
Ultrasound-guided caudal epidural steroid injection offers greater accuracy and early functional benefit, while the landmark-guided technique remains practical and effective in low-resource settings; both techniques are safe and effective in the management of chronic lower backache.
Dr. Harsh Chauhan, Department of Orthopaedics, Government Medical College and Hospital, Jammu, Jammu and Kashmir. E-mail: chauhanharsh2@gmail.com
Abstract
Introduction: Caudal epidural steroid injection (CESI) is a commonly performed interventional procedure for the management of chronic lower backache. The conventional landmark-guided (LG) technique is widely practiced, particularly in resource-limited settings, while ultrasound guidance is increasingly used to improve procedural accuracy and safety.
Objectives: The objective of the study was to compare the clinical efficacy, safety, and need for repeat intervention between LG and ultrasound-guided (USG) CESI in adults with chronic low backache.
Materials and Methods: A prospective randomized controlled study was conducted on 200 patients with chronic low backache, equally divided into two groups: Group L (LG CESI) and Group U (USG CESI). Pain intensity, functional disability, and straight leg raise test (SLRT) were assessed at baseline, 1 week, 1 month, and 2 months after injection using the visual analog scale (VAS), Oswestry disability index (ODI), and SLRT. The requirement for repeat injections and procedure-related complications was also recorded.
Results: Both groups demonstrated significant improvement in VAS and ODI scores following CESI. The USG group showed better improvement in right-sided SLRT at 1 week (P = 0.003) and required fewer repeat injections compared to the LG group (8% vs. 11%, P = 0.029). No complications were observed in either group.
Conclusion: Both LG and USG CESI are safe and effective techniques for the management of chronic low backache. Ultrasound guidance provides early functional benefits and reduces the need for repeat injections, while the LG technique remains a practical alternative in resource-constrained settings.
Keywords: Caudal epidural steroid injection, chronic low back pain, ultrasound guidance, landmark technique, visual analog scale, Oswestry disability index.
Chronic low back pain is a prevalent musculoskeletal disorder worldwide, affecting nearly 80% of adults at some point during their lifetime and significantly impairing quality of life and work productivity. In India, the reported prevalence ranges from 6.2% to 92%. Caudal epidural steroid injection (CESI) is a widely accepted interventional modality for managing both axial and radicular low back pain [1,2]. Although CESI is commonly practiced, there is a relative lack of well-designed randomized controlled trials evaluating its efficacy in chronic low backache with or without radiculopathy [3]. Conventionally, landmark-guided (LG) CESI has been routinely performed, particularly in outpatient and resource-limited settings; however, anatomical variations may affect accuracy. Real-time ultrasound guidance allows visualization of sacral anatomy, potentially improving needle placement accuracy and procedural safety [4]. The posterior approach through the sacral hiatus provides reliable access to the epidural space, and detailed knowledge of sacral hiatus anatomy is essential for accurate CESI administration [5].
Study design
This study was conducted as a prospective randomized controlled trial in the Department of Orthopaedics, Government Medical College, Jammu, from May 2024 to April 2025, and was reported in accordance with CONSORT guidelines. [Fig. 1]
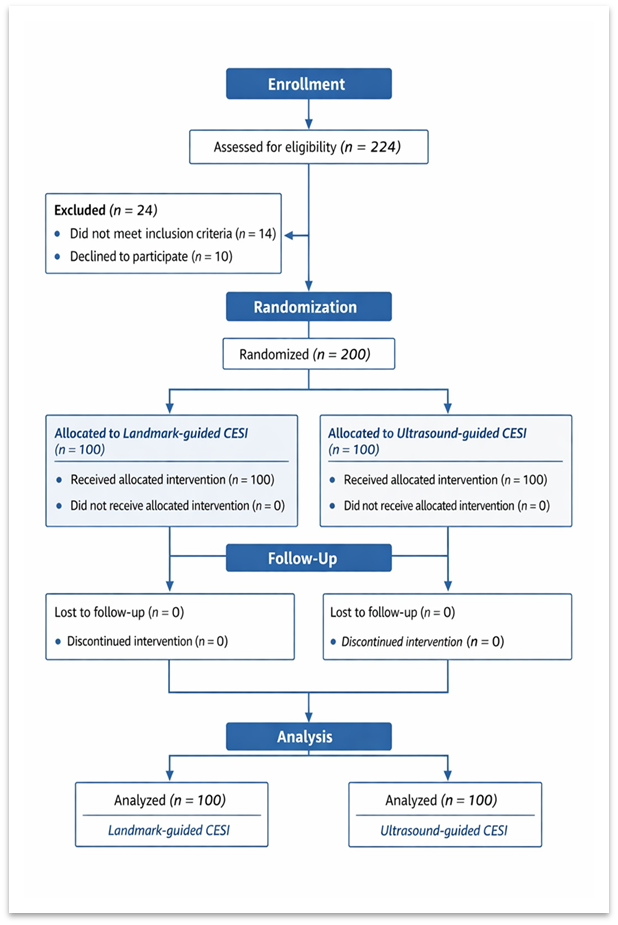
Figure 1: CONSORT flow diagram of study participants
Participants
A total of 200 adult patients diagnosed with chronic low backache, with or without radiculopathy, were enrolled after meeting inclusion and exclusion criteria and providing written informed consent.
Inclusion criteria
- Age ≥18 years
- Chronic low backache with or without radiculopathy
- Failure of conservative management
- Willingness to participate.
Exclusion criteria
- Coagulopathy
- Local or systemic infection
- Pregnancy
- Severe systemic illness
- Cauda equina syndrome.
Sample size
The sample size was 200 participants.
Sample size justification
Based on reported prevalence of chronic low backache in the Indian population and assuming a minimum clinically important difference of 0.5 units in Visual Analog Scale (VAS) score between groups, with an estimated standard deviation of 1.2, alpha error of 0.05, and power of 80%, the minimum required sample size was calculated as 92 patients per group. Allowing for potential attrition, 100 patients were enrolled in each group.
Randomization and allocation
Patients were randomized into two groups in a 1:1 ratio using simple random allocation before intervention:
- Group L: LG CESI (n = 100)
- Group U: Ultrasound-guided (USG) CESI (n = 100).
Blinding
Blinding of the operator was not feasible due to the nature of the intervention. Outcome assessments were performed using standardized and validated clinical assessment tools.
Intervention technique
LG CESI
Patients were positioned prone or in the lateral position when prone positioning was not feasible. A line connecting the posterosuperior iliac crests was identified, and the sacral cornua were palpated to locate the sacral hiatus. A 22- or 23-gauge spinal needle was introduced at approximately 45° to the sacrum [6,7]. Loss of resistance indicated penetration of the sacrococcygeal ligament. Correct epidural placement was confirmed using the whoosh test [8].
USG CESI
Using a 7–13 MHz linear probe, the sacral cornua and sacral hiatus were identified as hyperechoic and hypoechoic structures, respectively [9]. The probe was rotated longitudinally to visualize the sacrococcygeal ligament. The needle was advanced using an in-plane technique under real-time ultrasound guidance [10]. [Fig. 2 and 3].
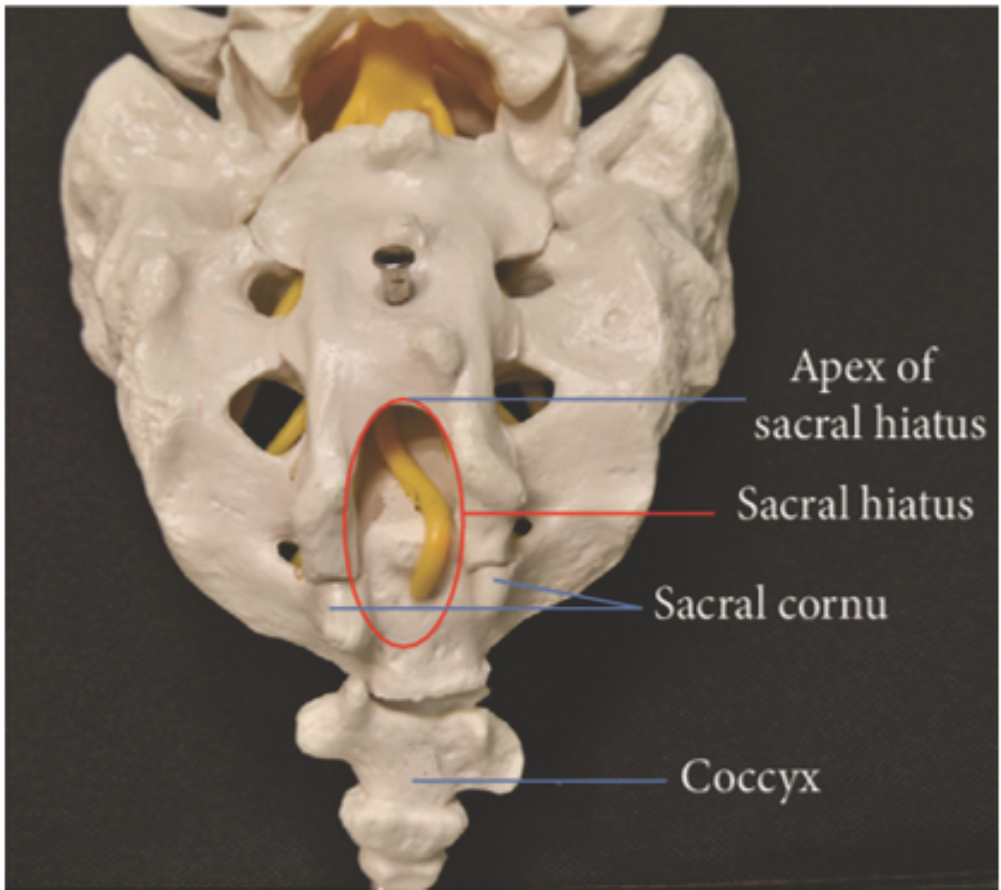
Figure 2: Sacrum- posterior view.
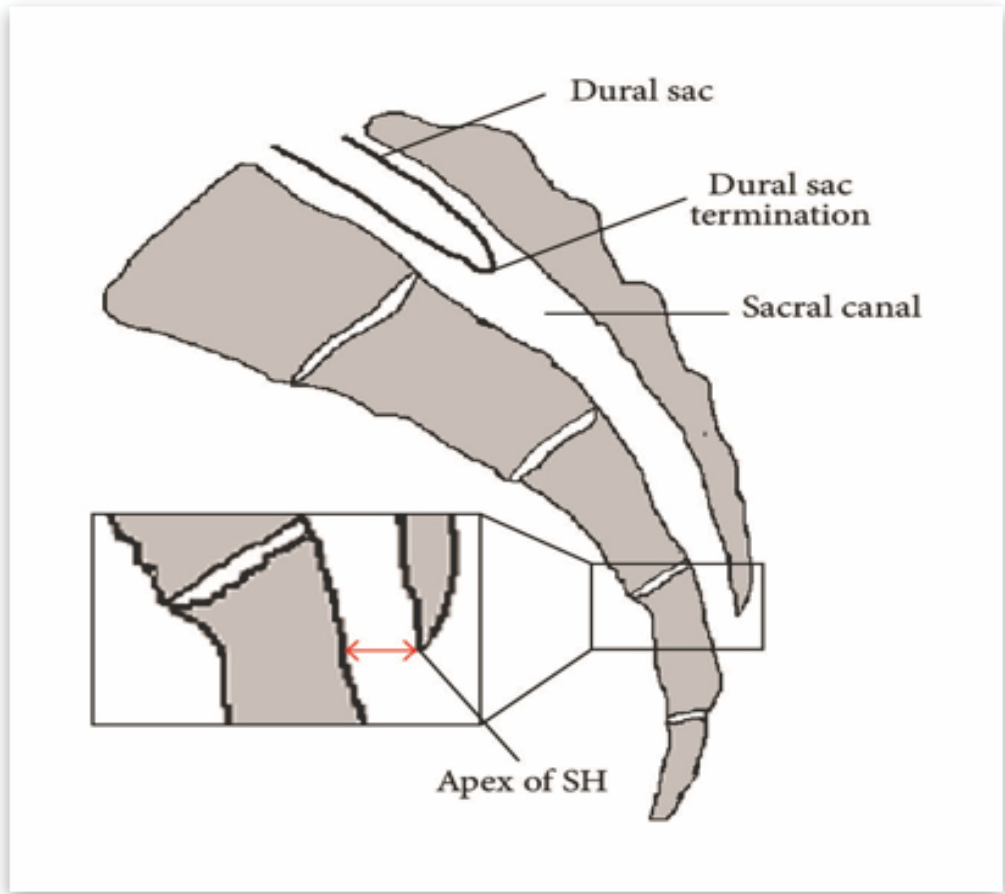
Figure 3 : Sacrum- sagittal view.
Drug administration
All patients received 80 mg methylprednisolone diluted in 10 mL normal saline.
Outcome measures
Primary outcome was pain relief assessed by VAS. Secondary outcomes included Oswestry disability index (ODI), straight leg raise test (SLRT), requirement for repeat CESI, and procedure-related complications. Assessments were performed at baseline, 1 week, 1 month, and 2 months.
Statistical analysis
Continuous variables were analyzed using Student’s t-test and categorical variables using Chi-square test. A P < 0.05 was considered statistically significant.
Ethical considerations
The study was approved by the Institutional Ethics Committee of Government Medical College, Jammu (IEC/GMCJ/2024/1930). Written informed consent was obtained from all participants.
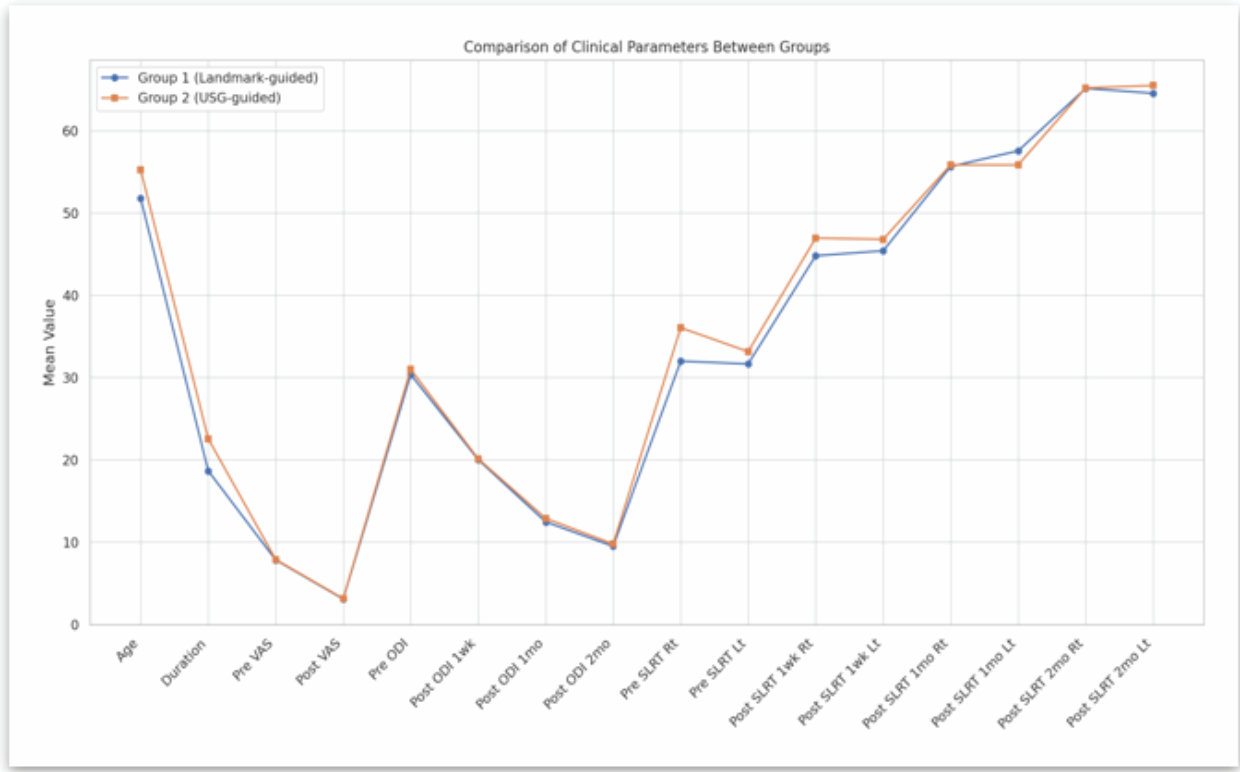
Figure 4 : Comparison of clinical parameters between two groups.
Baseline characteristics (Fig. 4)
- Mean age: Group L: 51.77 ± 16.07; Group U: 55.24 ± 13.17 (P = 0.097)
- Mean duration of symptoms: Group U had longer symptoms (P = 0.010)
- Weight: Higher in Group U (P = 0.036).
Baseline demographic characteristics were comparable between the two groups.
Pain and disability
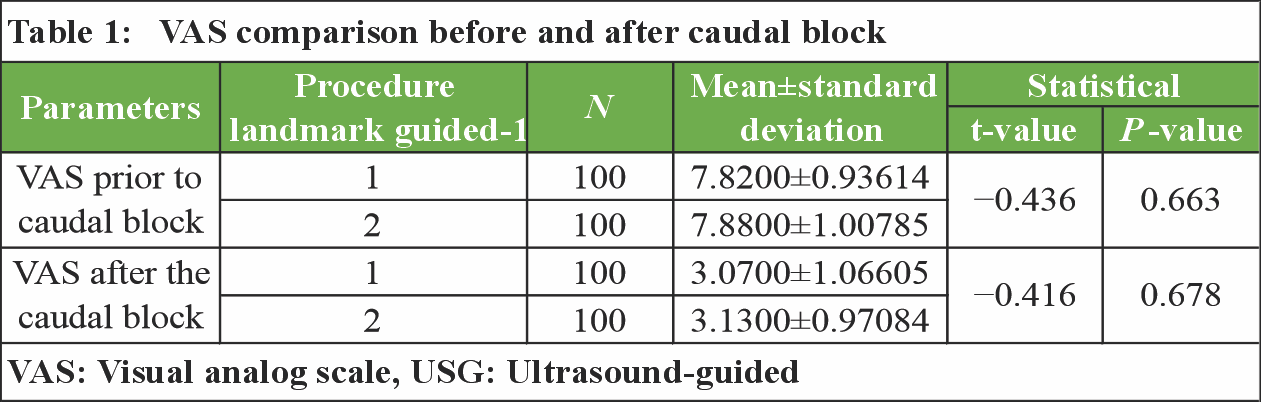
VAS decreased significantly in both groups post-CESI (Group L: 7.82→3.07; Group U: 7.88→3.13; P = 0.678). Both groups showed progressive improvement and significant reduction in VAS and ODI scores over time, without any statistically significant intergroup difference. [Table 1] [Fig. 5].
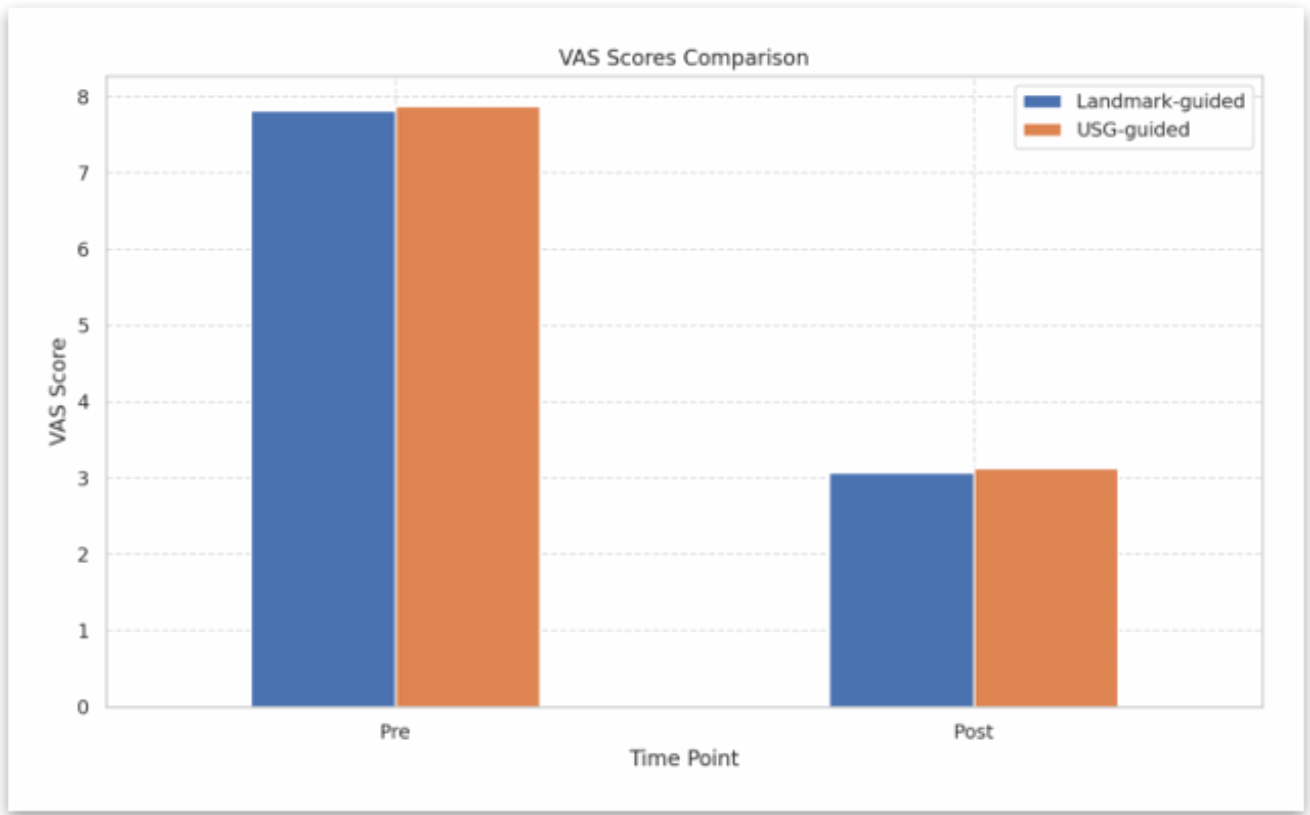
Figure 5: Visual Analog Scale comparison pre and post-injection.
 SLRT
SLRT
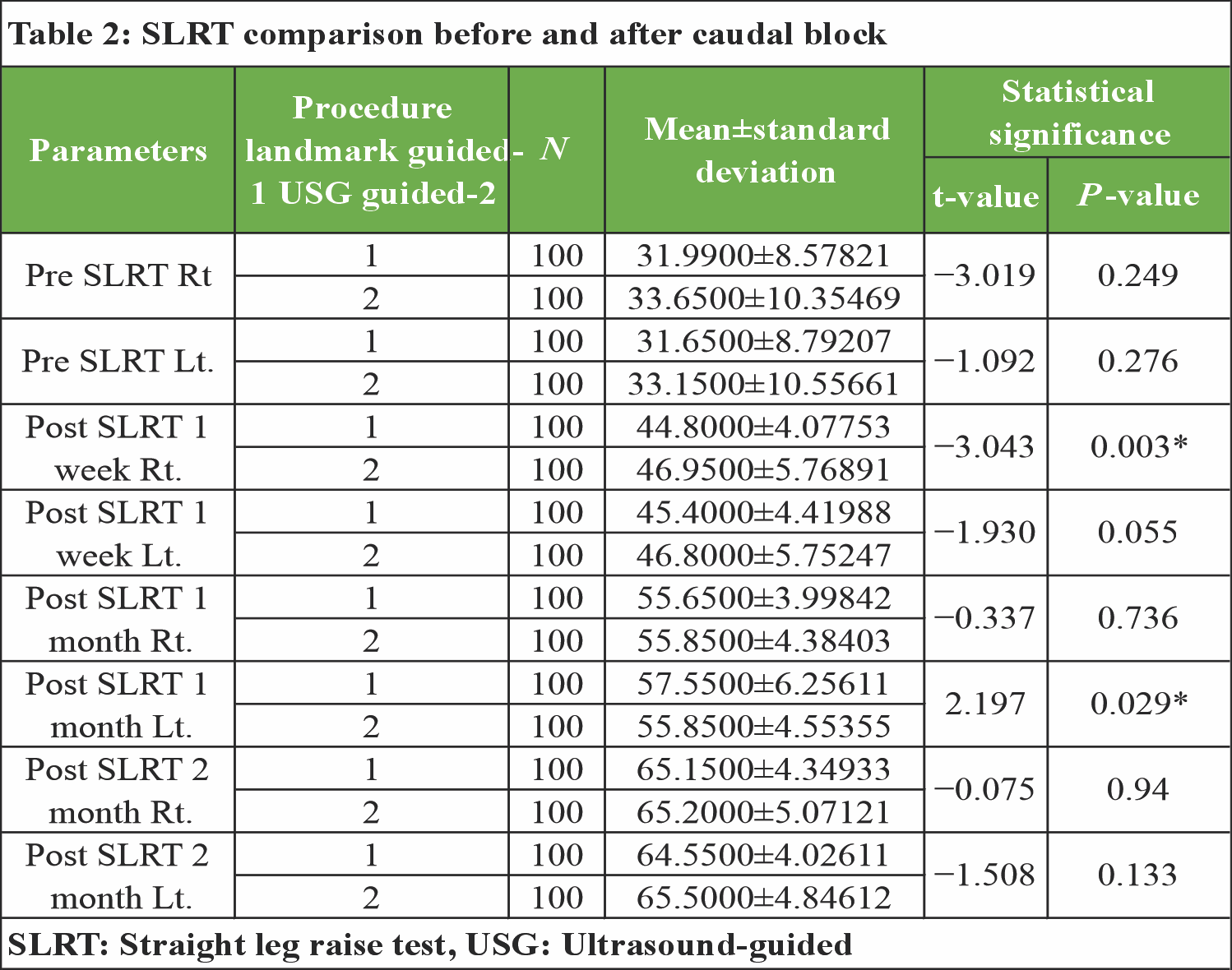
The USG group demonstrated better right-sided SLRT improvement at 1 week (P = 0.003), while the LG group showed better left-sided SLRT at 1 month (P = 0.029). [Table 2]
 Repeat injection requirement
Repeat injection requirement
Lower in Group U (8%) versus Group L (11%) (P = 0.029). [Table 3].
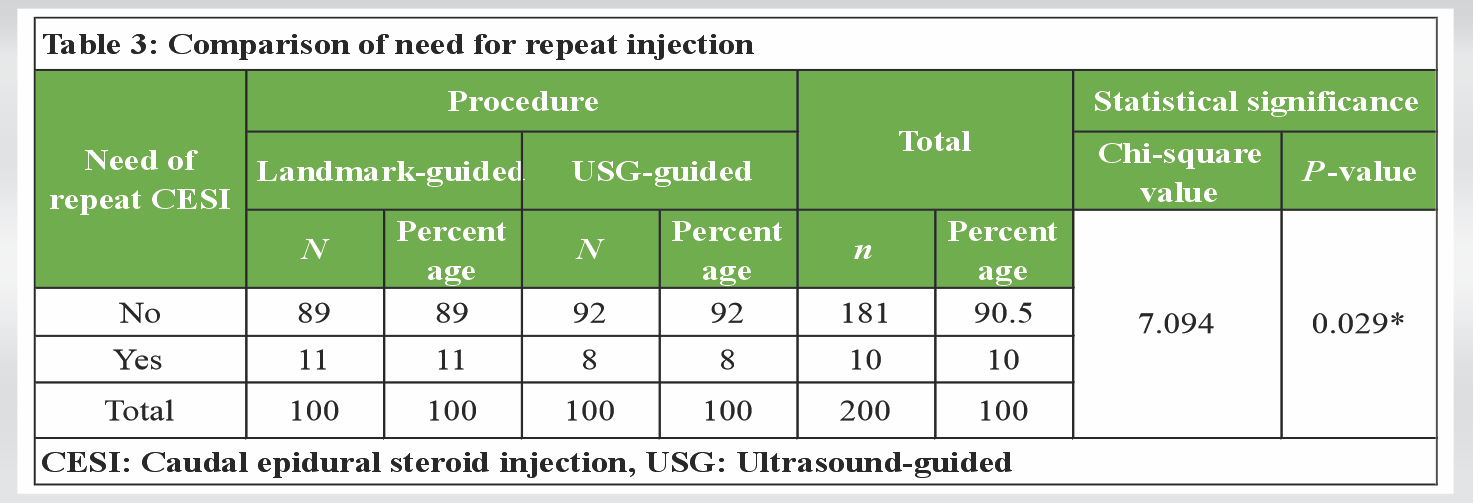
The requirement for repeat injections was significantly lower in the USG group.
Complications
No procedure-related complications were observed in either group.
Chronic lower backache remains a major contributor to disability and loss of productivity in the Indian population. CESI continues to occupy an important role as a minimally invasive intervention bridging prolonged conservative therapy and surgical management [11,12,13]. The present study demonstrates that both LG and USG CESI are effective in reducing pain intensity and improving functional outcomes, while also revealing technique-specific differences that become evident when interpreted alongside recent Indian literature [14,15].
Procedural accuracy and anatomical considerations
The reduced requirement for repeat injections and earlier functional improvement observed in the USG group are consistent with higher procedural accuracy achieved through real-time visualization of sacral anatomy. Anatomical variability of the sacral hiatus has been identified as a key factor influencing procedural success, explaining limitations inherent to blind landmark-based approaches.
Functional outcomes
Although both groups demonstrated significant improvement in VAS and ODI scores, the earlier functional recovery observed in the USG group suggests more reliable epidural drug deposition.
Safety profile and practical considerations
The absence of complications in both groups highlights the safety of CESI when performed with proper technique. Ultrasound guidance offers the additional advantage of avoiding radiation exposure, making it suitable for repeated interventions and special populations.
Limitations
The follow-up period was limited to 2 months, restricting assessment of long-term outcomes and recurrence. Operator blinding was not feasible due to the nature of the intervention. Functional outcomes were assessed clinically without imaging confirmation of epidural spread. As a single-center study, generalizability may be limited.
As per the prospective randomized trial results, both LG and USG CESI are safe, effective, and well-tolerated options for patients suffering from chronic low backache with or without radiculopathy. Although pain and disability outcomes were comparable, ultrasound guidance demonstrated advantages in early functional recovery and reduced need for repeat injections. Nevertheless, LG CESI remains a practical and effective approach in outpatient and resource-limited settings.
Both ultrasound-guided and landmark-guided CESI are comparable in pain relief and safety. Landmark guidance remains feasible in low-resource settings, while ultrasound guidance offers accuracy-driven benefits where available.
References
- 1. Ackerman WE 3rd, Ahmad M. The efficacy of lumbar epidural steroid injections in patients with lumbar disc herniations. Anesth Analg 2007;104:1217-22. [Google Scholar] [PubMed]
- 2. Murakibhavi VG, Khemka AG. Caudal epidural steroid injection: A randomized controlled trial. Evid Based Spine Care J 2011;2:19-26. [Google Scholar] [PubMed]
- 3. Conn A, Buenaventura RM, Datta S, Abdi S, Diwan S. Systematic review of caudal epidural injections in the management of chronic low back pain. Pain Physician 2009;12:109-35. [Google Scholar] [PubMed]
- 4. Singh V, Manchikanti L. Role of caudal epidural injections in the management of chronic low back pain. Pain Physician 2002;5:133-48. [Google Scholar] [PubMed]
- 5. Aggarwal A, Kaur H, Batra YK, Aggarwal AK, Rajeev S, Sahni D. Anatomic consideration of caudal epidural space: A cadaver study. Clin Anat 2009;22:730-7. [Google Scholar] [PubMed]
- 6. Senoglu N, Senoglu M, Oksuz H, Gumusalan Y, Yuksel KZ, Zencirci B, et al. Landmarks of the sacral hiatus for caudal epidural block: An anatomical study. Br J Anaesth 2005;95:692-5. [Google Scholar] [PubMed]
- 7. Kao SC, Lin CS. Caudal epidural block: An updated review of anatomy and techniques. Biomed Res Int 2017;2017:9217145. [Google Scholar] [PubMed]
- 8. Lewis MP, Thomas P, Wilson LF, Mulholland RC. The ‘whoosh’ test. A clinical test to confirm correct needle placement in caudal epidural injections. Anaesthesia 1992;47:57-8. [Google Scholar] [PubMed]
- 9. Klocke R, Jenkinson T, Glew D. Sonographic evaluation of caudal epidural space. Reg Anesth Pain Med 2003;28:340-5. [Google Scholar] [PubMed]
- 10. Park GY, Kwon DR, Cho HK. Anatomic differences in the sacral hiatus during caudal epidural injection using ultrasound guidance. J Ultrasound Med 2015;34:2143-8. [Google Scholar] [PubMed]
- 11. Dernek B, Aydoğmuş S, Ulusoy I, Duymuş TM, Ersoy S, Kesiktaş FN, et al. Caudal epidural steroid injection for chronic low back pain: A prospective analysis of 107 patients. J Back Musculoskelet Rehabil 2022;35:135-9. [Google Scholar] [PubMed]
- 12. Goel S, Mitra S, Singh J, Jindal S, Upadhyay P, Jindal R. Comparison of ultrasound and fluoroscopy-guided caudal epidural block in low back pain with radiculopathy: A randomized controlled study. J Anaesthesiol Clin Pharmacol 2024;41:106-11. [Google Scholar] [PubMed]
- 13. Lee DY, Park Y, Song JH, Ahn J, Cho KH, Kim S. Ultrasound versus fluoroscopy-guided caudal epidural steroid injection for lumbar radicular pain: A comparative study. Medicina (Kaunas) 2024;60:809. [Google Scholar] [PubMed]
- 14. Nagpal AS, Vu TN, Gill B, Conger A, McCormick ZL, Duszynski B, et al. Systematic review of the effectiveness of caudal epidural steroid injections in the treatment of chronic low back or radicular pain. Interv Pain Med 2022;1:100149. [Google Scholar] [PubMed]
- 15. Chauhan AK, Bhatia R, Agrawal S. Lumbar epidural depth using transverse ultrasound scan and its correlation with loss of resistance technique: A prospective observational study in Indian population. Saudi J Anaesth 2018;12:279-82. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Effectiveness of Epidural Methylprednisolone Injection in Management of Lumbar Prolapsed Intervertebral Disc: A Comparison of Caudal, Transforaminal and Interlaminar Routes
October 1, 2025 Effectiveness of Epidural Methylprednisolone Injection in Management of Lumbar Prolapsed Intervertebral Disc: A Comparison of Caudal, Transforaminal and Interlaminar Routes July 1, 2026 Efficacy of Intra-articular Growth Factor Concentrate in Knee Osteoarthritis: A Randomized Controlled Trial
July 1, 2026 Efficacy of Intra-articular Growth Factor Concentrate in Knee Osteoarthritis: A Randomized Controlled Trial June 1, 2026 Predictive Factors for Unfavorable Outcomes in Degenerative Lumbar Spondylolisthesis Surgery
June 1, 2026 Predictive Factors for Unfavorable Outcomes in Degenerative Lumbar Spondylolisthesis Surgery March 1, 2026 Clinical Outcome of Arthroscopic Anterior Cruciate Ligament Reconstruction with Simultaneous Meniscus Repair
March 1, 2026 Clinical Outcome of Arthroscopic Anterior Cruciate Ligament Reconstruction with Simultaneous Meniscus Repair