
A planned fibular osteotomy can serve as an effective tool of biological dynamization in Fraser Type 1 fractures following damage-control fixation when timed appropriately within a staged treatment protocol.
Dr. Jeff Walter Rajadurai OR, Department of Orthopaedics, Madha Medical College and Research Institute, Chennai, Tamil Nadu, India. E-mail: jeffy.walter@gmail.com
Introduction: Floating knee injuries are among the most severe manifestations of musculoskeletal damage. They commonly come in with damaged soft tissues, a lot of blood loss, and people who are about to die from physiological collapse. It is never easy to take care of serious injuries. Every choice tries the delicate balance between biology and stability, especially when open wounds need both caution and urgency.
Case Report: A 22-year-old male, a chronic alcoholic with an O-negative blood group, was brought in after a high-velocity road traffic collision. Radiographs showed a Fraser Type I floating knee injury, a distal one-third femoral shaft fracture with a segmental tibial fracture classified as Gustilo-Anderson Grade IIIA. He underwent, in the first stage, retrograde titanium intramedullary (IM) nailing for the femur, combined with ankle-spanning external fixation and meticulous wound debridement, in accordance with the damage-control orthopedics principle. Three weeks later, once the soft tissues had settled, definitive fixation was carried out with closed suprapatellar IM nailing of the tibia. A planned same-level fibular osteotomy was added to encourage controlled compression and biological strain across the tibial fracture. This approach, echoing Wu’s concept of fibular osteotomy-assisted dynamization through stabilisation of the fibula (1996, 2001) and later refined as the stress-relieving fibular osteotomy by Vicenti (2019), allows the bone to heal under natural tension.
Conclusion: A well-planned osteotomy of the fibula may alter the course of events in such complicated floating-knee injuries. Well-timed in a staged damage-control setting, it provides a simple, biologically friendly method of promoting healing, fusing science and biomechanical art with surgical restraint.
Keywords: Floating knee, Fraser Type I, damage-control orthopedics, fibular osteotomy, biological dynamization.
Floating-knee, characterised by ipsilateral fractures of the femur and tibia, constitutes one of the most intricate and management-challenging injuries encountered by orthopedic surgeons [1,2]. They are frequently linked to significant soft-tissue injury, hemorrhage, and systemic compromise, rendering early definitive fixation perilous in physiologically unstable individuals. The idea of damage-control orthopedics (DCO) was created to put survival and systemic stability ahead of rebuilding [3,4]. The DCO technique has greatly cut down on problems, including acute respiratory distress, multi-organ failure, and infection, by staging fracture fixation. This means that external stabilization is done first, and then internal fixation is done later, once inflammatory and metabolic parameters return to normal. The Fraser Type I floating knee, which has a distal femoral shaft fracture and a segmental tibial fracture, is one of the most difficult types because it throws off the knee’s alignment and its biological environment. Open wounds, substantial soft-tissue stripping, and poor vascularity can all slow down healing, even when the fixation is technically correct [1,2,15]. So, biological optimization is just as important as mechanical stabilizing in the entire plan for care. In these complicated situations, intramedullary (IM) nailing is still the best way to solve things permanently since it can restore limb length, mechanical axis, and early load sharing [5,6,7,8,9,10]. For the femur, retrograde IM nailing enables fixation through a controlled articular approach with minimum disturbance to proximal soft-tissue, proving particularly advantageous when a simultaneous tibial fracture or external fixator limits conventional antegrade access [5,6]. The suprapatellar technique for the tibia allows for semi-extended posture and lowers the likelihood of malalignment that comes with proximal segment or segmental fractures [7,8,9,10]. These modern changes to IM nailing have made it easier to control the surgical parts of the procedure and less stressful for the patient during surgery. However, the biological concerns usually linger after the acute phase. When callus progression stops even when the fixation is stable, dynamization is a good second step. Controlled axial micromotion is reintroduced to drive callus development and endochondral ossification [11,12,13,14,16] by transforming a static construct into a dynamic one. However, when the fibula is intact, it can serve as a hard strut, protecting the tibia from compression and thereby restricting the desired biological stimulation. To address this issue, multiple authors have elucidated the function of fibular osteotomy, referred to as “fibular osteotomy-assisted dynamization” or “stress-relieving fibular osteotomy,” in reinstating physiological load transmission and promoting union [17,18,21]. The method enables the tibia to undergo regulated strain while maintaining axial alignment and the integrity of the implant. This case report details the staged DCO management of a 22-year-old male chronic alcoholic (O-negative blood group) with a Fraser Type I floating knee (Gustilo-Anderson Grade III), treated via retrograde femoral nailing, ankle-spanning external fixation, and delayed suprapatellar tibial nailing, with a planned same-level fibular osteotomy. The method not only mechanically completed the fixation but also functioned as a sort of biological dynamization, facilitating progressive, stress-mediated healing without the need for implant exchange. This instance underscores the enduring significance of phased fixation and regulated biological stimulation in intricate limb damage.
A 22-year-old man with a long history of chronic alcoholism and blood group O-negative was admitted to the emergency room following a high-speed road traffic accident. When he reached, he was hemodynamically unstable and had several abrasions, an open wound on his right leg, and a deformity in the distal thigh and leg. A local examination showed crepitus and abnormal movement at both the distal femur and mid-to-distal tibial levels. There was also an open wound that matched the Gustilo-Anderson Grade IIIA damage. The distal pulses were detectable, and the neurological assessment of the leg was unremarkable. Radiographs showed a fracture of the distal one-third of the femoral shaft on the same side and a segmental fracture of the tibial shaft. This is consistent with a Fraser Type I floating knee injury. A DCO approach was performed based on the physiological instability of the patient and the high contamination risk he presented. The patient also needed multiple blood transfusion to be hemodynamically stable. The first stage consisted of retrograde IM nailing of the femur, unilateral biplanar ankle-spanning external fixation for the tibia, and meticulous wound debridement with primary suturing under antibiotic cover. This was a balancing act that provided temporary skeletal stability with pain control and soft-tissue recovery with the least systemic further insult. The operation was carried out by inserting a solid nail made of titanium with interlocking screws, ensuring distal locking before engaging the proximal one to achieve anatomical reduction (Figs. 1,2,3).
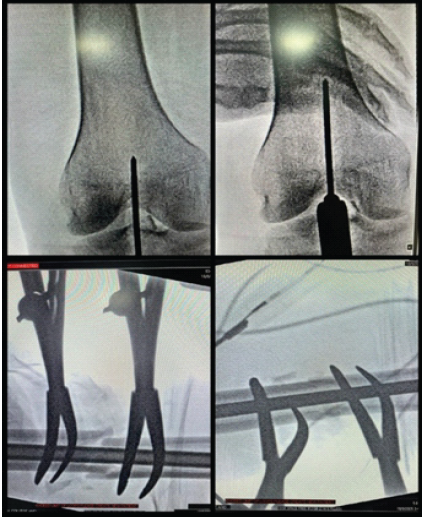
Figure 1: Intraoperative C-arm images showing retrograde femoral nail entry and reduction using clamps.

Figure 2: Immediate post-operative X-ray showing the temporary stabilisation of segmental tibia fracture.

Figure 3: 3-week old post-operative X-ray of retrograde femoral nail in situ
An ankle-spanning mono-lateral fixator to stabilize the alignment, allow access to the wound, and regular inspection was applied simultaneously. The soft tissue is debrided down to a healthy bleeding margin with pulsatile irrigation and closed primarily if possible (Fig. 4). The patient has received broad-spectrum intravenous antibiotics according to open fracture protocol.

Figure 4: Post-operative image after External Fixator application showing sutured open wound also.
The post-operative period course in the high-dependency unit was uneventful, the patient was resuscitated, and inflammatory and metabolic parameters were monitored for 48 h. The limb was elevated, and daily pin-site care was instituted. The static quadriceps exercises, passive knee flexion, and active and passive toe movements were started from post-operative day (POD)-1. Over the next days, the soft-tissue envelope showed an uneventful course of healing without any signs of infection.
The second stage of reconstruction, by which time soft-tissue healing had taken and inflammatory markers returned to normal, was performed at 3 weeks. The femoral shaft fracture by this time showed callus radiologically (Fig. 5, 6). The external fixator was removed, and closed suprapatellar IM nailing of the tibia (expert tibial nail) under fluoroscopic control undertaken. Intraoperative fluoroscopy confirmed accurate entry, guidewire placement and fracture reduction before reaming and nail insertion was done (Fig. 5, 6, 7,8, 9).
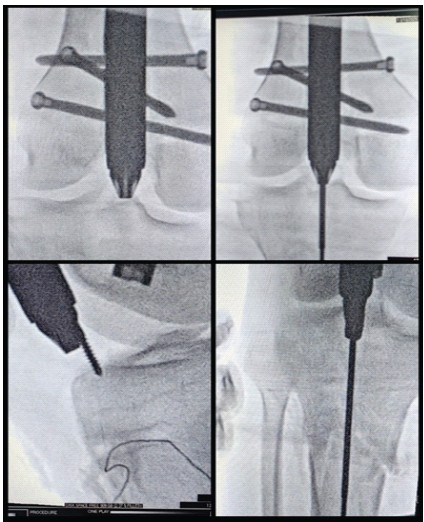
Figure 5: Intraoperative C-arm images showing the entry in both planes without disturbing the femoral nail.

Figure 6: Intraoperative C-arm images showing the supra-patellar tibial nail entry and pin playing the role of poller screw to centralize the guide wire.

Figure 7: Intraoperative C-arm image showing a curved osteotome and bone nibbler used for the fibular osteotomy, with a 5 mm Hohmann’s retractor employed to distort the forming callus and freshen the tibial edges.

Figure 8: Intraoperative C-Arm images of suprapatellar expert tibial nailing.

Figure 9: Immediate post-operative X-ray of segmental tibial shaft fracture with expert tibial nail in situ.
At the same sitting, an intended same-level fibular osteotomy as a small lateral incision over the distal third of the fibula was made creating a stress-relieving gap to permit controlled tibial compression (Fig. 7). A curved osteotome and bone nibbler were used for the fibular osteotomy. A 5 mm Hohmann’s retractor was employed to distort the forming callus and freshen the tibial edges.
Quadriceps strengthening and ankle mobilization were initiated postoperatively. Regular dressing of the wound was done (Fig. 10). Bilateral hip, knee, ankle, and quadriceps strengthening exercises were initiated on POD-1. The patient was encouraged to go for full weight bearing with walker support and tip-toe walking. The time of discharge was when the patient was adequately counseled with all necessary advice and precautions.

Figure 10: Post-operative image showing the wounds after External fixator removal and expert tibial nail in situ.
The floating knee is still one of the most serious injuries in trauma orthopedics, not because it happens very often, but because it causes so much biological havoc. When both the femoral and tibial shafts are broken at the same time, it turns a single-limb injury into a regional disaster. This requires an approach to treatment that takes into account both systemic physiology and local biology [1,2]. The initial classification was based on early studies by Blake and McBryde in 1975 and later by Fraser in 1978. More than 40 years later, treatment concepts are still changing as fixation advances and biological knowledge improve [1,2]. The decision to follow a DCO course was made because the patient’s body was unstable and his fractures were open. Pape et al. [3,4] have demonstrated that advocating for early definitive fixation in these patients can exacerbate the systemic inflammatory response, precipitate pulmonary problems, and elevate the risk of infection. The DCO approach, which means “stabilize first, reconstruct later,” has changed how trauma care works by giving damaged tissues time to heal before extensive repair. In this scenario, the first objective was simple and life-saving: To stop contamination, make the area less mechanically unstable, and preserve sensitive tissues. Retrograde femoral nailing, ankle-spanning external fixation, careful debridement, and temporary wound closure all helped to keep the area stable. This careful method helped the limb heal naturally while keeping the bones in proper alignment. The choice of retrograde femoral nailing for the femoral shaft fracture was intentional and based on evidence. Ricci et al. [5] and Ostrum et al. [6] showed that retrograde nailing is just as stable or even more stable than antegrade nailing, especially when the proximal thigh is weak or when tibial fixation is needed at the same time. It allows for anatomical reduction, early knee motion, and safe integration with lower-limb external fixators, which is an important part of floating-knee concepts. The suprapatellar semi-extended nailing technique for the tibia was a modern and well-thought-out solution because it is hard to do an infra-patellar nailing. Tornetta and Collins [7] were the first to talk about the method. Since then, Gelbke et al. [8], Eastman et al. [9], and Sun et al. [10] have all done cadaveric and clinical studies that indicate it works better at managing proximal fragments and minimizing malalignment. The surgeon can directly adjust coronal alignment with fluoroscopy while keeping the knee in a semi-extended position, which also protects the patellar tendon. The Schanz pin from the previous external fixator acted as a poller screw to center the guide wire during surgery. In the staged context, it offered a clear and predictable pathway for definitive fixation when soft-tissue conditions were optimal. Even when the best fixation was achieved, complicated tibial fractures often go for delayed union without any problems because the construct is too rigid. The lack of interfragmentary tension diminishes endochondral activity, resulting in a condition of “mechanical silence” at the fracture site. The principle of dynamization, initially introduced by Küntscher and subsequently validated by Perumal et al. [11], Pesciallo et al. [12], and Vaughn et al. [13], redefines regulated micromotion that promotes bone formation through mechanotransduction pathways. When done during the 8–16-week biological window, union rates can be higher than 85–90%, especially for tibial fractures [11,12,13,14]. But having an intact fibula, even though its healing modifies how the load is divided out. It acts as a stiff side strut, keeping the tibia from being compressed along its length and going against the fundamental principle of dynamization. The conceptual importance of fibular osteotomy lies in its targeted, biologically valid methodology that restores balance between stress and strain. Elshahhat et al. [17], Gálvez-Sirvent et al. [18] demonstrated that both biomechanically and clinically, same-level fibular osteotomy facilitates axial loading through the tibia, resulting in measurable shortening and expedited recovery [19,20]. Vicenti et al. [21] and other modern authors have talked about this idea more and called it “stress-relieving fibular osteotomy.” It means a change from only mechanical dynamization to biological dynamization. In this case, performing a planned fibular osteotomy on a united fibular fracture together with closed suprapatellar nailing turned a structure that could have been inactive into a dynamic, functional environment. By creating a controlled break in the fibula, physiological load transfer was restored, allowing the tibia to move slightly. It was a planned and biologically sound choice to do the second Stage 3 weeks after the first fixation. The first inflammatory storm had passed, the soft tissues had gotten their blood flow back, and the wound bed had gotten stable enough to sustain more harm. Moving too quickly could have caused the structure to come apart; waiting too long, as Ferreira et al. [16] and Yu et al. [14] pointed out, makes the body less able to recover itself. The current patient is expected to achieve cortical bridging within this constrained yet critical timescale of 8 weeks and gain complete functional recovery by 5 months, signifying healing in both osseous and biological systems. This experience validates a core tenet in trauma practice: Dynamization is not a corrective measure but an intentional biological process. When done with care and purpose, it restores the balance between mechanical stability and biological vigor. Too much fixation or too long of rigidity can easily throw this equilibrium off. The management’s expertise is not in the intricacies of the hardware, but in the systematic arrangement of meticulously considered options that consider the patient’s physiology and the limb’s biology. Orthopedic specialists are changing the way they think about things. Instead of just healing things, they are now regulating them and regenerating them instead of putting them together. The surgeon goes beyond just mending the mechanical parts by carefully mixing DCOs, modern nailing ideas, and fibular-osteotomy-assisted biological dynamization. This makes the surgeon a biological architect, setting the scene for nature to finish the job. This viewpoint is especially potent in areas with scarce resources. It joins together without too many implants, protects the donor site, and follows Küntscher’s long-held belief that limited mobility strengthens bone. From the viewpoint of modern mechanobiology, it concept maintains its poetic nature and truthfulness.
The present instance serves as a reminder that in complicated limb injuries, timing, staging, and biological intuition are just as important as the choice of implant. In a Fraser Type I floating knee, the patient was able to make the transition from temporary stabilisation to definitive fixation only after both systemic stability and local tissue health had recovered. This was possible because of the meticulous application of a DCO regimen. The combination of retrograde femoral nailing and suprapatellar tibial nailing kept the alignment and strength while still being careful with the soft-tissue envelope. Adding a planned same-level fibular osteotomy transformed the whole biological landscape of the limb, making it more flexible and able to breathe, adapt, and recover. It reactivated the tibia’s natural healing rhythm through biological dynamization by enabling regulated axial loading. The outcome conveys a subtle yet lasting message: the intentional integration of dynamization into the treatment plan unifies mechanics and biology. Even with improved fixation methods and precise implants, the best results still depend on the surgeon’s ability to decide when to let stability give way to motion.
True fracture healing arises when mechanical stability is balanced with biological motion.
References
- 1. Blake R, McBryde A Jr. The floating knee: Ipsilateral fractures of the tibia and femur. South Med J 1975;68:13-6. [Google Scholar] [PubMed]
- 2. Fraser RD, Hunter GA, Waddell JP. Ipsilateral fracture of the femur and tibia. J Bone Joint Surg Br 1978;60-B:510-5. [Google Scholar] [PubMed]
- 3. Pape HC, Giannoudis PV, Krettek C. The timing of fracture treatment in polytrauma patients: Relevance of damage control orthopedic surgery. Am J Surg 2002;183:622-9. [Google Scholar] [PubMed]
- 4. Giannoudis PV, Hildebrand F, Pape HC. Damage control orthopaedics: State of the art. Injury 2004;35 Suppl 1:S1-7. [Google Scholar] [PubMed]
- 5. Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-9. [Google Scholar] [PubMed]
- 6. Ostrum RF, Agarwal A, Lakatos R, Poka A. Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501. [Google Scholar] [PubMed]
- 7. Tornetta P 3rd, Collins E. Semiextended position for intramedullary nailing of the tibia. J Orthop Trauma 1996;10:92-5. [Google Scholar] [PubMed]
- 8. Gelbke MK, Coombs D, Powell S, DiPasquale T. Suprapatellar versus infra-patellar intramedullary nail insertion of the tibia: A cadaveric model for comparison of patellofemoral contact pressures and forces. J Orthop Trauma 2010;24:665-71. [Google Scholar] [PubMed]
- 9. Eastman JG, Tseng S, Lee MA, Yoo BJ, Wang J, Tornetta P 3rd. The use of the suprapatellar approach improves alignment in proximal tibial shaft fractures. J Orthop Trauma 2013;27:e212-7. [Google Scholar] [PubMed]
- 10. Sun Q, Nie X, Gong J Suprapatellar versus infrapatellar intramedullary nailing for tibial shaft fractures: A meta-analysis. Int Orthop 2016;40:1869-78. [Google Scholar] [PubMed]
- 11. Perumal R, Shankar V, Basha R, Jayaramaraju D, Rajasekaran S. Is nail dynamization beneficial after twelve weeks – An analysis of 37 cases. J Clin Orthop Trauma 2018;9:322-6. [Google Scholar] [PubMed]
- 12. Pesciallo CA, Deluca D, Olivero P. Effectiveness of nail dynamization in delayed union of tibial shaft fractures. Indian J Orthop 2021;55:125-31. [Google Scholar] [PubMed]
- 13. Vaughn JE, Shah RV, Samman T, Stirton J, Liu J, Ebraheim NA. Systematic review of dynamization vs exchange nailing for delayed/non-union femoral fractures. World J Orthop 2018;9:92-9. [Google Scholar] [PubMed]
- 14. Yu P, Huang L, Wang L, Cai L, Tu D. Nail dynamization for delayed union and nonunion in femur and tibia fractures following intramedullary nailing: A systematic review and meta-analysis. Injury 2025;56:112748. [Google Scholar] [PubMed]
- 15. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: Retrospective and prospective analyses. J Bone Joint Surg Am 1976;58:453-8. [Google Scholar] [PubMed]
- 16. Ferreira N, Tanwar YS, Burger M. The effect of fixation dynamization on fracture healing: A systematic review. J Limb Lengthen Reconstr 2020;6:7-12. [Google Scholar] [PubMed]
- 17. Elshahhat A, Khalifa M, Saleh M Combined dynamized nailing with partial fibulectomy for tibial nonunion. Eur J Orthop Surg Traumatol 2023;33:1181-9. [Google Scholar] [PubMed]
- 18. Gálvez-Sirvent E, Ibarzábal-Gil A, Rodríguez-Merchán EC. Treatment options for aseptic tibial diaphyseal non-union: A review of selected studies. EFORT Open Rev 2020;5:835-44. [Google Scholar] [PubMed]
- 19. Rüedi TP, Buckley RE, Moran CG, editors. AO Principles of Fracture Management. 3rd ed. Stuttgart: Thieme; 2018. [Google Scholar] [PubMed]
- 20. Müller ME, Allgöwer M, Schneider R, Willenegger H. Manual of Internal Fixation. 3rd ed. Berlin: Springer-Verlag; 1991. [Google Scholar] [PubMed]
- 21. Vicenti G, Bizzoca D, Carrozzo M, Nappi V, Rifino F, Solarino G, et al. The ideal timing for nail dynamization in femoral shaft delayed union and non-union. Int Orthop 2019;43:217-22. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2024 Ipsilateral Floating Hip and Floating Knee with Multiple Fractures – A Case Report
September 1, 2024 Ipsilateral Floating Hip and Floating Knee with Multiple Fractures – A Case Report February 10, 2024 Bilateral Floating Knee Injuries Managed by Intramedullary Nailing – An Unusual Injury
February 10, 2024 Bilateral Floating Knee Injuries Managed by Intramedullary Nailing – An Unusual Injury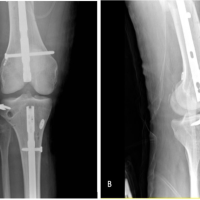 December 10, 2023 Multiligament Knee Reconstruction of the ACL, PLC, and ALL in a Floating Knee: A Case Report
December 10, 2023 Multiligament Knee Reconstruction of the ACL, PLC, and ALL in a Floating Knee: A Case Report February 10, 2021 Bilateral Periprosthetic Knee Fracture with the Right Floating Total Knee and Left Periprosthetic Patella Fracture Management Strategy: A Case Report
February 10, 2021 Bilateral Periprosthetic Knee Fracture with the Right Floating Total Knee and Left Periprosthetic Patella Fracture Management Strategy: A Case Report