
Early diagnosis of aneurysmal bone cyst as an underlying cause of subtrochanteric femur fractures in adolescents and management with thorough clerance of lesion, bone grafting, and stable fixation can lead to definitive fracture union and prevention of complications or recurrence.
Dr. Chandrashekhar R Rai, Department of Orthopaedics, GGMC and JJH, Mumbai, Maharashtra, India. E-mail: chandrashekharrai13@gmail.com
Abstract
Introduction: Aneurysmal bone cyst is a locally aggressive as well as benign bony lesion most commonly seen in adolescents. Although it mostly involves the metaphysis of long bones, presents as a fracture which is pathological in the subtrochanteric region of the femur is rare. The subtrochanteric femur is a biomechanically demanding region of the lower limb, and the presence of an underlying cystic pathology can complicate fracture management. Management of subtrochanteric femur fractures due to aneurysmal bone cysts in adolescents is limited, as described in the literature. This case is a rare presentation and to denote an effective surgical treatment with anatomical reconstruction and stable fixation.
Case Report: A 14-year-old male presented with pain and inability to bear weight on the left hip joint following trauma which was trivial. There was localized tenderness and restricted hip movement on clinical examination. X-rays demonstrated left sided subtrochanteric femur fracture along with an underlying expansile lytic lesion. Magnetic resonance imaging was done in order to assess the extent of the lesion and to help in further management. The patient underwent surgical management, which consisted of curettage of the lesion, fixation using a dynamic condylar screw with cancellous allogenic bone grafting. Confirmation with the diagnosis of aneurysmal bone cyst was also confirmed using histopathology. The post-operative course was uneventful, and follow-up showed union of the fracture with incorporation of the bone graft with gradual full weight bearing without pain.
Conclusion: Subtrochanteric femur fractures, which are pathological due to aneurysmal bone cysts, are rare in adolescents and are challenging to manage. This case demonstrates that there are satisfactory results if the lesion is managed by clearance combined with bone grafting and stable internal fixation. The novelty of this report lies in documenting the successful fixation of this rare presentation using a dynamic condylar screw. The important learning point is that adherence to both biological as well as mechanical principles are necessary for optimal outcomes in involving the subtrochanteric femur, which are pathological in origin.
Keywords: Aneurysmal bone cyst, pathological femur fracture, subtrochanteric femur fracture, dynamic condylar screw fixation, bone grafting.
Aneurysmal bone cyst is a benign, expansile, osteolytic bone lesion characterized by blood-filled spaces separated by connective tissue septa. It predominantly affects children and adolescents and commonly involves the metaphyseal region of long bones, particularly around the knee and proximal humerus [1,2]. Although benign, the lesion can be locally aggressive and may compromise structural integrity, predisposing the affected bone to pathological fractures [3]. Clinical presentation most commonly includes pain, swelling, and restricted movement.
Pathological fractures associated with aneurysmal bone cysts of the femur have been reported in the literature; however, involvement of the subtrochanteric region remains rare [4]. The subtrochanteric femur is subjected to high biomechanical stresses, making fracture management technically demanding, especially in the presence of an underlying bone lesion. Various treatment strategies have been described, including curettage with bone grafting, intralesional adjuvant therapies, and internal fixation using different implants [5]. However, there is no consensus regarding the optimal fixation method in skeletally immature patients with subtrochanteric pathological fractures.
The literature largely consists of rare case reports and few case series, with limited emphasis on the selection of implants along with outcomes which are long-term and functional in adolescents. This mainly highlights a gap in research in the role of stable methods of fixation, which would achieve outcomes which are satisfactory while reducing complications and recurrence. The main objective of this study is to present the clinical features, surgical management, and results of a pathological subtrochanteric femur fracture with aneurysmal bone cyst in an adolescent, managed with curettage, dynamic condylar screw fixation, and bone grafting.
This case report mainly focuses on the limited literature available for the management of such rare presentations and to support the use of stable internal fixation in along with adequate lesion clearance. The main limitation of this study is that it is a rare presentation with a single case study; however, it provides important insight into a rare clinical scenario and its successful management.
This study is a single-patient clinical case report conducted in the Department of Orthopedics at Grant Medical College and Sir J.J. Group of Hospitals. Written informed consent was obtained from the patient’s legal guardian for participation in the study and for the use of clinical data and radiological images for academic and publication purposes.
A 14-year-old male patient presented with pain, swelling, and inability to bear weight on the left hip joint after trauma which was trivial. Clinical evaluation was performed, which included limb alignment, tenderness over the hip joint, range of motion of the hip joint, as well as distal neurovascular status. Imaging evaluation consisted of plain X-rays of the pelvis with both hips and anteroposterior and lateral views of femur to assess fracture pattern and morphology.[Figure 1]
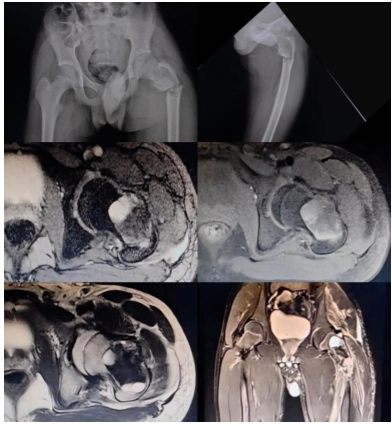
Figure 1: Pre-operative imaging of affected hip showing anteroposterior and lateral X-rays and magnetic resonance imaging delineating the subtrochanteric femur fracture with aneurysmal bone cyst.
To characterize the lesion, magnetic resonance imaging of the affected femur was performed. To evaluate the extent of the cystic lesion, internal septations, fluid-fluid levels, cortical breach, and any associated soft-tissue involvement, the imaging protocol was T1-weighted, T2-weighted, and fluid-sensitive sequences. These magnetic resonance imaging findings were used for confirming the diagnosis along with surgical planning and further management.[Figure 1]
Routine pre-operative laboratory investigations, including complete blood count, inflammatory markers, and coagulation profile, were obtained for pre-anesthetic checkup. After optimization, surgical intervention was carried out under regional anesthesia with the patient positioned supine on a fracture table. A lateral approach to the proximal femur with splitting of vastus laterally muscle was performed. After exposure, thorough intralesional cyst curettage was performed until healthy bleeding bone was seen. A thorough wash was given, followed by intralesional allogenic cancellous bone grafting. A sandwich technique of bone grafting was done, which consisted of an outer layer of cortical bone graft, a middle layer of cancellous bone graft, followed by cortical bone grafting.
Fracture fixation was done using a dynamic condylar screw fixation system. Proper reduction and implant placement were ensured using intraoperative fluoroscopic guidance. Samples curetted from the cyst were sent for histopathological examination to establish a definitive diagnosis.
Post-operative management included intravenous antibiotics, analgesia, and limb elevation. Rehabilitation protocol consisted of early range-of-motion exercises, followed by non-weight-bearing mobilization. Gradual progression to partial and then full weight-bearing was allowed based on clinical assessment and serial radiographic evidence of fracture union and graft incorporation. Follow-up evaluations were conducted at regular intervals to assess fracture healing, implant integrity, functional recovery, and any evidence of lesion recurrence.[Figure 2]
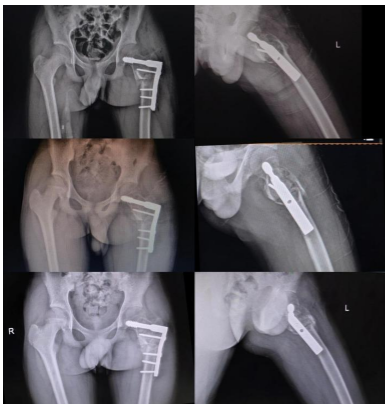
Figure 2: Post-operative follow-up X-rays showing union of the fracture site with graft uptake.
Clinically and radiologically patient was followed up at regular intervals after surgical management. The post-operative period was uneventful, with no distal neurovascular deficit and wound-related complications. Immediate post-operative X-rays demonstrated anatomical fracture reduction and stable implant positioning. Serial follow-up X-rays suggested progressive callus formation, maintenance of reduction, and gradual incorporation of the bone graft. Union demonstrated over X-rays was achieved within the time frame for a pathological subtrochanteric femur fracture. Clinically, there was improvement in pain and mobility, and the patient was able to resume with day to day restoration of hip function without pain. There was no evidence of implant failure or local recurrence during follow-up. The last date of follow-up was March 27, 2026, which showed adequate callus with union of the fracture site. Patient is currently walking without support with full weight bearing without any complaints of daily activities.[Figure 3]

Figure 3: Post-operative follow-up clinical photo of patient showing cross-legged sitting, standing, and active straight leg raising.
As this study represents a single-patient case report, statistical analysis was not applicable. Instead, clinical parameters such as fracture union, full weight-bearing, no complications, and lack of recurrence were used to assess treatment outcome, as commonly reported in similar case-based studies [4,5].
Aneurysmal bone cysts are locally aggressive but benign lesions, most frequently affecting children and adolescents [1,2,6]. Although femur is commonly involved, pathological fractures in the subtrochanteric region are rare and present with difficulty due to high biomechanical stresses in this area [2,4,8]. Various studies have highlighted that incomplete or inadequate treatment of the lesion in skeletally immature patients may result in recurrence [6,9].
Bone grafting and curettage are the most accepted treatment modality for aneurysmal bone cysts, with recurrence rates as high as 10–30% in various series [5,10]. Various authors have emphasized the importance of internal fixation with bone grafting and clearance when the fracture is pathological, to restore mechanical stability and allow early rehabilitation [4,10]. In the present case, a dynamic condylar screw with rotational stability in the subtrochanteric region helps in satisfactory fracture healing and functional recovery. These findings are consistent with previously published reports describing good outcomes following stable internal fixation of pathological subtrochanteric femur fractures associated with aneurysmal bone cysts [4,5,8].
The limitations of this report include its single-case design and limited duration of follow-up, which restrict the generalizability of the findings. In addition, long-term surveillance is necessary to detect late recurrence, which has been reported in previous studies [6,9]. Despite these limitations, this case contributes to the limited literature on pathological subtrochanteric femur fractures due to aneurysmal bone cysts in adolescents and supports the role of thorough lesion clearance, bone grafting, and stable internal fixation in achieving satisfactory clinical and radiological outcomes.
Due to high biomechanical demands and the presence of a pathological fracture along with aneurysmal bone cyst, the choice of a 95° dynamic condylar screw and plate for fixation in this case was used. Due to high rotational and compressive forces at the subtrochanteric region, a fixation device that maintains both rotational as well as well compression was required. In the presence of an aneurysmal bone cyst, bone quality is reduced, making it osteoporotic at the lesion site, which further increases the chances of implant failure. Due to this construct, there is an additional advantage of adequate curettage and bone grafting of the lesion without compromising mechanical stability. In addition, the dynamic condylar screw, due to its nature, prevents varus collapse, which is most commonly seen in subtrochanteric pathological femur fracture. Therefore, due to stable fixation and adequate biological maintenance, the use of a 95° dynamic condylar screw and plate facilitates union and early rehabilitation in this adolescent patient.
Subtrochanteric femur fractures, which are pathological with aneurysmal bone cysts, are rare in adolescents and have significant management challenges. A subtrochanteric femur fracture following trivial trauma in an adolescent due to an underlying aneurysmal bone cyst is an uncommon presentation. The use of a 95-degree dynamic condylar screw for fixation in such cases is less frequently reported in current practice. In this case, thorough curettage of the cyst followed by stable fixation with an appropriately selected implant resulted in satisfactory fracture reduction, early rehabilitation, and no evidence of recurrence on follow-up. The combination of this rare presentation and successful management highlights the uniqueness of this case and its relevance to clinical practice.
Early diagnosis of aneurysmal bone cyst as an underlying cause of subtrochanteric femur fractures in adolescents and management with thorough clearance of lesion, bone grafting, and stable fixation can lead to definitive fracture union and prevention of complications or recurrence.
References
- 1. Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst: With emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg 1942;44:1004-25. [Google Scholar] [PubMed]
- 2. Leithner A, Lang S, Windhager R, Haas OA, Kainberger F, Kotz R. Aneurysmal bone cyst. A population based epidemiologic study and literature review. Clin Orthop Relat Res 1999;363:176-9. [Google Scholar] [PubMed]
- 3. Campanacci M. Bone and Soft Tissue Tumors. 2nd ed. Vienna: Springer-Verlag [Google Scholar] [PubMed]
- 4. Papagelopoulos PJ, Choudhury SN, Frassica FJ, Bond JR, Unni KK, Sim FH. Treatment of aneurysmal bone cysts of the pelvis and sacrum. JBJS. 2001 Nov 1;83(11):1674-81.; 1999. p. 965-80. [Google Scholar] [PubMed]
- 5. Garg S, Mehta S, Dormans JP. Modern surgical treatment of primary aneurysmal bone cyst of the spine in children and adolescents. J Pediatr Orthop 2005;25:387-92. [Google Scholar] [PubMed]
- 6. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, Villafuerte J, Gebhardt MC. Aneurysmal bone cyst: A review of 150 patients. J Clin Oncol 2005;23:6756-62. [Google Scholar] [PubMed]
- 7. Capanna R, Bettelli G, Biagini R, Ruggieri P, Bertoni F, Campanacci M. Aneurysmal cysts of long bones. Ital J Orthop Traumatol 1985;11:409-17. [Google Scholar] [PubMed]
- 8. Rapp TB, Ward JP, Alaia MJ. Aneurysmal bone cyst. J Am Acad Orthop Surg 2012;20:233-41. [Google Scholar] [PubMed]
- 9. Lin PP, Brown C, Raymond AK, Deavers MT, Yasko AW. Aneurysmal bone cysts recur at juxtaphyseal locations in skeletally immature patients. Clin Orthop Relat Res 2008;466:722-8. [Google Scholar] [PubMed]
- 10. Cottalorda J, Bourelle S. Current treatments of primary aneurysmal bone cysts. J Pediatr Orthop B 2006;15:155-67. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report January 1, 2025 Aneurysmal Bone Cyst of Femoral Head : A Rare Case Report
January 1, 2025 Aneurysmal Bone Cyst of Femoral Head : A Rare Case Report July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report
July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report