
Calcific tendinitis should be considered in persistent lateral elbow pain unresponsive to conventional treatment, allowing for timely diagnosis and appropriate management.
Dr. Sandeep Mohan, Department of Orthopaedics, St Joseph’s Hospital, Karuvanchal, Kannur, Kerala, India. E-mail: sandeepmohan123@gmail.com
Abstract
Introduction: Calcific tendinitis is an uncommon disorder characterized by the deposition of calcium hydroxyapatite crystals in tendons, primarily affecting the rotator cuff and rarely involving the elbow. Misdiagnosis as lateral epicondylitis can lead to delayed management and persistent symptoms.
Case Report: We report a rare case of calcific tendinitis in a 46-year-old female presenting with refractory lateral elbow pain, initially misdiagnosed as lateral epicondylitis. Imaging confirmed calcific deposits within the lateral collateral ligament. Given the chronicity of symptoms and failure of conservative management, surgical intervention was performed, resulting in significant symptomatic relief and functional recovery.
Conclusion: This case underscores the importance of considering calcific tendinitis in persistent elbow pain unresponsive to conventional treatment. Advanced imaging modalities play a crucial role in diagnosis, whereas surgical excision remains a viable option for refractory cases.
Keywords: Calcific tendinitis, lateral epicondylitis, elbow pain, hydroxyapatite deposition, surgical excision.
Calcific tendinitis is a relatively uncommon musculoskeletal disorder characterized by the deposition of calcium hydroxyapatite crystals within tendons [1,2,3,4]. While it predominantly affects the rotator cuff in the shoulder, it can rarely involve other tendons, including those around the elbow. Its pathogenesis remains debated. Uhthoff proposed that reduced vascular perfusion induces metaplastic transformation of tenocytes into chondrocyte-like cells, promoting calcium deposition. The disease is believed to evolve from an initially silent phase of fibrocartilaginous change, through a symptomatic phase marked by deposition and painful resorption of calcium, to a final remodeling phase in which granulation tissue and vascularized scar replace the deposits [1,2,5,6]. This condition often presents with symptoms similar to more common disorders, such as lateral epicondylitis, which can lead to misdiagnosis and delayed management [7,8,9,10]. As calcific tendinitis remains an under-recognized cause of elbow pain, its clinical presentation can easily be mistaken for tennis elbow, resulting in prolonged discomfort and unnecessary treatment delays [7,8,9,10,11]. The diagnosis of calcific tendinitis typically relies on advanced imaging techniques, with radiography, ultrasonography (USG), and magnetic resonance imaging (MRI) playing pivotal roles in confirming the presence of calcium deposits and ruling out alternative pathologies [2,12,13,14]. Conservative management strategies, including rest, non-steroidal anti-inflammatory drugs (NSAIDs), and corticosteroid injections, are often effective for milder cases. However, for refractory cases where conservative measures fail to provide relief, surgical excision of the calcific deposits offers a definitive solution, providing significant symptomatic relief and restoring functional capacity [2,14,15,16]. In this article, we present a rare case of calcific tendinitis involving the common extensor tendon of the elbow in a 46-year-old female, initially misdiagnosed as lateral epicondylitis. This case highlights the diagnostic challenges and the importance of considering calcific tendinitis in persistent cases of lateral elbow pain that do not respond to conventional treatments. We further discuss the role of advanced imaging modalities in diagnosis and emphasize the value of surgical intervention in refractory cases.
A 46-year-old right-handed female presented with severe left elbow pain for the past 1 year. The pain has progressively worsened, persisting even at rest and aggravating with movements of the forearm and wrist, such as lifting objects. There was no history of trauma or overuse of the elbow. A similar episode occurred one year ago, which was diagnosed clinically as lateral epicondylitis. Initially managed by oral naproxen 500 mg twice daily for 3 weeks, resulting in partial pain relief. This was followed by a structured physiotherapy program over 4 weeks, comprising progressive resistance exercises targeting wrist extensors, eccentric strengthening, and stretching of the extensor carpi radialis brevis. The patient reported moderate improvement in symptoms after completion of the program. However, 2 months later, pain recurred with increased intensity that was treated with a single dose of 1 ampoule of local triamcinolone acetonide injection around the lateral epicondyle. The patient experienced significant symptomatic relief within 1 week, with pain subsiding almost completely over the following fortnight. No further rehabilitation or physiotherapy was given after the injection. After 1 year, she presented with unrelenting pain for 2 weeks and rated 8 on the Visual Analog Scale (VAS), which was significantly hampering her daily activities. On physical examination of the left forearm, there was tenderness over the lateral epicondyle of the humerus and the proximal radioulnar joint. Pain exacerbated on wrist extension, and both cozen’s and varus stress tests were positive. There was restriction of flexion at the elbow joint (100°), and the Mayo elbow performance score was 60. A plain radiography of the left elbow revealed calcific deposits at the lateral epicondyle, suggestive of calcific tendinitis (Fig. 1). To evaluate soft-tissue involvement, MRI was performed, revealing proton density fat-suppressed hypointense thickening of the lateral collateral ligament (Fig. 2), further corroborating the radiographic findings.

Figure 1: X-ray image showing calcific deposits at the lateral epicondyle.

Figure 2: Magnetic resonance image (coronal) showing proton density fat-suppressed hypointense thickening of the lateral collateral ligament.
Given the severity and resistance to conservative management, surgical intervention was planned. The procedure was performed under regional anesthesia using a supraclavicular brachial plexus block. The patient was placed in the supine position with the affected arm supported on an arm table. After standard antiseptic preparation and draping, a pneumatic tourniquet was inflated to 250 mmHg. A 5 cm longitudinal incision was made over the lateral epicondyle. The subcutaneous tissues were dissected using electrocautery to minimize bleeding. The fascia overlying the extensor origin was incised longitudinally to expose the common extensor tendon. The tendon was split in line with its fibers, revealing a white, paste-like calcific deposit within the substance of the extensor carpi radialis brevis. The deposit was carefully excised using small curettes and forceps. All visible dystrophic calcific deposits were removed(Fig. 3).

Figure 3: Surgical excision intraoperative image.
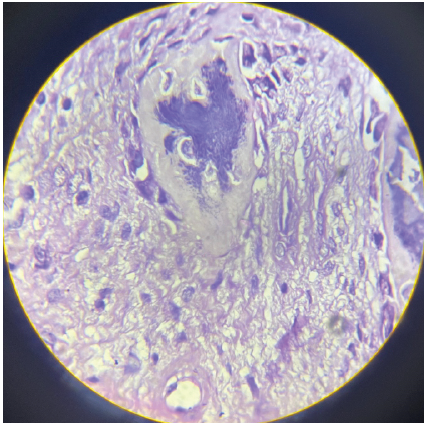
Figure 4: Histopathology slide showing calcium deposits within fibrous ligament tissue, accompanied by inflammatory infiltration.
The debrided area was irrigated with normal saline to remove residual calcium particles and reduce the risk of post-operative inflammation. The integrity of the remaining tendon was assessed, and the tendon was repaired with interrupted 3–0 polypropylene sutures to restore continuity. The wound was closed in layers with absorbable sutures for subcutaneous tissue and non-absorbable sutures for skin. A sterile dressing was applied, and the elbow was placed in a broad arm sling. No intraoperative complications were noted. Hemostasis was adequate. A compressive dressing was applied, and the elbow was immobilized in 90° flexion. Histopathological examination confirmed calcium deposits within fibrous ligament tissue, accompanied by inflammatory infiltration (Fig. 4). Antibiotic prophylaxis with ceftriaxone 1 g IV was administered preoperatively and continued for 24 h postoperatively. The patient was monitored for signs of infection, hematoma, and neurovascular compromise. Post-operative infection was a potential concern due to soft-tissue dissection and suture repair, but none occurred. The patient was educated on wound care and discharged on post-operative day 2 and followed up regularly. Early mobilization exercises helped minimize the risk of post-operative stiffness, which is a known complication of elbow surgery. No symptoms of lateral collateral ligament injury or iatrogenic nerve damage were noted. Preoperatively, the patient reported a VAS score of 8/10 and a limited active range of motion at the elbow (100° flexion) with significant impairment in daily activities, reflected by a disabilities of the arm, shoulder, and hand (DASH) score of 55. At the 2-week follow-up, the patient rated her pain as 5/10 on the VAS. Mild tenderness was noted over the lateral epicondyle on palpation, but the surgical site was healing well. A follow-up radiograph revealed complete resolution of the calcific deposit. At 6 months, the patient reported no pain (VAS 0/10), with restored elbow range of motion to 130° of flexion and full extension. Functional recovery was excellent, with a DASH score of 2 with no limitations in daily activities. At 1-year follow-up, the patient remained asymptomatic with full elbow function and strength with no signs of recurrence of calcific deposits. A summary of the patient’s clinical progress, functional outcomes, and imaging findings at each follow-up is presented in Table 1. Regular clinical and radiographic assessments confirmed sustained symptom resolution and joint preservation.
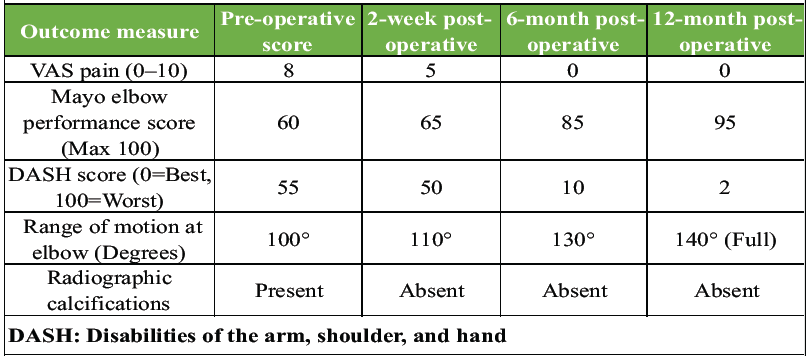
Table 1: Pre- and post-operative functional scores
Calcific tendinitis is characterized by the deposition of calcium hydroxyapatite crystals within tendons, predominantly affecting the rotator cuff and rarely the elbow. Its prevalence ranges from 2.7% to 20% [3], with a higher incidence in women aged 40–60 years [5]. Although typically involving the dominant limb, our case presented with calcific tendinitis in the non-dominant elbow, specifically the common extensor tendon. Sandstrom reported that only 6 out of 329 cases of calcific periarthritis involved the elbow [4]. Table 2 summarizes previously reported cases of calcific tendinitis in the elbow. Calcific tendinitis of the elbow remains exceedingly rare, with only a limited number of well-documented cases in the literature. In all three cases listed in Table 2, the patients were young to middle-aged women with a chronic history and initially misdiagnosed as lateral epicondylitis.
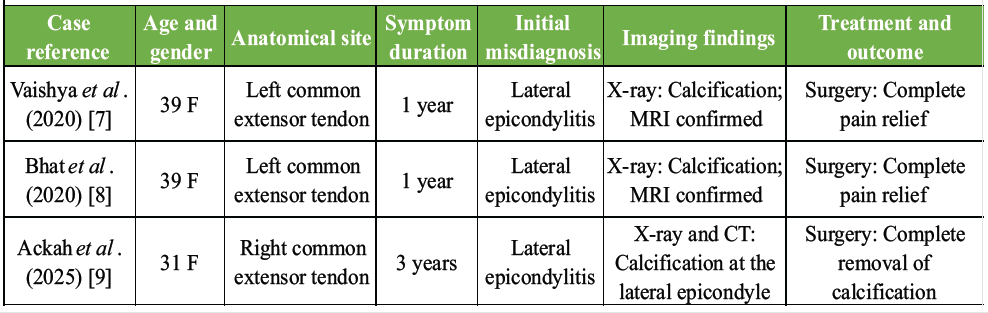
Table 2: Summary of previously reported cases of calcific tendinitis of the elbow
All cases involved the common extensor tendon and ultimately required surgical excision of calcific deposits after conservative treatment failed, resulting in complete pain relief and return of function. Our case mirrors this pattern in several aspects, such as female gender, chronic lateral elbow pain, misdiagnosis as lateral epicondylitis, and radiographic evidence of calcification in the common extensor tendon. However, unlike previous reports, we provide a longer follow-up of 1 year, a detailed surgical technique, and a comprehensive rehabilitation protocol, which are missing in earlier reports. While all previous cases opted for surgery after conservative management failed, the specifics of that conservative approach were often poorly described. In contrast, our case offers clarity on NSAID duration, physiotherapy protocol, and injection technique, filling a crucial gap in the literature. The small number of reported cases signifies the need for greater clinical suspicion, particularly when patients with presumed lateral epicondylitis fail to improve despite adequate conservative measures. This case reinforces the diagnostic value of early imaging, especially plain radiographs, to avoid delays in appropriate management. The precise etiology remains uncertain despite numerous hypotheses proposed over the decades. Among the most widely cited is the theory advanced by Uhthoff, who suggested that reduced vascular perfusion induces metaplastic transformation of tenocytes [1] into chondrocyte-like cells, ultimately resulting in the production and deposition of calcium hydroxyapatite. In this model, the disease progresses through a continuum of stages. The earliest stage is marked by fibrocartilaginous metaplasia within the tendon, generally occurring without clinical manifestations. The subsequent phase is characterized initially by the deposition of calcium and later by a resorptive process in which cellular proliferation and enzymatic colliquation of the calcific material take place. This stage is frequently accompanied by intense pain, attributed to chemical irritation and increased intratendinous pressure, and may be poorly responsive to standard analgesics. The final phase involves tendon remodeling, with calcium deposits gradually replaced by granulation tissue that matures into organized, vascularized scar tissue. Clinically, this stage is associated with subacute symptoms, often perceived as transient exacerbations of chronic discomfort before eventual resolution. Rui et al. proposed that tendon-derived stem cells may undergo aberrant differentiation into osteoblasts or chondrocytes, leading to calcification [17]. The clinical presentation varies, with 20% of cases being asymptomatic [5], whereas others experience acute pain, tenderness, swelling, and functional impairment. Due to overlapping symptoms, calcific tendinitis is frequently misdiagnosed as lateral epicondylitis [7,8,9,10,11], as in this case, where an initial diagnosis of tennis elbow delayed definitive treatment. Radiographic evaluation is the first-line diagnostic modality [12], revealing calcium deposits within the tendon. USG serves both diagnostic and therapeutic roles [2,13], delineating the location, size, and morphology of calcifications. MRI provides superior soft-tissue resolution [14], assessing tendon involvement and ruling out alternative pathologies such as tendon tears or soft-tissue masses, with a reported diagnostic accuracy of 95%. While Computed Tomography helps to confirm the diagnosis. Conservative management of calcific tendinitis includes physiotherapy, NSAIDs, ultrasound-guided needling (UGN), and extracorporeal shock wave therapy (ESWT) [2] that focuses on symptom relief and promoting the resorption of calcium deposits. NSAIDs are commonly used to alleviate pain and inflammation. Physical therapy plays a crucial role, incorporating stretching and strengthening exercises. Local corticosteroid injections may be administered for temporary relief of inflammation and pain. However, Smidt et al. reported that it is associated with high recurrence rates and poor outcomes [15]. UGN was performed on six non-shoulder calcific tendinitis patients, with only one case involving the common extensor tendon. The procedure led to an 80% reduction in calcium deposits, resulting in a good clinical outcome [13]. A recent study suggests that more evidence is needed to establish the efficacy of this technique [14]. ESWT is a safe and non-invasive procedure. In a study by Daecke et al, 70% patients had successful recovery and 20% required surgery [16]. While it is well-documented for shoulder calcific tendinopathy (CT), evidence for its effectiveness in non-shoulder CT remains limited. Furthermore, the procedure is expensive and painful, with significant disparity regarding the dosage and interval of administration. Kimura et al. reported that cimetidine, an H2 receptor antagonist, was effective in relieving pain and promoting the disappearance of calcific deposits in 56% of patients with CT, when administered orally at 200 mg twice a day [18]. However, its long-term effects remain unknown. Surgical excision is reserved for chronic and refractory cases, as in our case. It is a definitive treatment that ensures complete removal of calcific deposits but carries the risk of potential complications such as infection, nerve injury, and persistent pain or stiffness [19]. Excessive debridement may cause iatrogenic posterolateral rotatory instability. At the same time, injury to the posterior cutaneous nerve of the forearm (located 1.5 cm anterior to the lateral epicondyle) can lead to neuroma formation, causing persistent paresthesia. Other complications include seroma, fibrosis, reactive bone formation, and, rarely, recurrence as ossifying tendinitis. The differential diagnoses include lateral epicondylitis, radial tunnel syndrome, tendon tear, osteoarthritis, olecranon bursitis, ligament injuries, gout, pseudogout, and septic arthritis. Lateral epicondylitis and radial tunnel syndrome were ruled out due to imaging evidence of calcific deposits and absence of nerve compression. Osteoarthritis and olecranon bursitis were excluded based on the absence of characteristic imaging findings and posterior swelling, respectively. Tendon tears and significant ligament injuries were ruled out by MRI. Deposition diseases such as gout and pseudogout were excluded as the calcification pattern was consistent with hydroxyapatite crystals. Septic arthritis was unlikely due to the absence of systemic symptoms and infection markers. Table 3 outlines the key differential diagnoses and their distinguishing features. Ultimately, clinical evaluation and imaging confirmed calcific tendinitis as the definitive diagnosis, highlighting the necessity of considering this entity in persistent elbow pain.
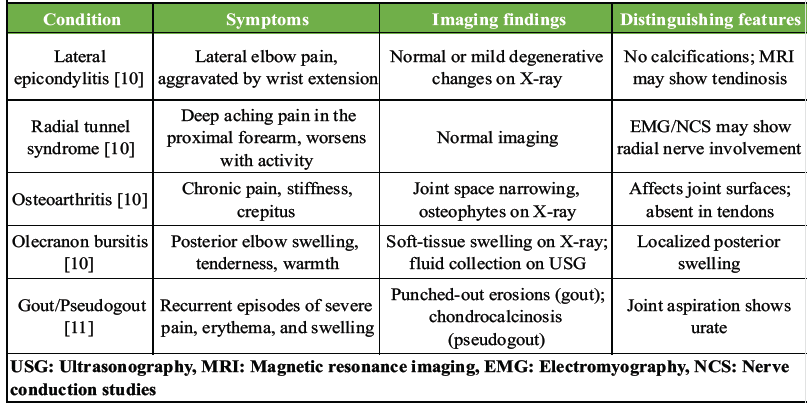
Table 3: Comparative overview of differential diagnoses
Calcific tendinitis of the elbow is a rare yet significant cause of lateral elbow pain, often misdiagnosed as lateral epicondylitis. This case illustrates the importance of recognizing atypical presentations and utilizing advanced imaging techniques for accurate diagnosis. Surgical excision provides a definitive solution for refractory cases, leading to substantial pain relief and functional restoration.
Calcific tendinitis of the elbow is a rare but important differential diagnosis for lateral elbow pain, often misdiagnosed as lateral epicondylitis. Advanced imaging plays a crucial role in accurate diagnosis, while conservative management is effective in many cases, surgical excision provides definitive relief in refractory cases.
References
- 1. Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: Pathogenesis, diagnosis, and management. J Am Acad Orthop Surg 1997;5:183-91. [Google Scholar] [PubMed]
- 2. Merolla G, Singh S, Paladini P, Porcellini G. Calcific tendinitis of the rotator cuff: State of the art in diagnosis and treatment. J Orthop Traumatol 2016;17:7-14. [Google Scholar] [PubMed]
- 3. Bosworth BM. Calcium deposits in the shoulder and subacromial bursitis: A survey of 12,122 shoulders. J Am Med Assoc 1941;116:2477-82. [Google Scholar] [PubMed]
- 4. Sandstrom C. Peritendinitis calcarea: A common disease of middle life: Its diagnosis, pathology, and treatment. Am J Roentgenol Radium Ther 1938;40:1-21. [Google Scholar] [PubMed]
- 5. DePalma AF, Kruper JS. Long-term study of shoulder joints afflicted with and treated for calcific tendinitis. Clin Orthop 1961;20:61-72. [Google Scholar] [PubMed]
- 6. Compagnoni R, Menon A, Radaelli S, Lanzani F, Gallazzi MB, Tassi A, et al. Long-term evolution of calcific tendinitis of the rotator cuff: Clinical and radiological evaluation 10 years after diagnosis. J Orthop Traumatol 2021;22:42. [Google Scholar] [PubMed]
- 7. Vaishya R, Siddalingeshwara GI, Vaishya A. Calcific tendonitis of the elbow in an adult – a case report and review of the literature. J Orthop Case Rep 2020;10:57-60. [Google Scholar] [PubMed]
- 8. Bhat AK, Bhaskaranand K, Nair NS. Calcific tendinitis of the elbow: A case report. J Orthop Case Rep 2020;10:23-5. [Google Scholar] [PubMed]
- 9. Ackah E, Xue D, Pan Z. Calcific tendonitis of the right epicondyle of the elbow: A case report. Medicine (Baltimore) 2025;104:e41604. [Google Scholar] [PubMed]
- 10. Kane SF, Lynch JH, Taylor JC. Evaluation of elbow pain in adults. Am Fam Physician 2014;89:649-57. [Google Scholar] [PubMed]
- 11. Moseley S, Akel A, Mse Adeen MA, Abu-Jeyyab M. A tennis elbow, a first presentation of gout disease. Orthop Rev (Pavia) 2022;14:39574. [Google Scholar] [PubMed]
- 12. Farin PU. Consistency of rotator-cuff calcifications. Observations on plain radiography, sonography, computed tomography, and at needle treatment. Invest Radiol 1996;31:300-4. [Google Scholar] [PubMed]
- 13. De Zordo T, Ahmad N, Ødegaard F, Girtler MT, Jaschke W, Klauser AS, et al. Us-guided therapy of calcific tendinopathy: Clinical and radiological outcome assessment in shoulder and non-shoulder tendons. Ultraschall Med 2011;32 Suppl 1:S117-23. [Google Scholar] [PubMed]
- 14. Vignesh KN, McDowall A, Simunovic N, Bhandari M, Choudur HN. Efficacy of ultrasound-guided percutaneous needle treatment of calcific tendinitis. AJR Am J Roentgenol 2015;204:148-52. [Google Scholar] [PubMed]
- 15. Smidt N, Van Der Windt DA, Assendelft WJ, Devillé WL, Korthals-De Bos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: A randomised controlled trial. Lancet 2002;359:657-62. [Google Scholar] [PubMed]
- 16. Daecke W, Kusnierczak D, Loew M. Long-term effects of extracorporeal shockwave therapy in chronic calcific tendinitis of the shoulder. J Shoulder Elbow Surg 2002;11:476-80. [Google Scholar] [PubMed]
- 17. Rui YF, Lui PP, Chan LS, Chan KM, Fu SC, Li G. Does erroneous differentiation of tendon-derived stem cells contribute to the pathogenesis of calcifying tendinopathy? Chin Med J (Engl) 2011;124:606-10. [Google Scholar] [PubMed]
- 18. Kimura H, Iwamoto T, Oki S, Matsumura N, Nakamura M, Matsumoto M, Sato K. Chronic calcific periarthritis of the elbow treated by cimetidine administration: Five cases. J Orthop Surg (Hong Kong). 2017 May-Aug;25(2):2309499017717193. doi: 10.1177/2309499017717193. PMID: 28659055. [Google Scholar] [PubMed] [CrossRef]
- 19. Merolla G, Bhat MG, Paladini P, Porcellini G. Complications of calcific tendinitis of the shoulder: A concise review. J Orthop Traumatol 2015;16:175-83. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Correlation of Serum Vitamin D Levels and Incidence of Lateral Epicondylitis of the Elbow: An Observational Study in Eastern India
January 1, 2026 Correlation of Serum Vitamin D Levels and Incidence of Lateral Epicondylitis of the Elbow: An Observational Study in Eastern India July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 A Prospective Randomized Controlled Study Comparing the Efficacy of Platelet Rich Plasma Injection versus Steroid Injection in Lateral Epicondylitis
July 1, 2026 A Prospective Randomized Controlled Study Comparing the Efficacy of Platelet Rich Plasma Injection versus Steroid Injection in Lateral Epicondylitis June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair
June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair