
Lipoma can also be intra-articular and affect patients’ function.
Dr. Shakil Ahmad, Department of Orthopaedic Surgery, Sohar Hospital, Sohar, Oman. E-mail: dr.shakilortho@gmail.com
Abstract
Introduction: Lipomas are common benign soft-tissue tumors typically found in subcutaneous regions. Intra-articular lipomas, however, are exceedingly rare and may present with functional impairment.
Case Report: A 27-year-old male presented with chronic right knee pain, limited flexion, and inability to run. Clinical examinations ruled out ligamentous or meniscal injuries. Magnetic resonance imaging revealed a 30 × 10 × 27 mm encapsulated intra-articular lipoma in the inferomedial recess of the anterior knee joint. The mass was excised surgically through a medial parapatellar approach, and histopathology confirmed a lipoma. Postoperatively, the patient regained a full range of motion and resolution of pain.
Conclusion: This case underscores the importance of considering intra-articular lipomas in differential diagnoses for chronic joint pain and restricted mobility. MRI remains pivotal for accurate diagnosis, and surgical excision ensures favorable outcomes.
Keywords: Intra-articular lipoma, knee joint, chronic pain, Magnetic resonance imaging, surgical excision
Lipomas are benign mesenchymal tumors composed of mature adipocytes, typically presenting as soft, mobile, and asymptomatic subcutaneous masses [1]. While prevalent in regions such as the trunk, neck, and extremities, their occurrence within joints is exceptionally rare, with limited documented cases in the medical literature. One case report has documented an intra-articular lipoma arising within the posterior compartment of the knee joint.[2] Intra-articular lipomas may manifest as space-occupying lesions and present clinically with symptoms of mass effect, most commonly pain and limited range of movement, and occasionally non-specific symptoms, such as locking, often mimicking more common pathologies such as meniscal tears or ligament injuries [3,4]. This locking is due to impingement and snapping of the patellofemoral joint [5]. Occasionally, they are diagnosed as incidental findings. This report details a case of an intra-articular lipoma located in the inferomedial recess of the anterior knee joint, highlighting diagnostic challenges, imaging findings, and therapeutic management. The clinical relevance lies in raising awareness of this rare entity to prevent misdiagnosis and ensure timely intervention.
Patient history
A 27-year-old male army employee presented with a 6-month history of progressive right knee pain, exacerbated during physical activity. He reported an inability to fully flex the knee or run, with no history of trauma or prior surgery.
Clinical examination
Physical examination revealed limited terminal flexion (0–110°). Anterior/posterior drawer, Lachman, McMurray, and varus/valgus stress tests were negative. No effusion or palpable mass was noted.
Imaging
Standing radiographs showed no abnormalities. Magnetic resonance imaging (MRI) demonstrated a well-encapsulated lobulated mass (30 × 10 × 27 mm) with fat-signal intensity in all sequences, located between the medial patellar facet and medial retinaculum, compressing Hoffa’s fat pad (Fig. 1). The cruciate ligaments and menisci were intact.
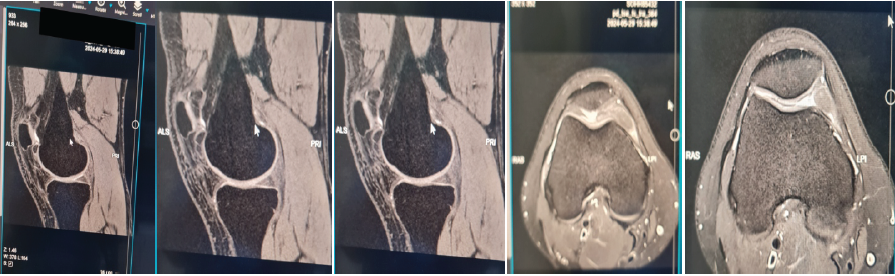
Figure 1: Sagittal magnetic resonance imaging (T1-weighted) images showing a hyperintense intra-articular mass in the inferomedial recess.
Surgical intervention
The patient underwent arthrotomy through a medial parapatellar approach. A yellowish, encapsulated mass was excised (Figs. 2 and 3). Histopathology confirmed mature adipocytes with fibrocollagenous septae, consistent with lipoma.
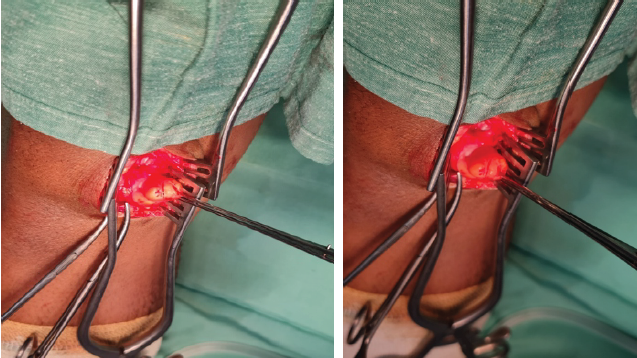
Figure 2: Intraoperative pictures of the encapsulated lipoma before excision.

Figure 3: Post-operative pictures of the encapsulated lipoma after excision.
Post-operative outcome
At the 3-month follow-up, the patient reported complete pain resolution and restored knee flexion (0–135°).
Intra-articular lipomas are rare, accounting for <1% of all lipomas. Their pathogenesis remains unclear, though associations with trauma, synovial metaplasia, or congenital anomalies have been proposed. Clinically, they may mimic intra-articular pathologies such as meniscal tears, synovial proliferative disorders, or loose bodies. There is a limited role of plain X-ray in the diagnosis of intra-articular lipoma. Small lipomas may not be detected, whereas larger lesions may feature isolated soft-tissue swelling with no other joint changes [6,7]. MRI is the gold standard for diagnosis [8], demonstrating homogeneous fat-signal intensity on T1- and T2-weighted sequences with suppression on fat-saturated images [9]. Differential diagnoses include lipoma arborescens, synovial chondromatosis, and pigmented villonodular synovitis [10] (Table 1). Unlike lipoma arborescens [11], which exhibits villous synovial proliferation, intra-articular lipomas are discrete, encapsulated masses.
Table 1: Differential diagnosis of intra-articular masses (Adapted from Sheldon et al.)
Surgical excision is curative, as evidenced by this case. Recurrence is rare, and post-operative rehabilitation focuses on restoring joint mobility.
This case highlights an intra-articular lipoma as a rare yet treatable cause of chronic knee dysfunction. Clinicians should maintain a high index of suspicion in patients with unexplained joint pain and motion limitations. MRI is indispensable for accurate diagnosis, and surgical excision ensures symptom resolution and functional recovery.
Intra-articular lipomas, though rare, warrant inclusion in the differential diagnosis of persistent knee pain with restricted mobility. Early imaging and intervention prevent prolonged morbidity.
References
- 1. Bancroft LW, Kransdorf MJ, Peterson JJ, O’Connor MI. Benign fatty tumors: Classification, clinical course, imaging appearance, and treatment. Skeletal Radiol 2006;35:719-33. [Google Scholar] [PubMed]
- 2. Bankaoglu M, Ugurlar OY, Ugurlar M, Sonmez MM, Eren OT. Intra-articular lipoma of the knee joint located in the posterior compartment: A rare location. North Clin Istanb 2017;4:89-92. [Google Scholar] [PubMed]
- 3. Yeomans NP, Robertson A, Calder SJ. Torsion of an intra-articular lipoma as a cause of pseudo locking of the knee. Arthroscopy 2003;19:E27. [Google Scholar] [PubMed]
- 4. Tudisco C, Farsetti P, Febo A. Solitary intra-articular lipoma locking the knee in a young boy. J Pediatr Orthop B 2008;17:131-3. [Google Scholar] [PubMed]
- 5. Yilmaz E, Karakurt L, Yildirim H, Ozercan R. Intra-articular lipoma causing snapping in the patellofemoral joint. Saudi Med J 2007;28:955-8. [Google Scholar] [PubMed]
- 6. Knapp EL, Kransdorf MJ, Letson GD. Diagnostic imaging update: Soft tissue sarcomas. Cancer Control 2005;12:22-6. [Google Scholar] [PubMed]
- 7. Dalla Rosa J, Nogales Zafra JJ. Large intra-articular true lipoma of the knee. BMC Musculoskelet Disord 2019;20:110. [Google Scholar] [PubMed]
- 8. Sheldon PJ, Forrester DM, Learch TJ. Imaging of intraarticular masses. Radiographics 2005;25:105-19. [Google Scholar] [PubMed]
- 9. Gaskin CM, Helms CA. Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. AJR Am J Roentgenol 2004;182:733-9. [Google Scholar] [PubMed]
- 10. Bui-Mansfield LT. Lipoma arborescens: Imaging features of typical and atypical disease and differentiation from other intra-articular pathology. Contemp Diagn Radiol 2021;44:1-5. [Google Scholar] [PubMed]
- 11. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: Radiologic-pathologic correlation. Radiographics 2008;28:1493-518. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge
October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair
June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair June 1, 2026 Atypical Bilateral Cystic Foot Swellings with Osteomyelitis-Like Features: A Diagnostic Dilemma
June 1, 2026 Atypical Bilateral Cystic Foot Swellings with Osteomyelitis-Like Features: A Diagnostic Dilemma May 1, 2026 Clinical and Radiological Outcomes of All-inside Versus Complete Tibial Tunnel Techniques in Anterior Cruciate Ligament Reconstruction using Hamstring Tendon Autograft: A Prospective Comparative Study
May 1, 2026 Clinical and Radiological Outcomes of All-inside Versus Complete Tibial Tunnel Techniques in Anterior Cruciate Ligament Reconstruction using Hamstring Tendon Autograft: A Prospective Comparative Study