
Bicolumnar fixation using a lateral buttress plate combined with a medial titanium elastic nail (TENS) is an effective, “biologically-friendly” alternative to traditional dual-plating for complex bicondylar tibial plateau fractures.
Dr. Abhishek Shukla ingh, Department of Orthopaedics, Government Medical College, Satna, Madhya Pradesh, India. E-mail: 3king00009@gmail.com
Abstract
Introduction: Bicondylar tibial plateau fractures are complex intra-articular injuries that require stable fixation and early mobilization. Bicolumnar fixation using a buttress plate combined with a titanium elastic nail system (TENS) aims to provide biomechanical stability while preserving soft-tissue integrity.
Materials and Methods: A prospective study was conducted on 60 adult patients with bicondylar tibial plateau fractures treated with bicolumnar fixation. Demographic data, operative parameters, clinical union, complications, and functional outcomes were analyzed.
Results: The mean age of the patients was 37.4 ± 12.38 years. Clinical union was achieved in 36.7% of the patients. Significant differences were observed in operative time and blood loss between the sexes. Age and clinical union were significant predictors of the post-operative knee range of motion.
Conclusion: Bicolumnar fixation using a buttress plate and a TENS nail provides acceptable clinical and functional outcomes with stable fixation in bicondylar tibial plateau fractures.
Keywords: Tibial fractures, intra-articular fractures, fracture fixation.
Bicondylar tibial plateau fractures represent a subset of complex intra-articular injuries that predominantly arise from high-energy mechanisms such as motor vehicle accidents, falls from significant heights, or sports-related trauma [1]. These fractures are characterized by extensive articular surface comminution and disruption of the metaphyseal–diaphyseal junction, which collectively compromise both the structural integrity and biomechanical function of the knee joint [2]. The tibial plateau plays a pivotal role in load transmission across the knee and in maintaining joint congruity and stability; thus, fractures in this region pose significant challenges in achieving satisfactory anatomical and functional outcomes [3]. Inadequate or suboptimal management of bicondylar tibial plateau fractures can result in a spectrum of adverse sequelae, including persistent pain, joint stiffness, malalignment, instability, and the early onset of post-traumatic osteoarthritis [4]. These complications not only diminish the patient’s functional capacity but also adversely affect their overall quality of life and long-term mobility [5]. Consequently, the primary objectives in treating these injuries are to restore the articular surface anatomy meticulously, provide stable fixation to allow early joint motion, and preserve the biological environment conducive to fracture healing [6]. Traditional treatment modalities, such as open reduction and internal fixation (ORIF) using plates or isolated intramedullary nailing, have been widely employed. However, these approaches may fall short in addressing the intricate biomechanical demands posed by bicondylar fractures, especially when significant comminution and metaphyseal instability are present [7]. ORIF with plating, while allowing direct visualization and anatomical reduction, carries risks related to extensive soft-tissue dissection, which may increase the likelihood of wound complications and infections [8]. Conversely, intramedullary nailing alone may not provide adequate fixation for the articular fragments or restore the complex load distribution across the tibial plateau [9]. Both methods are susceptible to complications such as delayed union, malunion, hardware failure, and secondary deformities, particularly in osteoporotic bone or severely comminuted fracture patterns [10]. The biomechanical rationale underlying bicolumnar fixation stems from the recognition that the medial and lateral tibial columns function as distinct yet interdependent structural units critical for knee stability [11]. Each column bears specific loads and contributes to maintaining the congruity of the knee joint under physiological stresses [12]. Bicolumnar fixation techniques aim to address this by combining buttress plating of the articular surfaces to counteract shear and compressive forces with intramedullary fixation to provide axial stability and share load transmission along the tibial shaft [13]. This synergistic approach enhances mechanical stability, reduces micromotion at the fracture site, and facilitates early functional rehabilitation. The titanium elastic nail system (TENS) has emerged as a valuable adjunct in this context due to its unique properties. TENS offers elastic intramedullary stabilization that preserves the periosteal blood supply and fracture hematoma, both of which are essential for biological healing processes. Its flexible nature promotes controlled micro-motion at the fracture site, stimulating callus formation and accelerating union [14]. When integrated into a bicolumnar fixation strategy, TENS effectively addresses metaphyseal and diaphyseal instability, complementing the buttress plating by reducing stress concentration and distributing mechanical loads more evenly across the fracture construct [15]. This combined fixation method not only enhances the biomechanical environment for healing but also minimizes soft-tissue trauma, thereby reducing post-operative complications. Clinically, the application of bicolumnar fixation incorporating TENS has been associated with improved fracture union rates, better restoration of knee joint alignment and stability, and enhanced functional outcomes. Early mobilization facilitated by stable fixation helps prevent joint stiffness and muscle atrophy, which are critical factors in the rehabilitation process [16]. Furthermore, this approach may mitigate the risk of secondary osteoarthritis by preserving joint congruity and reducing abnormal load transmission [17]. Despite these advantages, patient-specific factors such as fracture pattern, bone quality, and soft-tissue condition must be carefully considered to tailor the fixation strategy optimally [18]. In summary, bicondylar tibial plateau fractures demand a comprehensive treatment approach that addresses both the mechanical and biological challenges inherent to these injuries. Bicolumnar fixation, combining buttress plating with elastic intramedullary stabilization through TENS, represents a biomechanically sound and biologically favorable technique. This method seeks to restore anatomical alignment, provide stable fixation, and promote early mobilization, thereby improving the prospects for successful fracture healing and functional recovery.
This prospective observational study was conducted to evaluate the clinical and radiological outcomes of bicolumnar fixation using a combination of a lateral buttress plate and a transverse elastic nail system (TENS) nail in bicondylar tibial plateau fractures. The Single-center study was carried out in the Department of Orthopedics at Index Medical College. Ethical permission was taken before the study IEC NO (IMCHRC/IEC/2022/126). A total of 60 patients with bicondylar tibial plateau fractures were included in the study. All fractures resulted from high-energy trauma, predominantly road traffic accidents. Patients aged between 18 and 60 years were enrolled after obtaining informed written consent. This study prospectively enrolled patients aged 18–60 years presenting with closed bicondylar tibial plateau fractures who were deemed medically fit for surgery. By limiting the age range and focusing on closed injuries, the protocol minimizes confounding variables associated with geriatric bone quality and the high infection rates typical of open trauma. To ensure a homogenous cohort, several exclusions were applied: Pathological, undisplaced, and open fractures were omitted. Elderly patients with osteoporotic bone who commonly sustain tibial plateau fractures were also excluded. In addition, patients with severe medical comorbidities were excluded to reduce perioperative risk and ensure that functional outcomes were primarily attributable to the surgical intervention. No Biochemical and computed tomography scan intervention was done.
Pre-operative evaluation
All patients underwent detailed clinical evaluation on admission, including the assessment of soft-tissue condition, neurovascular status, and associated injuries. Preoperative investigations included routine hematological tests and radiological assessment using digital anteroposterior and lateral radiographs of the knee joint. Fracture patterns were analyzed, preoperative planning was performed for optimal fixation strategy, and all surgeries were performed under regional or general anesthesia with the patient positioned supine on a radiolucent operating table. An anterolateral approach to the proximal tibia was used under tourniquet control. After adequate exposure, reduction of the articular surface and condylar fragments was achieved under fluoroscopic guidance, and a lateral condylar buttress plate was applied and fixed with appropriate cortical and cancellous screws to stabilize the lateral column. Subsequently, through a separate approximately 2 cm medial incision, a TENS nail was introduced into the medullary canal of the tibia under C-arm guidance to support the medial column. Proper positioning and fixation were confirmed by fluoroscopy. The wounds were closed in layers after hemostasis was achieved.
Post-operative rehabilitation
Postoperatively, patients started quadriceps strengthening exercises and knee range-of-motion exercises from the fourth post-operative day, depending on pain tolerance and soft-tissue condition. Partial weight-bearing with crutches was initiated and gradually progressed to full weight-bearing based on clinical and radiological evidence of fracture healing. The patients were followed-up at regular intervals.
Outcome measures
Patients underwent comprehensive clinical and radiological evaluations over a minimum follow-up period of 12 months, with functional outcomes quantified using the Schatzker and Lambert scoring system. Assessment parameters focused on the biological and mechanical success of fixation, specifically the time to clinical and radiological union, recovery of knee range of motion, and quadriceps muscle strength. Additionally, physical markers such as limb length discrepancy, walking ability, and overall functional mobility were monitored to determine the quality of life after recovery. Comprehensive data regarding surgical performance and post-operative safety were also recorded, including operative duration, intraoperative blood loss, and the incidence of post-operative infection. To identify potential technical or physiological hurdles, the study documented specific complications such as implant failure, delayed union, and non-union. These metrics provide a holistic overview of the efficacy of surgical intervention and long-term stability of bicondylar fixation.
Data collection and statistical analysis
Data were recorded using a structured form, including demographic details, fracture characteristics, operative notes, rehabilitation progress, and follow-up findings. Statistical analysis was performed using the appropriate statistical software. Descriptive statistics were used for baseline characteristics, and inferential statistics were used to assess outcome measures. Statistical significance was set at P < 0.05.
The demographic characteristics of the study population are summarized in (Table 1). The mean age of the patients was 37.4 ± 12.38 years (range 19–59 years), with a nearly equal sex distribution, and operative parameters, including operative time and intraoperative blood loss, are detailed in (Table 2).
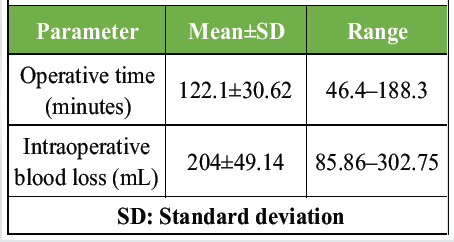
Table 2: Operative parameters
The mean operative time was 122.1 ± 30.62 min, and the mean blood loss was 204 ± 49.14 mL. Clinical union was achieved in 22 patients (36.7%), whereas 38 patients (63.3%) did not achieve clinical union at the time of assessment. A statistically significant relationship was observed between complications and failure to achieve clinical union. Strong correlations were observed for both pairs of variables. Multiple linear regression analysis identifying predictors of post-operative knee range of motion showed that age and clinical union emerged as significant predictors, whereas sex and blood loss were not statistically significant (Table 3).
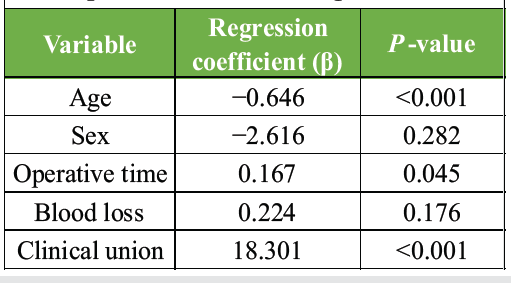
Table 3: Multiple linear regression analysis for predictors of knee range of motion
The management of bicondylar tibial plateau fractures poses significant challenges due to the complex geometry of the fractures, involvement of the articular surface, and vulnerability of the soft tissues. This prospective study demonstrates that bicolumnar fixation, using a lateral buttress plate in combination with a titanium elastic nail, provides stable fixation along with satisfactory functional and radiological outcomes. The patient demographics in this study align with the typical injury profile, featuring a mean age of 37.4 years and an almost equal distribution of genders. The operative parameters were within acceptable ranges; however, it was observed that male patients experienced significantly longer operative times and greater blood loss. A strong positive correlation between operative time and blood loss underscores the impact of fracture complexity and surgical duration on intraoperative morbidity. Clinical union was achieved earlier in 36.7% of the patients, while delayed union was often linked to post-operative complications. The notable relationship between complications and delayed union highlights the necessity for meticulous surgical techniques and attentive post-operative management. Similar findings have been documented in earlier studies assessing complex tibial plateau fractures. Functional assessments indicated that advancing age was significantly correlated with a decrease in knee range of motion. Multivariate regression analysis identified both age and the attainment of clinical union as strong predictors of final knee mobility, underscoring the significance of biological healing and patient-related factors in functional recovery. Although a longer operative time was positively associated with range of motion, this may indicate a more accurate fracture reduction in complex cases rather than merely the duration of the operation. In comparison to traditional dual plating, bicolumnar fixation offers benefits such as load sharing, metaphyseal support, and minimized medial soft-tissue dissection. Biomechanical and clinical investigations have indicated enhanced stability and acceptable complication rates with plate-nail constructs.
This study provides a comprehensive understanding of the multifaceted aspects that influence the outcomes of bicolumnar fixation of bicondylar tibial fractures. By elucidating demographic patterns, surgical variables, and their impact on clinical recovery, this study offers valuable insights for enhancing patient care, refining surgical techniques, and advancing orthopedic practices. Continued research and clinical implementation of evidence-based strategies are essential to further improve outcomes and ensure optimal recovery for patients with bicondylar tibial fractures.
Limitations
This study was performed by a single surgical team, so there is a chance of surgeon-dependent bias. Post-operative alignment parameters such as tibial plateau angle, posterior slope, and limb alignment were not quantitatively analyzed in this study. Due to the need for specialized surgical skills and intraoperative fluoroscopic support, outcomes might not be easily reproducible in every clinical scenario. Minor complications such as superficial infections, knee stiffness, or implant irritation were also not analyzed. Functional outcomes were assessed using the Schatzker and Lambert scoring system alone, without incorporating widely validated patient-reported outcome measures such as KOOS or Lysholm knee scores.
In the management of complex bicondylar tibial plateau fractures (Schatzker Types V and VI), bicolumnar fixation using a lateral buttress plate combined with a medial titanium elastic nail (TENS) provides a stable, “biologically-friendly” alternative to traditional dual-plating. This hybrid approach ensures sufficient medial column support to prevent varus collapse while minimizing extensive soft-tissue stripping, ultimately facilitating early joint mobilization and favorable radiological union.
References
- 1. Apostolou CD, Markopoulou V, Chatzipanagiotou G, Efstathiou S, Chronopoulos E. Association between tibial plateau fractures and bone metabolic status: A prospective observational study. Cureus 2025;17:e92476. [Google Scholar] [PubMed]
- 2. Rudran B, Little C, Wiik A, Logishetty K. Tibial plateau fracture: Anatomy, diagnosis and management. Br J Hosp Med (Lond) 2020;81:1-9. [Google Scholar] [PubMed]
- 3. Liu CD, Hu SJ, Chang SM, Du SC, Chu YQ, Qi YM, et al. Treatment of posterolateral tibial plateau fractures: A narrative review and therapeutic strategy. Int J Surge 2025;111:1071-82. [Google Scholar] [PubMed]
- 4. Chang H, Zheng Z, Yu Y, Shao J, Zhang Y. The use of bidirectional rapid reductor in minimally invasive treatment of bicondylar tibial plateau fractures: Preliminary radiographic and clinical results. BMC Musculoskelet Disord 2018;19:419. [Google Scholar] [PubMed]
- 5. Herrera-Pérez M, Valderrabano V, Godoy-Santos AL, De César Netto C, González-Martín D, Tejero S. Ankle osteoarthritis: Comprehensive review and treatment algorithm proposal. EFORT Open Rev 2022;7:448-59. [Google Scholar] [PubMed]
- 6. Petrovych O, Florek J, Georgiew F, Kawa P, Florek P. Comminuted transarticular fracture of the middle phalanx: A non-standard surgical procedure. Cureus 2025;17:e97754. [Google Scholar] [PubMed]
- 7. Cui X, Chen H, Rui Y, Niu Y, Li H. Two-stage open reduction and internal fixation versus limited internal fixation combined with external fixation: A meta-analysis of postoperative complications in patients with severe Pilon fractures. J Int Med Res 2018;46:2525-36. [Google Scholar] [PubMed]
- 8. Nadeem A, Abbasi H. Outcomes of intramedullary nailing versus plate fixation in the management of humeral shaft fractures: A systematic review and meta-analysis. Cureus 2024;16:e72473. [Google Scholar] [PubMed]
- 9. Wani IH, Ul Gani N, Yaseen M, Bashir A, Bhat MS, Farooq M. Operative management of distal tibial extra-articular fractures – intramedullary nail versus minimally invasive percutaneous plate osteosynthesis. Ortop Traumatol Rehabil 2017;19:537-41. [Google Scholar] [PubMed]
- 10. Sun Q, Wu X, Wang L, Cai M. The plate fixation strategy of complex proximal humeral fractures. Int Orthop 2020;44:1785-95. [Google Scholar] [PubMed]
- 11. Klima ML. Mechanical complications after intramedullary fixation of extracapsular hip fractures. J Am Acad Orthop Surg 2022;30:e1550-62. [Google Scholar] [PubMed]
- 12. Kim D, Lim JR, Yoon TH, Shin SH, Chun YM. Lateral wall integrity of the greater tuberosity is important for the stability of osteoporotic proximal humeral fractures after plate fixation. J Bone Joint Surg Am 2024;106:1750-6. [Google Scholar] [PubMed]
- 13. Brial C, Mccarthy M, Adebayo O, Wang H, Chen T, Warren R, et al. Lateral meniscal graft transplantation: Effect of fixation method on joint contact mechanics during simulated gait. Am J Sports Med 2019;47:2437-43. [Google Scholar] [PubMed]
- 14. Tucker SM, Wee H, Fox E, Reid JS, Lewis GS. Parametric finite element analysis of intramedullary nail fixation of proximal femur fractures. J Orthop Res 2019;37:2358-66. [Google Scholar] [PubMed]
- 15. Jeremic D, Grubor N, Bascarevic Z, Slavkovic N, Krivokapic B, Vukomanovic B, et al. Comparative analysis of complication rates in tibial shaft fractures: Intramedullary nail vs. Ilizarov external fixation method. J Clin Med 2024;13:2034. [Google Scholar] [PubMed]
- 16. Bottlang M, Shetty SS, Blankenau C, Wilk J, Tsai S, Fitzpatrick DC, et al. Advances in dynamization of plate fixation to promote natural bone healing. J Clin Med 2024;13:2905. [Google Scholar] [PubMed]
- 17. Ayhan EM, Nair M, Levitt SJ, Levy BA, Medvecky MJ. Knee-spanning external fixation in the management of knee dislocations and multiligamentous knee injuries: A narrative review. Open Access J Sports Med 2025;16:131-49. [Google Scholar] [PubMed]
- 18. Paladugu P, Kumar R, Ong J, Waisberg E, Sporn K. Virtual reality-enhanced rehabilitation for improving musculoskeletal function and recovery after trauma. J Orthop Surg Res 2025;20:404. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2025 Comparative Evaluation of Functional Outcomes Following Surgical and Conservative Management of Distal Tibia Shaft Fractures: A Prospective Observational Study
July 1, 2025 Comparative Evaluation of Functional Outcomes Following Surgical and Conservative Management of Distal Tibia Shaft Fractures: A Prospective Observational Study June 1, 2026 Comparison of Surgical Outcomes and Perioperative Laboratory Parameters Following Minimally Invasive Plate Osteosynthesis versus Conventional Plating in Long Bone Fractures
June 1, 2026 Comparison of Surgical Outcomes and Perioperative Laboratory Parameters Following Minimally Invasive Plate Osteosynthesis versus Conventional Plating in Long Bone Fractures May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing
May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing December 1, 2025 Hook Plate Fixation of an Isolated Pisiform Fracture with a Small Proximal Fragment: A Case Report
December 1, 2025 Hook Plate Fixation of an Isolated Pisiform Fracture with a Small Proximal Fragment: A Case Report