
Metallosis-related osteolysis, though rare in knees, should be considered in patients with long-standing prostheses presenting with instability, swelling, and pain. Early revision surgery with synovectomy prevents catastrophic implant failure.
Dr. Abdulla Harafan, Department of Orthopaedics, Malabar Medical College, Men’s Hostel Room No. F-18, Modakkallur, Kozhikode, Kerala, India. E-mail: abdullaharafan123@gmail.com
Abstract
Introduction: Metallosis is a rare but recognized complication following total knee replacement (TKR). It is characterized by metallic particle deposition within periprosthetic tissue, triggering chronic inflammation, progressive osteolysis, and implant loosening.
Case Report: A 63-year-old female with bilateral TKRs, performed 12 and 15 years earlier, presented with pain, swelling, and restricted flexion of the right knee following a fall. She had a history of recurrent instability and locking for 3 years. Imaging revealed extensive osteolysis, polyethylene liner dissociation, and loosening of the tibial component. She underwent one-stage revision with implant removal, synovectomy, and implantation of a constrained modular revision prosthesis. Postoperatively, she showed stable function without recurrence.
Conclusion: Although uncommon in knee arthroplasty, metallosis can lead to catastrophic implant failure if undetected. Timely recognition and revision surgery with thorough synovectomy are essential to restore function and prevent further bone loss.
Keywords: Metallosis, Osteolysis, Polyethylene liner dissociation, Total knee replacement failure, Revision arthroplasty
Metallosis refers to the deposition of metallic wear particles in periprosthetic tissues, most commonly seen in metal-on-metal hip prostheses but less frequently in total knee replacement (TKR) [1,2]. It is associated with chronic inflammation, synovitis, and osteoclastic bone resorption, which may culminate in aseptic loosening of implants [3,4]. In TKR, metallosis may develop due to polyethylene liner wear or dissociation, failure of metal-backed components, or trauma leading to direct metal-on-metal articulation [5,6,7]. We present a case of severe metallosis-induced osteolysis and polyethylene liner dissociation causing failure of TKR, managed successfully with revision arthroplasty.
A 63-year-old female presented with pain, swelling, and reduced flexion in the right knee following a fall 2 months earlier. She also reported a 3-year history of recurrent instability, sudden locking, and restricted motion, which she occasionally relieved by self-manipulation. She had undergone bilateral TKR (left knee 15 years ago and right knee 12 years ago) using the Stryker Duracon system. At a local hospital, X-ray imaging, as shown in Figs. 1 and 2, revealed tibial component loosening, polyethylene liner dissociation, and marked osteolysis. Laboratory parameters (complete blood count, erythrocyte sedimentation rate, and C-reactive protein) were normal, excluding infection.
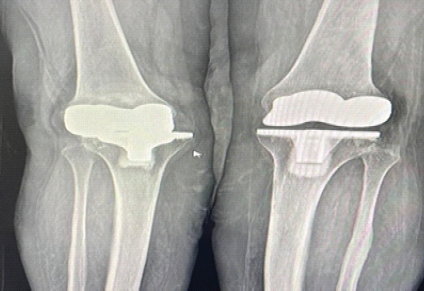
Figure 1: There is osteolysis, dislocation, and implant loosening in the right knee, whereas the left knee appears normal in anteroposterior X-ray.
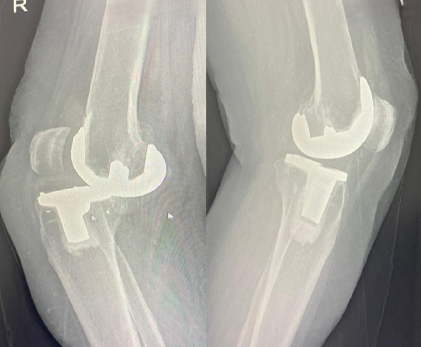
Figure 2: Dislocation is well noted in the lateral right knee X-ray, whereas the left knee appears normal.
On admission to our center, she had persistent swelling and pain with restricted mobility. A one-stage revision TKR was performed, involving implant removal, extensive synovectomy, and reconstruction with a constrained modular revision system. Intraoperative images, as per Fig. 3, show metallic debris and a worn-out polyethylene liner, which gives us a diagnosis of metallosis. Post-operative radiographs confirmed stable implants without evidence of loosening, as shown in Fig. 4.

Figure 3: Metallic debris, a worn-out polyethylene liner, gives us a diagnosis of metallosis.
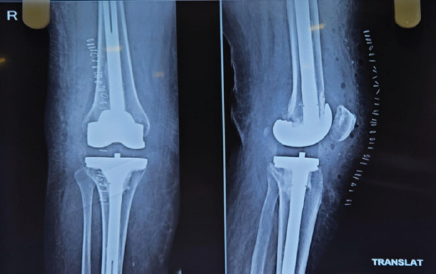
Figure 4: Post-operative X-ray following revision total knee replacement of the right knee.
At follow-up, the patient reported resolution of pain and improved mobility, with no recurrence of instability.
Metallosis results from the accumulation of metallic wear debris within periprosthetic tissues, triggering a chronic inflammatory cascade mediated by cytokines such as interleukin (IL-1), IL-6, IL-8, and tumor necrosis factor-α [3,8]. This immune reaction promotes synovitis, osteolysis, and progressive implant loosening. Although crepitus is a hallmark of hip prostheses, it is rarely described in knees [3]. In TKR, common etiologies include polyethylene liner wear, dissociation, or patellar component failure [6,7]. Rader et al. observed metallosis in 7 of 30 cases with metal-backed patellae, and more than half also showed liner dissociation [6]. In our case, tibial liner dissociation led to direct metal-on-metal contact, accelerating wear and osteolysis. Management requires revision arthroplasty combined with meticulous synovectomy, since conservative measures are ineffective [9]. Alternative prosthetic materials, such as oxinium, have been introduced to reduce metallic ion release and limit hypersensitivity reactions [10]. Our case reinforces the importance of vigilance even years after primary arthroplasty, as delayed metallosis-related osteolysis can compromise outcomes [4,11,12,13].
Severe metallosis following TKR is uncommon but can cause rapid osteolysis and catastrophic implant failure. Long-term surveillance of TKR patients is essential. Revision with thorough synovectomy and prosthetic replacement remains the definitive management.
Metallosis should be suspected in patients with late-onset pain, instability, and swelling after TKR. Revision surgery is the only effective treatment to prevent further destruction and restore function.
References
- 1. Wigren A, Fischer T. Allergic cobalt reaction (metallosis) following knee arthroplasty with vitallium endoprosthesis ad modum Walldius (author’s transl). Z Orthop Ihre Grenzgeb 1975;113:273-4. [Google Scholar] [PubMed]
- 2. Pritchett JW. Metallosis of the resurfaced hip. Orthopedics 2005;28:869-72. [Google Scholar] [PubMed]
- 3. Rader CP, Löhr J, Wittmann R, Eulert J. Results of total knee arthroplasty with a metal-backed patellar component. A 6-year follow-up study. J Arthroplasty 1996;11:923-30. [Google Scholar] [PubMed]
- 4. Sculco TP, Greenfield R, Walter RD. Metallosis after total knee replacement: Radiological-pathological conferences of the Massachusetts general hospital. Radiology 1998;208:345-8. [Google Scholar] [PubMed]
- 5. McGovern TF, Moskal JT. Radiographic evaluation of periprosthetic metallosis after total knee arthroplasty. J South Orthop Assoc 2002;11:18-24. [Google Scholar] [PubMed]
- 6. Chang JD, Lee SS, Hur M, Seo EM, Chung YK, Lee CJ. Revision total hip arthroplasty in hip joints with metallosis: A single-center experience with 31 cases. J Arthroplasty 2005;20:568-73. [Google Scholar] [PubMed]
- 7. Niki Y, Matsumoto H, Otani T, Tomatsu T, Toyama Y. Five types of inflammatory arthritis following total knee arthroplasty. J Biomed Mater Res A 2007;81:1005-10. [Google Scholar] [PubMed]
- 8. Romesburg JW, Wasserman PL, Schoppe CH. Metallosis and metal-induced synovitis following total knee arthroplasty: Review of radiographic and CT findings. J Radiol Case Rep 2010;4:7-17. [Google Scholar] [PubMed]
- 9. Schiavone Panni A, Vasso M, Cerciello S, Maccauro G. Metallosis following knee arthroplasty: A histological and immunohistochemical study. Int J Immunopathol Pharmacol 2011;24:711-9. [Google Scholar] [PubMed]
- 10. Vivegananthan B, Shah R, Karuppiah AS, Karuppiah SV. Metallosis in a total knee arthroplasty. BMJ Case Rep 2014;2014:bcr2013202801. [Google Scholar] [PubMed]
- 11. Sharareh B, Phan DL, Goreal W, Schwarzkopf R. Metallosis presenting as knee pain 26 years after primary total knee arthroplasty. J Orthop Case Rep 2015;5:62-5. [Google Scholar] [PubMed]
- 12. La Verde L, Fenga D, Spinelli MS, Campo FR, Florio M, Rosa MA. Catastrophic metallosis after tumoral knee prosthesis failure: A case report. Int J Surg Case Rep 2017;30:9-12. [Google Scholar] [PubMed]
- 13. Patel V. Metallosis following knee arthroplasty: A case report and review of literature. J Clin Orthop Trauma 2019;10:785-9. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series
July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series May 1, 2026 Diagnostic Accuracy of Synovial Alpha-Defensin and Histopathology for Periprosthetic Joint Infection: A Validation Study
May 1, 2026 Diagnostic Accuracy of Synovial Alpha-Defensin and Histopathology for Periprosthetic Joint Infection: A Validation Study August 1, 2025 Progressive Loosening in Metal-on-Metal Total Hip Arthroplasty after Fifteen Years of Effective Function: Two Case Reports
August 1, 2025 Progressive Loosening in Metal-on-Metal Total Hip Arthroplasty after Fifteen Years of Effective Function: Two Case Reports August 1, 2025 Polyethylene Insert Wear Leading to Early Aseptic Bilateral Total Knee Arthroplasty Failure: Case Report
August 1, 2025 Polyethylene Insert Wear Leading to Early Aseptic Bilateral Total Knee Arthroplasty Failure: Case Report