
Synthetic skin grafts, such as Hyalomatrix, are effective, safe, and cosmetically favorable options for skin deficit coverage in pediatric patients undergoing complex syndactyly reconstruction.
Dr. Hayley E Hansen, Department of Orthopaedic Surgery, Corewell Health William Beaumont University Hospital, MI, USA. E-mail: hayley.hansen@corewellhealth.org
Abstract
Introduction: Congenital syndactyly is described as the failure of two or more digits to separate, resulting in fusion of soft tissue or osseous structures. Although traditional techniques involving surgical release and skin grafting are cornerstones of syndactyly reconstruction, over the last decade the use of synthetic grafts for skin deficit coverage has become increasingly popular due to improved scar cosmesis and decreased rates of web creep.
Case Report: A 6-month-old Caucasian male with complete syndactyly of the third through fifth digits of bilateral hands underwent staged syndactyly reconstruction using Hyalomatrix synthetic graft coverage for skin deficits of the bilateral ring fingers, resulting in successful resolution of the skin deficits without scarring or significant web creep.
Conclusion: Synthetic skin grafts provide excellent coverage and cosmesis for skin deficits not amenable to primary closure during complex, complete syndactyly reconstruction in pediatric patients.
Keywords: Syndactyly, graftless syndactyly reconstruction, complex syndactyly, hyalomatrix, skin substitute.
Congenital syndactyly is the result of an embryologic failure of separation involving fingers or toes leading to soft tissue and, occasionally, bony fusion across digits. It is the most common congenital hand deformity with an incidence of 1 in 2000 live births. In addition, bilateral syndactyly occurs in nearly half of all cases [1]. If not addressed, syndactyly can be functionally debilitating, esthetically displeasing, and disrupt natural growth of the digits [2]. Current techniques for syndactyly reconstruction vary depending on the complexity and digits involved, with surgical intervention usually occurring between 12 and 24 months of life to improve patient function [3,4]. However, patients with syndactyly between the thumb and index and ring and small fingers can be considered for release prior to 6 months of age in order to prevent asymmetric growth of the digits and resultant joint contractures [4]. Historically, treatment of syndactyly has involved Bruner incisions between the digits, a proximal dorsal flap for recreation of the commissure, and utilization of full-thickness skin grafts from the forearm or groin for deficient skin coverage between digits [3,4,5,6]. However, skin grafting is associated with hypertrophic scarring, web creep, donor site pain, and abnormal hair growth or pigmentation [5,7]. Since first reported in 1990 by Niranjan and de Carpentier, graftless techniques for syndactyly reconstruction have become a popular treatment option to avoid these complications [5,7]. Synthetic skin graft alternatives, including Integra™ (Integra LifeSciences, Princeton, NJ, USA), Hyalomatrix™ (Medline Industries, Inc, Northfield, IL), and Pelnac™ (Gunze Limited, Kyoto, Japan), are additional options for skin coverage after syndactyly reconstruction where primary closure is unattainable [8,9,10,11]. In comparison to traditional skin grafts, synthetic grafts have the benefits of improved scar appearance and low rates of web creep, while also reducing the morbidity associated with skin graft harvest [8,9,10,11]. Hyaluronic acid (HA) is a glycosaminoglycan found in connective, epithelial, and neuronal tissues [12,13]. It serves a critical structural role in the extracellular matrix of cells as well as regulation of essential cellular processes, including cell adhesion, proliferation, and regeneration [12,13]. Studies have shown that rapid degradation of HA by hyaluronidase in vivo can cause the half-life of HA to decrease to <1 day, limiting its clinical applications [12]. To slow this degradation and prolong the overall acting-time of HA in wound repair, an esterified HA, Hyalomatrix, was developed. Hyalomatrix is a synthetic dermal matrix composed of HYAFF, HA that has undergone esterification with benzoyl alcohol. The inner layer of Hyalomatrix acts as a biodegradable scaffold that promotes neoangiogenesis and colonization by fibroblasts, while the exterior semipermeable silicone membrane acts as a barrier to the external environment [14]. Multiple studies have shown the usefulness of Hyalomatrix in the treatment of chronic wounds and focal cartilage defects [15,16,17]. Hyalomatrix has also proven beneficial in the treatment of pediatric syndactyly reconstruction, demonstrating improved cosmesis and less web creep than traditional skin grafts [9,10]. In this report, we discuss a patient with complete syndactyly of the third through fifth digits of bilateral hands who underwent two-stage syndactyly reconstruction necessitating Hyalomatrix synthetic graft coverage for deficits of bilateral ring fingers, resulting in complete resolution of the skin deficits without scarring or web creep.
The patient initially presented at 2 weeks of age to our clinic. The patient’s perinatal history was unremarkable. He was born at full term through uncomplicated vaginal delivery. He was found to have complete syndactyly of digits three through five of the bilateral hands and simple, incomplete syndactyly of digits two and three of the bilateral feet (Fig. 1).

Figure 1: Pre-operative photographs of the patient’s left and right hands, respectively, at 2 weeks of age, demonstrating complete syndactyly of digits three through five bilaterally.
On imaging, complex syndactyly of digits three and four of the left hand and digits four and five of the right hand were also identified (Fig. 2).
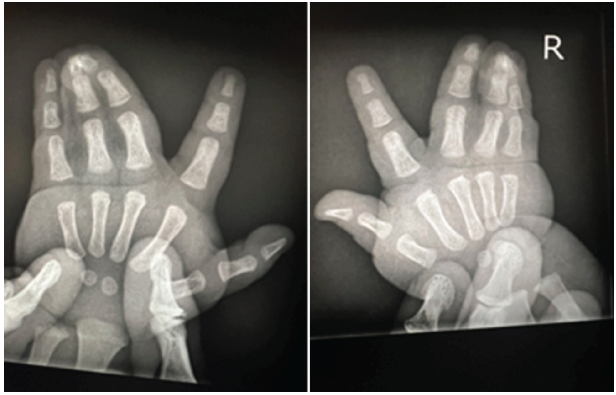
Figure 2: Pre-operative posterior-anterior radiographs of the left and right hands demonstrating complex syndactyly of digits three and four of the left hand and four and five of the right hand.
At the age of 6 months old, staged release of the affected digits was discussed with the patient’s parents. They wished to proceed with surgical management. The first stage was scheduled for when the patient turned 12 months old. Given the patient’s complete syndactyly involving two adjacent web spaces, a two-stage reconstruction was planned to reduce the risk of digital flap necrosis and possible digital artery injury. The patient was brought to the operating room for the first stage of the reconstruction. General anesthesia was induced and both hands were draped in the usual sterile fashion. The left hand was addressed first. A Bruner incision was made between digits four and five from the distal tips of the fingers to just proximal to the web space. In accordance with the technique first described by Smith and Harrison [18], a “seagull” shaped flap was made over the dorsal web space between digits four and five. Two oblique incisions were made starting from the volar web space and extending proximally over the skin superficial to the fourth and fifth metacarpal heads. The skin of the volar web space was then elevated and the digital neurovascular bundle was identified and protected. The dorsal “seagull” flap was elevated, defatted, and the redundant web space soft tissue released. The flap was then pulled between digits four and five and sutured into the volar skin defect with interrupted 5-0 Vicryl sutures. Skin between the digits was amenable to closure without the need for skin grafts or substitutes. The same procedure was performed on digits four and five of the right hand with the addition of separation of the bony connection between the distal phalanges using a #15 blade scalpel after localization via fluoroscopy. Clinical follow-up after the first stage revealed uneventful healing of the surgical incisions. Three months later, the patient returned to the operating room for the second stage of his syndactyly reconstruction. Again, the bilateral upper extremities were draped in the usual sterile fashion with bilateral upper arm sterile tourniquets. The left hand was addressed first. A longitudinal incision was made through the skin between digits three and four and a hexagonal dorsal skin flap was created at the web space. Paronychial fold reconstruction was performed using the double pulp flap technique, initially described by Buck-Gramcko [19]. These flaps were elevated with a #69 blade to the dorsal midline of the digits and defatted. Digital neurovascular bundles were identified on the volar aspects of the digits and protected throughout the case. Using fluoroscopy, the bony connection between the distal phalanges of digits three and four was identified. A small osteotome was used to separate this connection. The hexagonal dorsal skin flaps at the web space were brought between the digits and sutured volarly with 6-0 Vicryl suture. Skin on the ulnar aspect of digit three was amenable to primary closure, but skin on the radial aspect of digit four was not. A 2.5 × 2.5 cm piece of Hyalomatrix synthetic graft was trimmed, placed, and sutured over the skin deficit on the radial aspect of digit four using 6-0 Vicryl suture. Attention was then turned to the right hand. The same steps and techniques described for the left hand were performed on digits three and four of the right hand. However, there was no osseous connection between digits three and four and the connection between digits four and five was addressed during the first stage of the procedure. A 2.5 × 2.5 cm piece of Hyalomatrix was again utilized for skin deficit coverage involving the radial aspect of digit four. At the end of each procedure, the operative digits demonstrated good capillary refill and both hands were immobilized in mitten casts. The patient’s hands were evaluated in the clinic at two weeks and nine weeks postoperatively. Brisk capillary refill and intact sensation were noted in the operative digits at both follow-up appointments. Minimal web creep involving the fourth web space of the right hand was observed at the second post-operative visit (Fig. 3). No significant adverse complications were encountered, including infection, ischemia, or graft loss.

Figure 3: Clinical photographs of the patient’s right and left hands, respectively, 9 weeks from the date of surgery, demonstrating release of prior complex and complete syndactyly with minimal scarring. Previous skin deficits involving the radial aspects of digit four in bilateral hands necessitating Hyalomatrix coverage have fully healed with a small amount of creep involving the fourth web space of the right hand.
As demonstrated above, multiple techniques are available for the treatment of congenital syndactyly and more novel treatment options continue to evolve [2,3,5,20]. Our case supports the growing evidence for the use of Hyalomatrix as an alternative to traditional skin grafting for skin deficits not amenable to primary closure. In a study by Bohn and colleagues [21], the utility of full-thickness skin grafts versus a HA skin substitute for web space coverage in 18 patients was explored. For each patient, one-half of the web space skin deficit was covered by a full-thickness skin graft while the other was covered with an HA synthetic graft. The study demonstrated no significant differences in scar formation at the graft sites, but, interestingly, showed HA graft placement required less surgical time than a traditional skin graft. This decreased surgical time was offset by prolonged open-wound time postoperatively and increased wound care needs. Nonetheless, decreased surgical time is beneficial for both surgeons and patients in that it offers improved efficiency for the surgeon while minimizing anesthesia exposure for the patient. Typically, those who are surgically treated for congenital syndactyly are young pediatric patients ages 1–2 years old or younger. Current literature has shown that prolonged and frequent general anesthesia exposure can lead to negative neurocognitive and neurodevelopmental effects in pediatric patients [19]. Thus, surgeons who treat pediatric patients have a duty of care to limit general anesthesia exposure when possible while not compromising high-quality care. Our patient required staging of his syndactyly reconstruction to decrease the risk of flap necrosis and vascular injury. This required two sessions in the operating room and two inductions with general anesthesia. In comparison to the time necessary to harvest skin grafts, our use of Hyalomatrix for our patient decreased his general anesthesia exposure.
Our case provides further evidence to the limited literature that Hyalomatrix graft utilization can be successful in the treatment of complex, complete syndactyly reconstruction. In addition, our case highlights not only the technical benefits of synthetic graft use to surgeons but also the intangible benefit of decreased general anesthesia exposure time to pediatric patients. There is significant evidence that Hyalomatrix is a safe and effective option for skin deficit coverage with favorable outcomes regarding scar appearance, skin pigmentation, and function. It is important that surgeons be aware of and understand how to execute both traditional methods of coverage for skin deficits when performing syndactyly reconstruction, but also alternatives such as synthetic grafts when primary closure or dorsal flap advancement are not feasible.
Our report is a significant contribution to the current orthopedic literature as it reinforces evidence that Hyalomatrix, a HA synthetic matrix used for wound coverage, is an effective and safe skin substitute in infants who undergo upper extremity syndactyly reconstruction. In addition, compared to traditional skin grafting techniques for skin deficit coverage which can result in unappealing scarring, web creep, hyperpigmentation, and poor donor or recipient site healing, our report demonstrates the use of Hyalomatrix results in minimal scarring and web creep, no limitation of digit function, and complete resolution of skin deficits via new dermal tissue generation and spontaneous epithelization.
References
- 1. Jordan D, Hindocha S, Dhital M, Saleh M, Khan W. The epidemiology, genetics and future management of syndactyly. Open Orthop J 2012;6:14-27. [Google Scholar] [PubMed]
- 2. Kozin SH. Syndactyly. J Am Soc Surg Hand 2001;1:1-13. [Google Scholar] [PubMed]
- 3. Dao KD, Shin AY, Billings A, Oberg KC, Wood VE. Surgical treatment of congenital syndactyly of the hand. J Am Acad Orthop Surg 2004;12:39-48. [Google Scholar] [PubMed]
- 4. Braun TL, Trost JG, Pederson WC. Syndactyly release. Semin Plast Surg 2016;30:162-70. [Google Scholar] [PubMed]
- 5. Sullivan MA, Adkinson JM. A systematic review and comparison of outcomes following simple syndactyly reconstruction with skin grafts or a dorsal metacarpal advancement flap. J Hand Surg 2017;42:34-40.e6. [Google Scholar] [PubMed]
- 6. Gowrie S, Omosebi O, Veith P, Agarwal N, Shah S, Montalbano M, et al. Stuck together: A systematic review of hand syndactyly. Cureus 2025;17:e81943. [Google Scholar] [PubMed]
- 7. Ferrari BR, Werker PM. A cross-sectional study of long-term satisfaction after surgery for congenital syndactyly: Does skin grafting influence satisfaction? J Hand Surg Eur Vol 2019;44:296-303. [Google Scholar] [PubMed]
- 8. Jung JJ, Woo AS, Borschel GH. The use of Integra® bilaminar dermal regeneration template in apert syndactyly reconstruction: A novel alternative to simplify care and improve outcomes. J Plast Reconstr Aesthet Surg 2012;65:118-21. [Google Scholar] [PubMed]
- 9. Landi A, Garagnani L, Leti Acciaro A, Lando M, Ozben H, Gagliano MC. Hyaluronic acid scaffold for skin defects in congenital syndactyly release surgery: A novel technique based on the regenerative model. J Hand Surg Eur Vol 2014;39:994-1000. [Google Scholar] [PubMed]
- 10. Wall LB, Velicki K, Roberts S, Goldfarb CA. Outcomes of pediatric syndactyly repair using synthetic dermal substitute. J Hand Surg 2020;45:773.e1-6. [Google Scholar] [PubMed]
- 11. Fangxing A, Gongchi L, Zhiwei L, Hanling L, Haiding Z, Yuxiong W, et al. Syndactyly release with the use of the PelnacTM artificial dermal substitute without skin grafting. J Plast Reconstr Aesthet Surg 2023;84:115-20. [Google Scholar] [PubMed]
- 12. Simman R. The Role of an Esterified hyaluronic acid matrix in wound healing, a case series. J Am Coll Clin Wound Spec 2018;8:10-11. [Google Scholar] [PubMed]
- 13. Iaconisi GN, Lunetti P, Gallo N, Cappello AR, Fiermonte G, Dolce V, et al. Hyaluronic acid: A powerful biomolecule with wide-ranging applications-a comprehensive review. Int J Mol Sci 2023;24:10296. [Google Scholar] [PubMed]
- 14. Onesti MG, Carella S, Maruccia M, Ciotti M, Scuderi N. The use of hyalomatrix PA in the treatment of extravasation affecting premature neonates. Plast Reconstr Surg 2012;129:219e-21. [Google Scholar] [PubMed]
- 15. Xu DH, Forg P. Application of hyaluronic acid matrix membrane in wound healing. The Proceedings of the Annual Meeting of the Podiatry Institute. Chapter 7. 2019: 29-32. AccessedSept12,2025. https://www.podiatryinstitute.com/pdfs/Update_2019/chapter_07.pdf [Google Scholar] [PubMed]
- 16. Simman R, Mari W, Younes S, Wilson M. Use of hyaluronic acid-based biological bilaminar matrix in wound bed preparation: A case series. Eplasty 2018;18:e10. [Google Scholar] [PubMed]
- 17. Whyte GP, Bizzoco L, Gobbi A. One-step cartilage repair of full-thickness knee chondral lesions using a hyaluronic acid-based scaffold embedded with bone marrow aspirate concentrate: Long-term outcomes after mean follow-up duration of 14 years. Am J Sports Med 2024;52:3561-8. [Google Scholar] [PubMed]
- 18. Smith PJ, Harrison SH. The “seagull” flap for syndactyly. Br J Plast Surg 1982;35:390-3. [Google Scholar] [PubMed]
- 19. Arane K, Li D, Baxter T, Gandhi B, Positano K, Howlett M, et al. Reducing general anesthesia for lumbar punctures in pediatric patients with leukemia and lymphoma, a quality improvement project. Pediatr Blood Cancer 2025;72:e31843. [Google Scholar] [PubMed]
- 20. Schirlo JM, Saad Cleto A, Beltrame D, Beltrame M, Scortegagna T, Marinelli Martins C. Comparison between surgical techniques for correction of congenital syndactyly: A systematic review and meta analysis. HAND (N Y) 2025;20:523-32. [Google Scholar] [PubMed]
- 21. Bohn DC, Price JN, Novotny SA, Sylvanus TS, Van Heest AE. Syndactyly release with skin graft or skin graft substitute: A within-subject controlled trial. J Hand Surg Eur Vol 2025;50:1339-47. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2022 Localized Pigmented Villonodular Synovitis of the Bilateral Knee: A Case Report
July 10, 2022 Localized Pigmented Villonodular Synovitis of the Bilateral Knee: A Case Report March 1, 2025 Hybrid External Fixation as A Comprehensive, Safe, and Effective Solution for Periarticular Tibial Fracture with Soft Tissue Compromise
March 1, 2025 Hybrid External Fixation as A Comprehensive, Safe, and Effective Solution for Periarticular Tibial Fracture with Soft Tissue Compromise April 7, 2014 Malakoplakia of Proximal Tibia- A Case Report
April 7, 2014 Malakoplakia of Proximal Tibia- A Case Report August 10, 2020 Pseudo-winging of Scapula due to Ventral Scapular Osteochondroma: A Case Report and Literature Review
August 10, 2020 Pseudo-winging of Scapula due to Ventral Scapular Osteochondroma: A Case Report and Literature Review