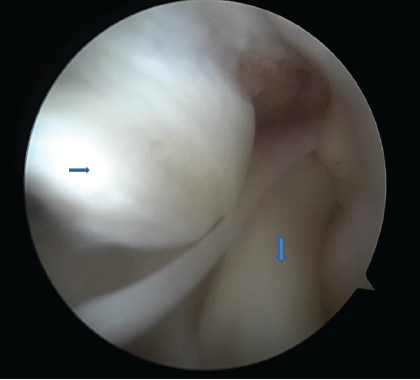
Figure 2: Displaced both meniscus bucket handle tear in the center of the knee joint (right pointing arrow – displaced medial meniscus bucket handle tear, down arrow – displaced lateral meniscus bucket handle tear.
The torn meniscus edges were freshened using a rasp and shaver to promote healing and remove perisynovial tissue. A trocar was used to push the bucket-handled part of the meniscus to its original place close to the capsule. The outside-in reduction stitch was deployed first to reduce and hold the meniscus in place for both the medial and lateral menisci. Identifying the anterior edge of the medial collateral ligament by palpation is very imperative and serves as an important landmark because the first outside-in should be placed in the mid-body of the meniscus. A box stitch configuration is used to peripheralize the meniscus and prevent the meniscus from entering the center of the joint and thus aiding in further vision for all inside stitches (Fig. 3).
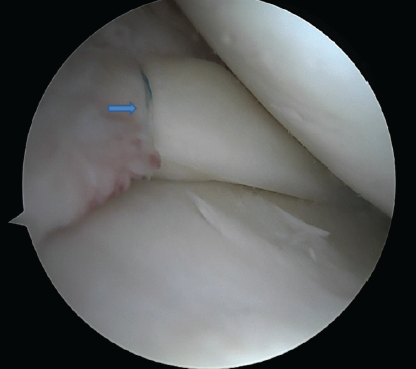
Figure 3: Reduced medial meniscus with a single outside-in stitch.
A simple and inexpensive technique was used for outside-in stitches. An 18-gauge spinal needle, which is pre-loaded with no.1 polydioxanone (PDS), is inserted into the joint cavity from outside to inside and passed through the upper surface of the meniscus. For a medial meniscus tear, the viewing portal is the anterolateral portal, and instrumentation is through the anteromedial portal. For a lateral meniscus tear, it is usually the opposite. However, the versatility of changing the portals or even an additional trans-patellar tendon portal is often necessary. Once the PDS is successfully inserted into the joint through the 18-gauge needle, it is retrieved through the anteromedial portal. A simple knot is made with the end of the PDS through which a No. 0 FiberWire is passed. The PDS from the side of the joint is pulled back. Along with the PDS, the FiberWire gets railroaded across to the side of the joint. The spinal needle was inserted again through the same skin puncture point, changing the direction subcutaneously to ensure the spinal needle passes between the lower surface of the meniscus and tibial plateau. The process is repeated, and both ends of FiberWire are retrieved to the medial side of the joint. A safety incision is made to retrieve both ends of the FiberWire. It is important to ensure that the soft tissue between the 2 ends of FiberWire is cleared to allow the stitch to sit on the capsule. An Aberdeen sliding knot is made and reduced to adequate tightness to ensure that the meniscus tear is closely approximated, but at the same time, avoid over-tightening. Then, subsequent half-hitch knots are made. For the lateral meniscus, the outside-in stitches were applied just anterior to the popliteus muscle. Once both the menisci were well peripheralized, the floppy posterior parts of the menisci were addressed using all-inside stitches. The posterior horn of the lateral meniscus was repaired with three vertical mattress sutures using the all-inside 24° DePuy Mitek device (Truespan meniscal repair system) at an interval of 5–10 mm from each other. Most of the devices come with 18 mm as a pre-set depth on opening the package. In total, 18 mm will be sufficient for most tears except when placing the stitch in the central part of the meniscus. The medial meniscus exhibited a displaced bucket handle tear extending from the body to the posterior horn. Initially, the meniscus was reduced using a trocar. The anterior horn and the body were repaired employing an outside-in technique using an 18-gauge spinal needle and No. 2-0 FiberWire. The posterior horn was repaired with 2 all-inside sutures (12° DePuy Mitek). While repairing the medial meniscus, its paramount to hold the knee in 20–30° of flexion and valgus stress to be provided to open up the medial joint space (Figs. 4 and 5).
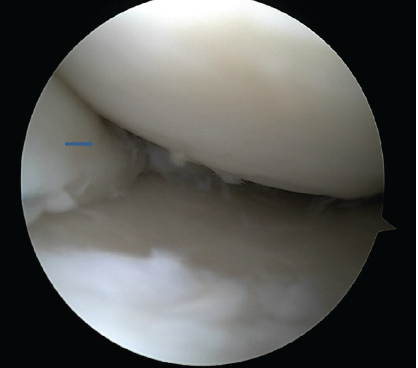
Figure 4: Completely reduced medial meniscus tear with a combination of outside-in and all inside stitches (right arrow shows completely reduced and peripheralized meniscus).
Once both the menisci were repaired, the knee joint was taken through the full range of motion (ROM). In addition, a meniscal stress test was performed to check for any inherent instability in the constructs of meniscal repairs.
The ACL was probed again. Although ACL fibers were vertically aligned, there was no laxity (Fig. 6).
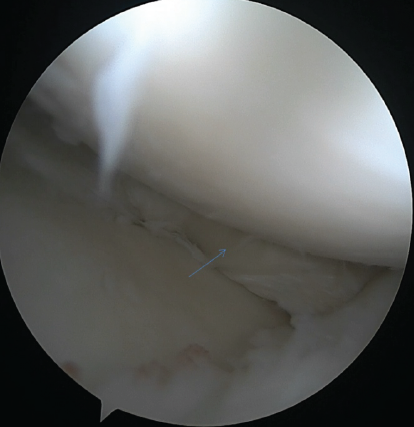
Figure 5: Completely reduced lateral meniscus tear with a combination of outside-in and all inside stitches (arrow indicating reduced lateral meniscus).
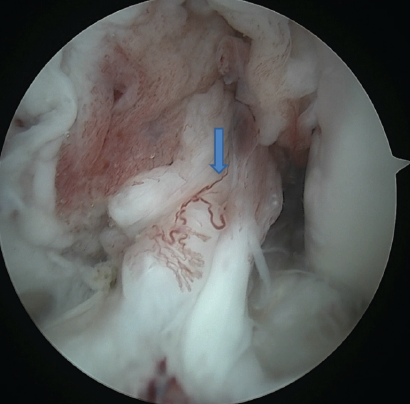
Figure 6: Intact previously reconstructed anterior cruciate ligament with vertical orientation of the graft (arrow indicates the orientation of the graft).
Post-operative rehabilitation protocol included:
- Weeks 0–4: Non-weight-bearing, 0–40° Knee ROM for the first 2 weeks and up to 90° flexion for the next 4 weeks
- Week 4 onwards: Progressive weight-bearing as tolerated
- Week 8 onwards: Quadriceps and hamstring strengthening, Gait training
- Weeks 12 onwards: Agility training and proprioception exercises
- Month 6: Return to sports.
At the 6-month follow-up, the patient was able to fully return to sports. The patient did not have any symptoms of locking or instability. His Lysholm score was 96 at 6 months post-surgery (pre-op: 45). Follow-up MRI at 6 months revealed no re-tears in the meniscus.
This report mainly tries to analyze the challenges in treating the rare condition, such as bicompartmental displaced bucket-handle tears. Second, it tries to analyze the role of the previous ACL reconstruction technique as a causative factor for such a rare injury. With both meniscal bucket handles sitting in the center of the joint, and the alteration of the meniscal landmarks such as anterior horns and intermeniscal ligaments adds to the challenge of successful reduction of the bucket handle tears. For the initial reduction of the bucket handled part of the meniscus, a trocar is an effective tool to push without tearing apart the meniscus tissue any further. For the all-inside stitch, the bucket handle tear on the opposite side comes in the way of inserting the all-inside device from the opposite side portal. Hence, reduction of both sides first by single outside-in stitches in the mid-portion of the bucket handles helps to reduce the menisci and hold them in place before proceeding with the rest of the stitches to fix the meniscal tears. The excellent functional recovery in our patient supports the efficacy of the combined approach. Medial meniscal bucket handle tears are more common due to the greater mechanical stress borne medially, while lateral involvement typically results from high-energy trauma [3]. The most common both compartment bucket-handle meniscus tears that have been reported were in association with an ACL injury [4,5]; however, they also occurred in an intact anterior cruciate ligament in certain cases [6,7,8]. In our patient, the possible contributing factor for injuring both the menisci could be the prior non-anatomic vertical ACL graft placement. As the femoral tunnel drilling is performed by the transtibial technique, it provides very minimal rotational stability. Femoral tunnel placement 10% deviation from anatomic position increases the subsequent risk of meniscal surgery after ACL reconstruction [9,10].
Bi-compartmental displaced bucket-handle meniscal tears are exceedingly uncommon, particularly in knees with previously reconstructed but intact ACL grafts. This case underscores the significance of recognizing such rare dual-compartment injuries and tailoring surgical strategy accordingly. The hybrid arthroscopic technique–integrating outside-in reduction with all-inside fixation seems to be an effective and reproducible method for restoring meniscal anatomy and preserving joint function. The successful outcome in this case suggests that, even in complex post-reconstruction scenarios, precise portal selection, controlled reduction, and meticulous suture placement are key to achieving stable meniscal repair and early functional recovery. Furthermore, this case highlights the potential influence of non-anatomic ACL graft positioning on meniscal biomechanics, emphasizing the need for anatomic reconstruction for better biomechanics. A long-term follow-up and larger series are warranted to validate the durability of this approach and to further elucidate the biomechanical interplay between reconstructed ACL alignment and meniscal injury risk.
The hybrid technique offers a superior approach in managing bicompartmental bucket-handle meniscal injury.
References
- 1. Poulsen MR, Johnson DL. Meniscal injuries in the young, athletically active patient. Phys Sportsmed. 2011 Feb;39(1):123-30. doi: 10.3810/psm.2011.02.1870. PMID: 21378495.. [Google Scholar] [PubMed] [CrossRef]
- 2. Barber FA, Herbert MA. Meniscal repair device. Arthroscopy 2000;16:613-8. [Google Scholar] [PubMed]
- 3. DeHaven KE, Lohrer WA. Meniscus repair. In: AAOS Atlas of Orthopaedic Surgery: Sports Medicine. Rosemont, IL: AAOS; 2006. [Google Scholar] [PubMed]
- 4. Kakel R, Russell R, VanHeerden P. The triple PCL sign: Bucket handle tears of both medial and lateral menisci in a chronically ACL-deficient knee. Orthopedics 2010;33:772. [Google Scholar] [PubMed]
- 5. Shepherd J, Abdul-Jabar HB, Kumar A. Locked bucket handle tears of the medial and lateral menisci with associated chronic ACL deficiency. J R Army Med Corps 2012;158:335-7. [Google Scholar] [PubMed]
- 6. Boody BS, Omar IM, Hill JA. Displaced medial and lateral bucket-handle meniscal tears with intact ACL and PCL. Orthopedics 2015;38:e738-41. [Google Scholar] [PubMed]
- 7. Wright J, Tamura C, Findlay I, Daneshfar A. Simultaneous bicompartmental bucket handle meniscal tears with a clinically competent anterior cruciate ligament. J Orthop Surg Res 2010;15:68. [Google Scholar] [PubMed]
- 8. Lykissas MG, Mataliotakis GI, Paschos N, Panovrakos C, Beris AE, Papageorgiou CD. Simultaneous bicompartmental bucket-handle meniscal tears with intact anterior cruciate ligament: A case report. J Med Case Rep 2010;4:34. [Google Scholar] [PubMed]
- 9. Inoue J, Giusto JD, Dadoo S, Nukuto K, Lesniak BP, Musahl V, et al. Nonanatomic femoral tunnel placement increases the risk of subsequent meniscal surgery after ACLR: Part II-patients without recurrent ACL injury. Knee Surg Sports Traumatol Arthrosc 2024;32:2780-9. [Google Scholar] [PubMed]
- 10. Hughes JD, Gabrielli AS, Dalton JF, Raines BT, Dewald D, Musahl V, et al. More anterior placement of femoral tunnel position in ACL-R is associated with postoperative meniscus tears. J Exp Orthop 2023;10:66. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 May 10, 2024 Buerger’s Disease of Hand; my Experience with Phenol Chemical Neurolysis of Stellate Ganglion: Case Series of Six Patients
May 10, 2024 Buerger’s Disease of Hand; my Experience with Phenol Chemical Neurolysis of Stellate Ganglion: Case Series of Six Patients April 7, 2014 Closed Talar Dislocation without Associated Fracture a Very Rare Injury, a Case Report
April 7, 2014 Closed Talar Dislocation without Associated Fracture a Very Rare Injury, a Case Report April 7, 2014 Fibrous Dysplasia of the Spine – A Case Involving Three Levels of Thoracic Spine
April 7, 2014 Fibrous Dysplasia of the Spine – A Case Involving Three Levels of Thoracic Spine November 1, 2024 Clostridium Septicum: Cause of Gas Gangrene in the Upper Extremity Leading to Proximal Trans-Humeral Amputation, A Review of Clostridium septicum
November 1, 2024 Clostridium Septicum: Cause of Gas Gangrene in the Upper Extremity Leading to Proximal Trans-Humeral Amputation, A Review of Clostridium septicum