
Importance of maintaining a broad differential for posterior ankle soft-tissue masses and the role of imaging and histology in reaching a definitive diagnosis.
Dr. Abhishek Chaudhary, Department of Orthopaedics, Postgraduate Institute of Medical Education and Research, Chandigarh, India. E-mail: abisekh.chaudhary@gmail.com
Abstract
Introduction: Benign soft-tissue tumors are found in the foot and ankle region rarely, depicting <8%, namely, giant cell tumors, lipomas, or even leiomyomas. Leiomyomas are benign mesenchymal tumors composed of well-differentiated smooth muscle cells, most commonly found in the uterus, gastrointestinal tract, and skin.
Case Report: This report highlights a very rare case of a leiomyoma located adjacent to the Achilles tendon in a middle-aged woman, ultimately leading to painful movement.
Conclusion: It reinforces the importance of considering a wide variety of differentials for diagnosis of ankle and heel masses, particularly when imaging shows a benign-appearing, non-invasive lesion. It is imperative to go step by step in radiology and histological examination to prevent a misdiagnosis. Awareness, along with coordination among clinicians, radiologists, and pathologists, can lead to earlier diagnosis and avoid unnecessary anxiety or overtreatment.
Keywords: Heel, leiomyoma, benign soft tissue.
Benign soft-tissue tumors are found in the foot and ankle region rarely, depicting <8%, namely giant cell tumors, lipomas, or even leiomyomas [1]. Leiomyomas are benign mesenchymal tumors composed of well-differentiated smooth muscle cells, most commonly found in the uterus, gastrointestinal tract, and skin [2,3]. They can be further divided into angioleiomyomas, piloleiomyomas, and genital leiomyomas based on their tissue of origin [3]. Cutaneous leiomyomas are mostly found in the extremities and lead to pain secondary to a growing mass. Presentation in deep soft tissues or in relation to tendinous structures, such as the Achilles tendon, is rare and often underrecognized. Among soft-tissue leiomyomas, subtypes include cutaneous, angioleiomyomas (vascular), and deep soft-tissue leiomyomas, each with distinct clinical and histologic profiles [4].
Leiomyomas have been reported in various parts of the body, but foot and ankle involvement is particularly uncommon [5]. In this region, leiomyomas may arise from smooth muscle within vessel walls or tendon sheaths and are often misdiagnosed clinically as more frequent benign lesions, such as ganglion cysts, lipomas, synovial sarcomas, or fibromatoses [6,7]. Their rarity, slow-growing nature, and typically benign behavior contribute to diagnostic delays. The patient only presents when symptomatic, and it is imperative to be informed about such rare conditions for adequate management.
This report highlights a very rare case of a leiomyoma located adjacent to the Achilles tendon in a middle-aged woman, ultimately leading to painful movement, underlining the importance of maintaining a broad differential for posterior ankle soft-tissue masses and the role of imaging and histology in reaching a definitive diagnosis.
A 49-year-old female presented to the orthopedics outpatient department with a primary complaint of persistent pain and a gradually enlarging swelling in the posterior aspect of the left ankle, localized proximal to the heel region. The symptoms had been present for several months and were insidious in onset. The pain was described as dull aching in nature, aggravated on walking and prolonged standing, and partially relieved with rest. There was no history of trauma, weight loss, uterine fibroids, or renal cell carcinoma. On physical examination, a firm, non-mobile, mildly tender swelling was palpated over the medial aspect of the left heel, just superior to the insertion of the Achilles tendon. The overlying skin was intact without any signs of inflammation or discoloration. Range of motion at the ankle joint was preserved, although terminal plantarflexion elicited discomfort. No signs of neurovascular compromise were present. Ultrasonography of the left ankle demonstrated a well-defined, thin-walled, non-vascular, heterogeneous hypoechoic lesion located just posteromedial to the distal Achilles tendon insertion. The lesion measured approximately 18 × 10.8 × 6 mm. No intralesional vascularity or communication with the tendon was noted, raising suspicion of a benign soft-tissue neoplasm and warranting histological examination. Subsequently, magnetic resonance imaging (MRI) of the left ankle was performed, revealing a small altered signal intensity lesion in the subcutaneous plane on the posterosuperior aspect of the hindfoot, closely abutting the calcaneal insertion of the Achilles tendon. The lesion was isointense to muscle on T1-weighted images and hyperintense on PDFS images, suggestive of soft-tissue neoplasm (Fig. 1). 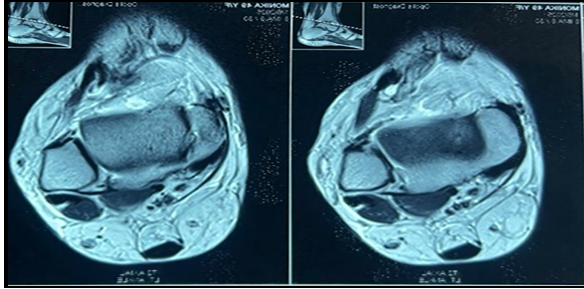
 Figure 1: (a) Sagittal view magnetic resonance imaging (MRI) showing the location of the benign tumor. (b) Axial view MRI showing the location of the benign tumor. (c) Coronal view MRI showing the location of the benign tumor.
Figure 1: (a) Sagittal view magnetic resonance imaging (MRI) showing the location of the benign tumor. (b) Axial view MRI showing the location of the benign tumor. (c) Coronal view MRI showing the location of the benign tumor.
 Figure 1: (a) Sagittal view magnetic resonance imaging (MRI) showing the location of the benign tumor. (b) Axial view MRI showing the location of the benign tumor. (c) Coronal view MRI showing the location of the benign tumor.
Figure 1: (a) Sagittal view magnetic resonance imaging (MRI) showing the location of the benign tumor. (b) Axial view MRI showing the location of the benign tumor. (c) Coronal view MRI showing the location of the benign tumor.
There was no intratendinous extension, nor was there any evidence of bony involvement or edema in adjacent musculature. Mild subcutaneous edema and degenerative subchondral cystic changes were noted in the naviculocuneiform joint and medial cuneiform bone. Based on clinical examination and imaging, a provisional diagnosis of a benign soft-tissue tumor adjacent to the Achilles tendon was made, and surgical excision with histopathological evaluation was planned to establish a definitive diagnosis and alleviate symptoms.
Treatment and follow-up
The patient underwent a planned surgical excision of the lesion under regional anesthesia in an elective setting. She was positioned prone, and a posterior-medial approach to the Achilles region was employed. A longitudinal skin incision was made parallel to the medial border of the tendon, and careful dissection was carried down through the subcutaneous tissue. A well-circumscribed, encapsulated white mass was identified in the subcutaneous plane, adjacent to but not involving the Achilles tendon. There were no adhesions or infiltration into surrounding structures (Fig. 2). The whole mass was meticulously excised and sent for histopathological analysis.
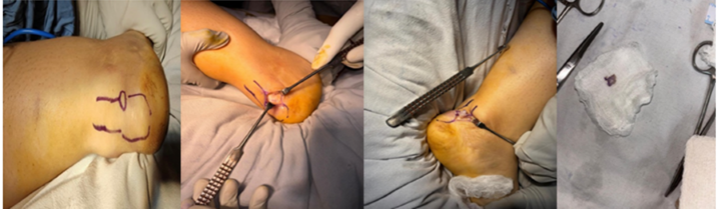 Figure 2: Intraoperative pictures of excision of the tumor.
Figure 2: Intraoperative pictures of excision of the tumor.
Grossly, the excised tissue measured 1.2 × 0.3 × 0.2 cm and appeared as a grey-white, irregular soft-tissue nodule. On histological examination, the lesion revealed a well-circumscribed spindle cell tumor composed of interlacing fascicles of smooth muscle cells with elongated nuclei, fine chromatin, and moderate eosinophilic cytoplasm. No evidence of nuclear atypia, mitoses, or necrosis was noted (Fig. 3). These features were consistent with leiomyoma, a benign smooth muscle tumor. Given the characteristic histomorphology, immunohistochemistry was not performed.
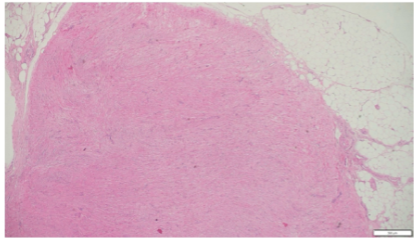
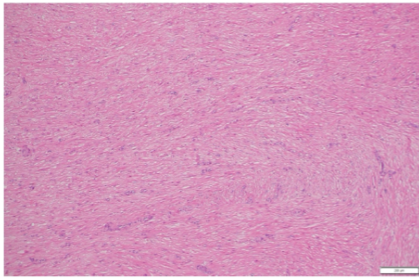
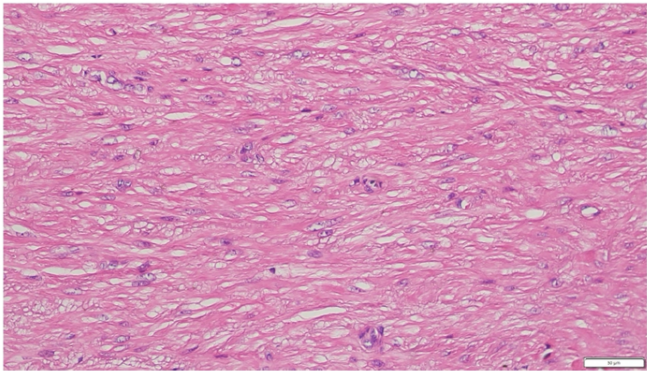
Figure 3: (a) Hematoxylin and eosin (H&E) (×4) photomicrograph shows a circumscribed spindle cell lesion arranged in interlacing fascicles. (b) H&E (×10) photomicrograph shows a circumscribed spindle cell lesion arranged in interlacing fascicles. (c) H&E (×20) photomicrograph shows a spindle cell have bland, round to ovoid nuclei, vesicular chromatin, small conspicuous nucleoli, and moderate eosinophilic cytoplasm. No increased atypia, necrosis, or mitosis is noted.
Postoperatively, the patient’s course was uneventful. A compression dressing was applied, and strict non-weight-bearing ambulation with crutch support was advised for the initial 7–10 days. Sutures were removed on post-operative day 14, and the patient was transitioned to partial and then full weight-bearing as tolerated. At 6-week follow-up, the patient reported significant symptomatic relief, with no pain or swelling and near-normal ankle mobility. At 3 months post-surgery, she had resumed routine activities and walking without discomfort. Follow-up clinical examination revealed no pain or swelling at the operative site. At her 6-month follow-up, the patient remained asymptomatic with full functional recovery and no evidence of tumor recurrence.
These tumors usually present in middle-aged adults, with a female preponderance, and often manifest as a firm, non-mobile subcutaneous nodule with or without pain. Angioleiomyomas, a vascular subtype of leiomyomas, are more likely to be painful due to ischemia or nerve compression, especially in weight-bearing locations such as the heel [5,8]. Ultrasound typically reveals a well-defined, hypoechoic lesion with variable internal echoes and, in vascular subtypes, Doppler flow [9]. MRI offers superior characterization: Leiomyomas are typically isointense to muscle on T1, hyperintense on T2/short tau inversion recovery, and show homogeneous enhancement on post-contrast imaging [10,11,12]. However, imaging findings are not pathognomonic and must be interpreted alongside clinical and pathological findings.
Histologically, leiomyomas demonstrate fascicles of uniform spindle-shaped smooth muscle cells with blunt-ended nuclei and eosinophilic cytoplasm. Absence of mitotic activity, atypia, and necrosis helps distinguish benign leiomyomas from their malignant counterparts, such as leiomyosarcoma [13,14]. Immunohistochemically, they express desmin, smooth muscle actin (SMA), and h-caldesmon [15]. The clinical presentation is typically a slow-growing subcutaneous mass that may be painful when located near neurovascular bundles. Cases in the posterior ankle may mimic entrapment syndromes (e.g., sural neuritis), calcific tendinitis, or retrocalcaneal bursitis. Our patient presented with localized pain and swelling, prompting imaging evaluation. Mohanty et al. reported a similar lesion in the Achilles tendon sheath leading to compressing the sural nerve in the foot, highlighting the need for clinical vigilance [16]. Histologically, leiomyomas consist of benign smooth muscle cells arranged in interlacing fascicles, with minimal pleomorphism, low mitotic activity, and no necrosis – distinguishing them from leiomyosarcoma or spindle cell sarcoma [11,12]. Immunohistochemistry is helpful when morphology is ambiguous: SMA, desmin, and h-caldesmon positivity confirms smooth muscle origin [15,17]. Surgical excision remains the definitive treatment. As these lesions are benign and well-encapsulated, marginal excision is usually curative. Recurrence is rare if the lesion is completely excised. Our patient had an uneventful recovery and remained recurrence-free at 6 months postoperatively. Similar outcomes were documented in case reports by D’Ambrosia and Ferguson, and Kinoshita et al., emphasizing surgical resection as curative in most cases [9].
Leiomyomas in the region of the Achilles tendon are exceptionally rare. In a large clinicopathologic review by Hachisuga et al., among 562 angioleiomyomas, the lower limb was the most commonly affected site (67%), but involvement of tendon sheaths, particularly the Achilles tendon, was virtually unreported [5]. In a case series by Gajanthodi et al., foot leiomyomas represented <1% of soft-tissue tumors in the region, most of which were angioleiomyomas [19]. They are difficult to diagnose with radiology, and hence, histology is the key investigation in such cases.
Szolomayer et al., reported eight patients with leiomyomas around the foot and ankle, and Jalgaonkar et al., even reported such tissue around the planter side of the for foot, initially identified as a fibroma [20,21]. Rarely these benign conditions have a propensity to progress into malignant leiomyosarcomas with an incidence of 0.13–0.29%. Cutaneous leiomyomas need to be evaluated thoroughly as they can be due to certain hereditary conditions like Reed’s syndrome [22].
Zaher et al., reported a superficial nodule over the posterior aspect of the tendo-achilles in a 57-year-old female with a probable diagnosis of a schwannoma by the radiologist on MRI. The histology ultimately reported the diagnosis of leiomyoma with immunohistochemistry depicting the diffuse expression of anti-actin smooth muscle antibodies, caldesmon, and desmin [23]. Another case report depicted the presence of the tissue around the heel in a 41-year-old female in 2018, which was initially treated for 6 months by a dermatologist and ultimately diagnosed on surgical excision and histology [24].
This case reinforces the importance of considering a wide variety of differentials for the diagnosis of ankle and heel masses, particularly when imaging shows a benign-appearing, non-invasive lesion. It is imperative to go step by step in radiology and histological examination to prevent a misdiagnosis. Awareness, along with coordination among clinicians, radiologists, and pathologists, can lead to earlier diagnosis and avoid unnecessary anxiety or overtreatment.
While treating soft-tissue tumors of the foot and ankle, however rare, it is important to keep a broad differential diagnosis with adequate radiological and pathological investigations.
References
- 1. Cheung MH, Lui TH. Plantar heel pain due to vascular leiomyoma (angioleiomyoma). Foot Ankle Spec 2012;5:321-3. [Google Scholar] [PubMed]
- 2. Suster S. Smooth muscle tumors of soft tissues. Adv Anat Pathol 2003;10:113-21. [Google Scholar] [PubMed]
- 3. Enzinger FM, Weiss SW. Soft Tissue Tumors. 5th ed. Amsterdam: Mosby Elsevier; 2008. [Google Scholar] [PubMed]
- 4. Fletcher CD, Bridge JA, Hogendoorn PC, Mertens F. WHO Classification of Tumours of Soft Tissue and Bone. 4th ed. France: IARC; 2013. [Google Scholar] [PubMed]
- 5. Hachisuga T, Hashimoto H, Enjoji M. Angioleiomyoma: A clinicopathologic reappraisal of 562 cases. Cancer 1984;54:126-30. [Google Scholar] [PubMed]
- 6. Nielsen GP, et al. Leiomyoma of deep soft tissue: Clinicopathologic analysis of 36 cases. Am J Surg Pathol 1996;20:1075-80. [Google Scholar] [PubMed]
- 7. Daigeler A, et al. Leiomyoma of deep soft tissue: Diagnostic criteria and differential diagnosis. Pathol Res Pract 2007;203:531-5. [Google Scholar] [PubMed]
- 8. DiCaprio MR, Jokl P. Vascular leiomyoma presenting as medial joint line pain of the knee. Arthroscopy 2003;19:E24. [Google Scholar] [PubMed]
- 9. Kinoshita T, Ishii K, Abe Y, Naganuma H. Angiomyoma of the lower extremity: MR findings. Skeletal Radiol 1997;26:443-5. [Google Scholar] [PubMed]
- 10. D’Ambrosia R, Ferguson A. Leiomyoma of the foot: A case report. Foot Ankle 1991;12:121-4. [Google Scholar] [PubMed]
- 11. Sardanelli F, et al. MR imaging features of soft tissue leiomyomas. Radiol Med 1996;92:695-701. [Google Scholar] [PubMed]
- 12. Smith J, Kransdorf MJ. Imaging of benign soft tissue tumors. Semin Musculoskelet Radiol 2006;10:21-40. [Google Scholar] [PubMed]
- 13. Miettinen M, Fetsch JF. Evaluation of smooth muscle tumors using immunohistochemistry: SMA, desmin, h-caldesmon. Mod Pathol 2006;19 Suppl 2:S1-4. [Google Scholar] [PubMed]
- 14. Reith JD, Goldblum JR, Lyles RH, Weiss SW. Leiomyosarcoma of deep soft tissue: A clinicopathologic study of 41 cases. Am J Surg Pathol 2000;24:1435-42. [Google Scholar] [PubMed]
- 15. Dei Tos AP. Immunohistochemistry in sarcoma diagnosis: Practical considerations. Pathol Clin 2014;33:201-10. [Google Scholar] [PubMed]
- 16. Mohanty MK, Mishra S, Pradhan S. Leiomyoma of the foot: A rare entity. J Foot Ankle Surg 2016;55:855-8. [Google Scholar] [PubMed]
- 17. Berber O, et al. Deep soft tissue leiomyoma of the foot: A rare cause of heel pain. Foot 2010;20:43-5. [Google Scholar] [PubMed]
- 18. Lee CH, et al. Leiomyoma of the ankle: MR imaging appearance and histopathologic correlation. J Korean Radiol Soc 2000;43:1033-7. [Google Scholar] [PubMed]
- 19. Gajanthodi S, Rai R, Chaudhry RK. Vascular leiomyoma of foot. J Clin Diagn Res 2013;7:571-2. [Google Scholar] [PubMed]
- 20. Szolomayer LK, Talusan PG, Chan WF, Lindskog DM. Leiomyoma of the foot and ankle: A case series. Foot Ankle Spec 2017;10:270-3. [Google Scholar] [PubMed]
- 21. Jalgaonkar A, Mohan A, Dawson-Bowling S, Skinner J, Briggs TW. Deep soft tissue leiomyoma mimicking fibromatosis in a 5-year-old male. J Foot Ankle Surg 2012;51:110-3. [Google Scholar] [PubMed]
- 22. Lehtonen HJ. Hereditary leiomyomatosis and renal cell cancer: Update on clinical and molecular characteristics. Fam Cancer 2011;10:397-411. [Google Scholar] [PubMed]
- 23. Zaher A, Yasser J, Badaro D, Sekkach N. Unusual presentation of leiomyoma in the hindfoot. Case Rep Orthop 2024;2024:1217277. [Google Scholar] [PubMed]
- 24. Buddemeyer K, McKissack HM, Farnell C, Robin JX, Qarmali M, Basetty CR, et al. Leiomyoma of the foot: A case report. Cureus 2018;10:e3419. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Reviewers Acknowledgement & Photo Gallery September 2025
September 1, 2025 Reviewers Acknowledgement & Photo Gallery September 2025 November 10, 2016 Modified Tension – Slide Technique for Anatomical Distal Biceps Tenodesis using a Bicortical EndoButton and a Tenodesis Screw
November 10, 2016 Modified Tension – Slide Technique for Anatomical Distal Biceps Tenodesis using a Bicortical EndoButton and a Tenodesis Screw January 1, 2026 A Prospective Comparative Study of the Outcome of Diaphyseal Humeral Shaft Fractures with Anterior BridgePlating versus Open Reduction Internal Fixation by Dynamic Compression Plating
January 1, 2026 A Prospective Comparative Study of the Outcome of Diaphyseal Humeral Shaft Fractures with Anterior BridgePlating versus Open Reduction Internal Fixation by Dynamic Compression Plating February 1, 2026 Closed Traumatic Dislocation of 2nd–4th Metatarsophalangeal Joints with Associated 5th Metatarsal Base Fracture: A Rare Case Report
February 1, 2026 Closed Traumatic Dislocation of 2nd–4th Metatarsophalangeal Joints with Associated 5th Metatarsal Base Fracture: A Rare Case Report