
Mycobacterium intracellulare can be a difficult organism to treat in prosthetic joint infection. Extended antibiotic spacer usage can be a useful tool in infection eradication before definitive management.
Dr. Jayanth Kumar, Department of Orthopaedic Surgery and Rehabilitation, College of Medicine, University of Florida, Jacksonville, Florida, United States. E-mail: jayanth.kumar@jax.ufl.edu
Abstract
Introduction: Mycobacterium infections are a rare but devastating cause of prosthetic joint infection (PJI). Most cases of non-tuberculous mycobacteria infections occur in immunocompromised hosts, a population increasing with the use of immunosuppressive medications such as biologics. We describe a unique case of a healthy patient with an infected total knee arthroplasty (TKA) found to be colonized by the rare Mycobacterium avium intracellulare, who ultimately had an antibiotic spacer retained for 18 months before second-stage revision surgery.
Case Report: The patient was an immunocompetent 41-year-old female with an infected TKA with the rare Mycobacterium avium intracellulare infection. She ultimately needed a two-stage revision surgery, where she had a retained antibiotic spacer for an extended period of 18 months before reimplantation surgery.
Conclusion: Mycobacterium intracellulare is a very rare organism seen with infection of total joint arthroplasty. Careful workup and infection management are critical to providing the best patient results. Antibiotic spacers are very useful in managing infected total joint arthroplasties. Ultimately, prolonged antibiotic spacer usage can be an effective strategy for orthopedic surgeons to address rare organisms with infected total joint arthroplasties.
Keywords: Prosthetic joint infection, mycobacterium, retained antibiotic spacer.
Prosthetic joint infections (PJIs) are a rare but dreaded complication of total joint arthroplasty. The gold standard of treatment remains a two-stage exchange with interval placement of an antibiotic spacer. Most PJI cases are caused by Gram-positive cocci, such as coagulase-negative Staphylococcus species (60%) and other gram-positive cocci, such as Staphylococcus aureus. However, <2% of all PJI cases are caused by Mycobacterium [1]. There is limited evidence on both the diagnosis and treatment of PJIs caused by nontuberculous mycobacteria. The bulk of the scientific literature regarding this specific problem consists of case reports and case series. The case presented demonstrates the difficulty in diagnosing mycobacterial infection, as well as the safe and effective prolonged use of antibiotics and retention of an antibiotic spacer for a period of 18 months. The use of an articulating spacer allowed our patient to maintain knee range of motion, which facilitated delayed reimplantation once clinical and laboratory evaluation suggested eradication of the infection.
The patient was an immunocompetent 41-year-old female who presented to our clinic with a painful and unstable right knee prosthesis, with the index procedure performed approximately 5 years prior at an outside institution. The patient was a poor historian, and the indication for the index procedure was not clear, and operative reports were not available for review. Clinical examination revealed a right knee with varus deformity, coronal plane instability, and a moderate joint effusion. Imaging demonstrated femoral component loosening with osteolysis of the lateral distal femoral condyle (Fig. 1). An infectious workup was initiated, and inflammatory markers were within normal limits, with a C-reactive protein of 3 mg/L and erythrocyte sedimentation rate of 8 mm/h. As surgical intervention was planned to address a loose femoral implant, a joint aspiration was performed. Initial right knee arthrocentesis revealed a synovial white blood cell count (WBC) of 1,870 cells per µL, 60% polymorphonuclear (PMN) cells, and negative aerobic and anaerobic cultures. Evaluation of the sample for acid-fast bacilli (AFB) was not performed. The patient was directed toward anticipated surgical intervention – revision TKA versus antibiotic spacer. Surgical scheduling was prolonged for several reasons: (1) poor patient follow-through with obtaining an magnetic resonance imaging to evaluate the integrity of the medial collateral ligament; (2) the patient took a significant period of time to achieve any reduction in smoking; and (3) difficulty obtaining primary care clearance. Due to this prolonged period before scheduling and persistent clinical concern for PJI, a repeat arthrocentesis was performed. This aspiration yielded a synovial WBC count of 1,822 cells/µL and 37% PMNs, yet cultures were positive for Mycobacterium intracellulare after 17 days. Given the low PMNs yet positive mycobacterial culture in an otherwise immunocompetent host, this result was initially considered a potential false positive due to suspected sample contamination. To confirm or refute this discrepancy, a repeat arthrocentesis was performed before surgery. The final pre-operative sample demonstrated a WBC of 2,397 cells/µL with 79% PMNs, negative aerobic and anaerobic cultures, and again positive AFB culture for Mycobacterium intracellulare. A diagnosis of PJI was made, and a two-stage exchange consisting of femoral and tibial component removal with interval placement of an articulating antibiotic spacer was planned (Fig. 2).
Intraoperative course
Intraoperative cultures once again grew Mycobacterium intracellulare, and infectious disease specialists recommended an oral antibiotic regimen of azithromycin 500 mg daily, rifabutin 300 mg daily, and ethambutol 1600 mg daily for 1 year. The patient was discharged on postoperative day 5 without complications. Post-operative instructions included non-weight-bearing on the right lower extremity, while allowing right knee range-of-motion exercises. The patient was consistent with orthopedic and infectious disease follow-up. Throughout her postoperative course, she reported significant improvement in knee pain following implant removal and antibiotic spacer placement. However, she experienced significant antibiotic-related adverse reactions, including skin blistering, vaginal fungal infections, sinus infections, and teeth discoloration. Consequently, at 3 months postoperatively, the infectious disease team discontinued rifabutin and initiated rifampin. It was also recommended that the duration of antibiotic treatment be increased to 18 months. At 4 months postoperatively, the patient experienced adverse reactions to rifampin, which was discontinued, and levofloxacin was initiated. Levofloxacin was poorly tolerated, and the patient was transitioned back to rifampin. At 18 months following implant removal and antibiotic spacer placement, the patient underwent a 2-week antibiotic holiday, followed by a right knee aspiration. This resulted in a synovial WBC of 616 cells/µL and 42% PMNs with negative cultures. Right knee range of motion consisted of full extension and 100° of flexion, and her clinical exam did not reveal any wounds or soft-tissue concerns. Based on these findings, the decision was made to proceed with revision right total knee arthroplasty (TKA).
Reimplantation procedure
A standard medial parapatellar approach was used, and the tibial and femoral antibiotic spacers were removed using osteotomes without any bone loss. The dowels were removed from the medullary canals of both the femur and tibia, which were then debrided and irrigated. Tibial reconstruction was performed using a trabecular metal cone, a splined, stemmed tibial implant, and medial and lateral tibial augments. Femoral reconstruction was performed using a trabecular metal cone, a splined, stemmed femoral component, and distal medial and lateral augments (Fig. 3).
Intraoperative cultures from three separate specimens were positive for Corynebacterium jeikeium. The patient was discharged on rifampin 600 mg daily, ethambutol 1600 mg daily, and azithromycin 500 mg daily. In the setting of prior PJI, the decision was made to treat the Corynebacterium with an additional 4 weeks of linezolid. This was poorly tolerated, and the patient was transitioned to minocycline 100 mg twice daily for 6 months. At the latest follow-up, 1 year postoperatively from revision TKA, she reported minimal pain, a fully healed incision, independent ambulation, and a full range of motion from 0° extension to 120° flexion. Radiographic imaging at the latest follow-up shows intact hardware without acute signs of loosening, subsidence, or failure. The patient was very satisfied with her progress.
PJI is an increasingly common reason for revision arthroplasty following joint replacement and is associated with increased patient morbidity, mortality, and healthcare costs. PJI is a dreaded complication for both the patient and the arthroplasty surgeon, and current data show that it will only become more common, with estimates of 10,000 cases per year by 2030 [2]. The current gold-standard treatment strategy in the United States is a two-stage revision, which involves explantation of hardware and placement of an antibiotic spacer, followed by a prolonged period – typically 6 weeks – of intravenous antibiotics before removal of the spacer and placement of definitive components. The decision to proceed with re-implantation was based on negative cultures, reassuring infectious lab markers, and evidence of complete wound healing from her prior procedures. The success rate of two-stage revisions has been reported to range from 65% to 90% [2]. Frequently encountered organisms include coagulase-negative staphylococci, methicillin-susceptible S. aureus, and polymicrobial infections [2]. In this case, aspiration cultures grew Mycobacterium intracellulare, a Gram-positive, acid-fast bacillus that is non-motile, non-spore-forming, and commonly acquired through the respiratory or gastrointestinal tract [3]. This opportunistic organism typically colonizes immunocompromised hosts, such as those with HIV or those taking immunomodulatory medications [3]. This patient’s diagnosis and treatment course were unique for several reasons. Non-tuberculous mycobacterial PJIs are rare; one study assessing infecting organisms in PJIs reported mycobacteria as the causative agent in <0.6% of cases [4]. These organisms form biofilms that facilitate their growth and further complicate treatment [5]. Due to the scarcity of documented cases of Mycobacterium intracellulare PJI, a standardized treatment regimen has not been established. To best eradicate infection, prolonged multidrug antimicrobial therapy is recommended. However, this increases the likelihood of medication side effects, as demonstrated by our patient [6]. A typical regimen includes rifampin, ethambutol, and azithromycin, continued until infection eradication, after which spacer removal and reimplantation can be performed [6]. This case is also unique due to the duration of antibiotic spacer retention. Her spacer remained in place far longer than is typically recommended. Most antibiotic spacers remain in place for 6–8 weeks; in this case, the spacer was retained for 18 months – one of the longest durations documented in orthopedic literature. Extended spacer use was necessary to ensure clearance of infection. Antimicrobial treatment for non-tuberculous mycobacteria generally lasts 12 months; however, due to medication intolerance, the course was prolonged. Three additional case reports document prolonged spacer retention exceeding 1 year, including during the COVID-19 pandemic or in patients with medical comorbidities precluding earlier reimplantation [7,8]. One case report describes a 7-year interval between spacer placement and reimplantation [9]. Numerous types of antibiotic spacers exist, and arthroplasty surgeons must be aware of the advantages and disadvantages of each when determining the best option for their patient. Broadly, antibiotic spacers are made of polymethyl methacrylate and are loaded with antibiotics that elute into the surrounding tissues. They may be static – spanning the knee joint and preventing motion – or articulating, which preserve knee motion. Static spacers may be preferred for low-demand or non-ambulatory patients and allow soft-tissue healing without joint motion. However, prolonged immobilization may result in quadriceps and collateral ligament atrophy and arthrofibrosis, leading to decreased postoperative range of motion [10]. Prolonged antibiotic spacer retention is not benign and is associated with complications such as supracondylar femur fractures and spacer dislocations, and antibiotic spacer revision rates have been shown to be as high as 21% for implants retained for 2 years [11]. Many surgeons prefer articulating spacers because they allow patients to maintain motion and ambulation, minimize bone loss, and facilitate easier reimplantation. Articulating spacers include several subtypes and may be handmade (cement-on-cement), cement-on-polyethylene, or prefabricated. Prefabricated spacers offer greater mechanical integrity but have limited size availability, prompting some surgeons to modify or create custom articulating spacers. This case represents the successful use of a prefabricated antibiotic spacer retained for over 1 year. Finally, this patient also experienced significant financial and psychological burdens associated with her infection. She unfortunately experienced numerous side effects from her antibiotic therapy and also suffered from losses in function and mobility with her spacer placement. Although it was not quantitatively documented, it was clear that her quality of life was significantly impacted by her diagnosis.
This unique case may serve as a guide for arthroplasty surgeons who encounter a rare PJI or require prolonged retention of an antibiotic spacer. Ideally, standardized functional outcome scores would be reported to assess improvement but were not collected throughout the course of treatment. The findings in our report may not be generalizable to the broader PJI population, but they highlight the importance of close collaboration with infectious disease specialists and the necessity of patience from both surgeon and patient to ensure complete eradication of infection before definitive revision arthroplasty.
This case highlights the management of a rare prosthetic joint infection with Mycobacterium intracellulare. It also highlights the use and management of an extended retained antibiotic spacer in these circumstances.
References
- 1. Jitmuang A, Yuenyongviwat V, Charoencholvanich K, Chayakulkeeree M. Rapidly-growing mycobacterial infection: A recognized cause of early-onset prosthetic joint infection. BMC Infect Dis 2017;17:802. [Google Scholar] [PubMed]
- 2. Kildow BJ, Springer BD, Brown TS, Lyden ER, Fehring TK, Garvin KL. Long term results of two-stage revision for chronic periprosthetic knee infection: A multicenter study. J Arthroplasty 2022;37:S327-32. [Google Scholar] [PubMed]
- 3. Akram SM, Attia FN. Mycobacterium avium complex. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431110/. Accessed December 12, 2026. [Google Scholar] [PubMed]
- 4. Aggarwal VK, Bakhshi H, Ecker NU, Parvizi J, Gehrke T, Kendoff D. Organism profile in periprosthetic joint infection: Pathogens differ at two arthroplasty infection referral centers in Europe and in the United States. J Knee Surg 2014;27:399-406. [Google Scholar] [PubMed]
- 5. Yamazaki Y, Danelishvili L, Wu M, Macnab M, Bermudez LE. Mycobacterium avium genes associated with the ability to form a biofilm. Appl Environ Microbiol 2006;72:819-25. [Google Scholar] [PubMed]
- 6. Coda R, Waller S, Vopat B. Nontuberculosis Mycobacterium infections in orthopaedic surgery: Review of the epidemiology, pathogenesis, diagnosis, and treatment guidelines. J Am Acad Orthop Surg Glob Res Rev 2025;9:e24.00274. [Google Scholar] [PubMed]
- 7. Welsh CR, Baumann PA. Two-stage total knee arthroplasty revision with extended antibiotic spacer use. Cureus 2021;13:e14854. [Google Scholar] [PubMed]
- 8. Young K, Chummun S, Wright T, Darley E, Chapman TW, Porteous AJ, et al. Management of the exposed total knee prosthesis, a six-year review. Knee 2016;23:736-9. [Google Scholar] [PubMed]
- 9. Park YB, Ha CW, Jang JW, Kim M. Antibiotic-impregnated articulating cement spacer maintained for 7 years in situ for two-stage primary total knee arthroplasty: A case report. BMC Musculoskelet Disord 2019;20:179. [Google Scholar] [PubMed]
- 10. Warth LC, Hadley CJ, Grossman EL. Two-stage treatment for total knee arthroplasty infection utilizing an articulating prefabricated antibiotic spacer. J Arthroplasty 2020;35:S57-62. [Google Scholar] [PubMed]
- 11. Petis SM, Perry KI, Pagnano MW, Berry DJ, Hanssen AD, Abdel MP. Retained antibiotic spacers after total hip and knee arthroplasty resections: High complication rates. J Arthroplasty 2017;32:3510-8. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A Rare Case of Salmonella Typhimurium Prosthetic Joint Infection in Total Hip Arthroplasty in a Young Patient with Long-term Corticosteroid Therapy
June 1, 2026 A Rare Case of Salmonella Typhimurium Prosthetic Joint Infection in Total Hip Arthroplasty in a Young Patient with Long-term Corticosteroid Therapy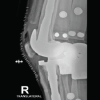 March 1, 2026 Sequential Bilateral Prosthetic Knee Infections Managed with Divergent Surgical Strategies: A Case Report
March 1, 2026 Sequential Bilateral Prosthetic Knee Infections Managed with Divergent Surgical Strategies: A Case Report December 1, 2025 Superior Gluteal Artery Perforation Following Girdlestone Resection Arthroplasty: A Case Report
December 1, 2025 Superior Gluteal Artery Perforation Following Girdlestone Resection Arthroplasty: A Case Report August 1, 2025 Haemophilus influenzae Acute Prosthetic Joint Infection: A Rare Case Report on Time-Critical, Pathogen-Specific Management
August 1, 2025 Haemophilus influenzae Acute Prosthetic Joint Infection: A Rare Case Report on Time-Critical, Pathogen-Specific Management