
Giant cell tumor of bone poses a lifelong risk of recurrence, underscoring the need for continuous, long-term surveillance.
Eleni Karagergou, Department of Orthopaedic, Aristotle University of Thessaloniki, Georgios Papanikolaou Hospital, Thessaloniki, Greece. E-mail: krgeleni@gmail.com
Abstract
Introduction: Giant cell tumor of bone (GCTB), a benign but locally aggressive tumor, may rarely undergo malignant transformation and metastasize. Although local recurrence following surgical excision with intralesional curettage is fairly common and it usually occurs within the first 3–5 years post-operatively, a low-frequency occurrence has been observed after en block resections.
Case Report: A case of persistently recurrent GCTB of distal ulnar head is reported. The patient, who had undergone a Darrach procedure for excision of the tumor 40 years ago, presented with a recurrent mass at the same location. Shortly after excision of the lesion, she developed a new recurrence, which was not controlled with the monoclonal antibody denosumab, and required re-excision due to signs of ulnar nerve palsy.
Conclusion: The activation of a dormant GCTB, after 40 years of silence, illustrates the need for a long-term follow-up after surgery, even when no clear evidence of tumor relapse is clinically apparent. Considering the aggressive nature of the recurrent GCTB and its potential for malignant transformation and metastasis, our case is emphasizing the importance for frequent follow-up and lifelong surveillance.
Keywords: Giant cell tumor of bone, wrist, local recurrence, bone neoplasms, neoplasm metastasis.
Giant cell tumor of bone (GCTB) is a benign but locally aggressive tumor with a relatively low risk of malignant transformation and hematogenous metastases, targeting mainly the lungs [1]. It typically occurs in the metaphyseal/epiphyseal area of the affected bone and most commonly occurs around the knee joint [1]. The second most common site is the distal radius, while the distal ulna is a relatively rare location for GCTB [2]. The surgical treatment of choice is determined pre-operatively by fine needle bone biopsy and imaging scanning, which evaluates the intra- or extracompartmental extension of the lesion. Intralesional curettage and cavity filling with autografts/polymethylmethacrylate cement or en bloc resection are the main treatment options, depending on tumor extension, involvement of articular surfaces and available bone stock [3]. Local recurrences though can occur and the majority of them are usually seen within the first 3–5 years post-operatively [2,4]. Although intralesional curettage results in better functional outcome and faster recovery, it may lead to higher recurrence rates compared to en bloc resections. The latter have been associated with recurrence rates ranging from 0% to 5% [2,3,4,5].
We present a rare case of a dormant GCTB which was activated and recurred twice after 40 years of silence, in a patient who had en bloc resection of the primary tumor through a Darrach procedure in the distal ulna of her right wrist. Our case is highlighting the necessity for a lifetime follow-up of these tumors as their activation can occur at any time and it is associated with more aggressive disease.
A 59-year old female patient, with an old history of GCTB of distal ulna, presented with a mass at the same location, over the dorsal/ulnar aspect of her right wrist. According to the patient, she had en bloc resection along with excision of the ulnar head (Darrach procedure) 40 years ago, followed by re-excision and radiotherapy due to recurrence 12 months later. She was monitored for 5 years, and since there were no signs of recurrence, she was discharged. The histopathology reports of the primary and recurrent tumors were not available and the rest of her medical history was unremarkable.
On presentation, she reported that the mass rapidly grew over the past 7 months and complained about limited wrist movements and pain, which was worsening during activities. Clinically, there was a palpable, hard and tender mass over the distal dorso-ulnar aspect of the wrist and in proximity with the previous surgical scar. The neurological status of the hand and the blood supply were normal. Radiographic examination of the wrist showed a radiopaque lesion at the distal ulnar region with distinct borders but not in continuity with the existed from the previous operation distal ulnar stump (Fig. 1).

Figure 1: Radiograph of the wrist. A radiograph of the wrist shows a radiopaque lesion at the site of the previously excised ulnar head. The lesion has distinct borders and it is not in continuity with the ulnar stump.
Further radiologic examination with magnetic resonance imaging (MRI) and computed tomography (CT) scan revealed a bone mass with abnormal shape surrounded by soft tissue swelling. These findings raised the suspicion of recurrence of the old GCTB which was confirmed by a fine needle bone biopsy. Further investigation with chest and abdomen CT scans revealed no metastases.
En bloc surgical resection of the bone mass was carried out by the senior author through a longitudinal incision over the old scar. The tumor was extirpated and all the surrounding anatomical structures were recognized and preserved (Fig. 2).

Figure 2: Excision of the tumor. Marginal excision of the tumor, by preserving extensor carpi ulnaris, flexor carpi ulnaris, ulnar nerve and artery.
Histopathologic examination of the resected bone tumor confirmed the diagnosis of GCTB and the bone sample received from the distal ulnar stump was free of tumor cells. The patient had an uneventful recovery period and managed to gain a painless full range of wrist motion shortly after surgery.
One year later and although the patient was asymptomatic, a second recurrence of the tumor was identified on MRI. In an effort to shrink the tumor and control the disease, she started treatment with the monoclonal antibody denosumab; however, 6 months later, she developed signs of low ulnar nerve palsy. Compression of the nerve by the tumor was suspected and surgical re-excision along with release of the ulnar nerve and artery were performed, which were severely entrapped within the recurrent mass (Figs. 3 and 4).
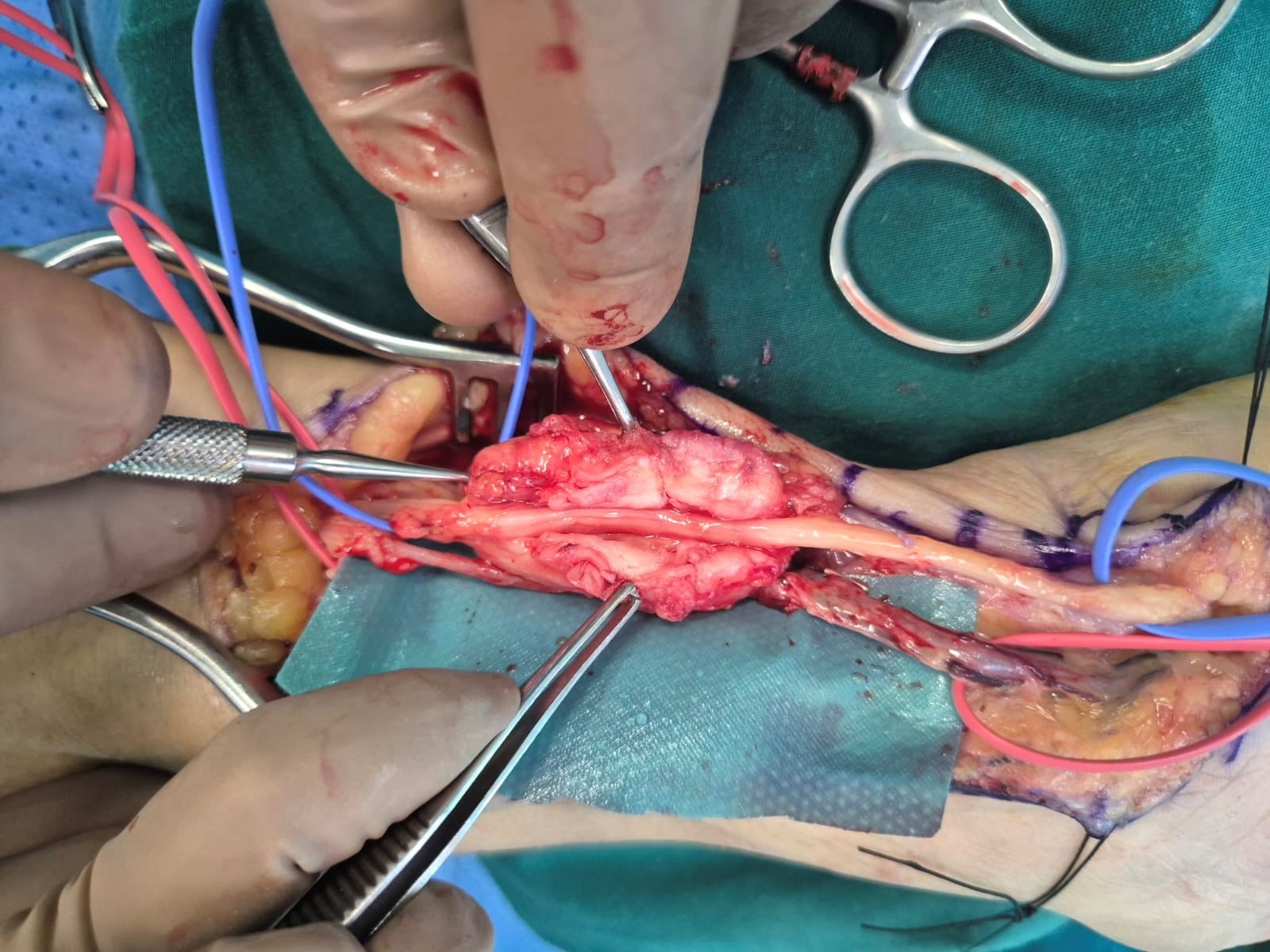
Figure 3: Ulnar nerve entrapment. Ulnar nerve entrapped within the recurrent tumor.

Figure 4: Preservation of ulnar nerve and artery. Dissection and preservation of ulnar artery and nerve after excision of the tumor.
The patient had an uneventful post-operative period and full recovery of the ulnar nerve palsy was observed 3 months later (Fig. 5). Up to date, 18 months following the re-excision of the tumor, she is free of macroscopic disease and remains on low dose of denosumab for local control of the disease.

Figure 5: Recovery of hand function. Clinical evidence of complete ulnar nerve recovery in the right hand.
We present a very rare case of GCTB recurrence after four decades of silence. The re-activation and local aggressiveness of the recurrent disease made its local control challenging. In a recently published systematic review, the mean interval between initial surgery and recurrence of GCTB was 23 months (range from 2 to 172 months), whether this was the first, second, or third recurrence of the tumor [3]. Cases of late relapse, such as those occurring 15 years after surgical treatment, have been reported very rarely [6]. Our case is unique due to the time interval of recurrence after 40 years of dormancy.
Recurrence rates of GCTB differ in various case series, depending on the method of primary treatment [2,4,5,7]. In a series of patients that received either intralesional curettage (n = 7) or en block resection (n = 21) for GCBT of distal ulna, the curettage group had a significantly higher recurrence rate (43% vs. 5%) [2]. However, even after wide excision of the tumor, local recurrences can occur. In a multicenter retrospective study among 205 patients who underwent en bloc resection for GCTB of the extremities and had adequate follow-up for more than 18 months, 29 of them presented with local recurrence [7]. In these cases, local recurrences are attributed to dormant tumor cells that remain in the soft tissues during excision and may be activated at any time. This is believed to account for the recurrence of GCTB in our patient, 40 years after excision of the primary tumor. This scenario is further supported from the fact that the tumor presented as a distinct entity and not in continuity with the distal ulnar stump, which was found to be free of disease.
Denosumab is a monoclonal antibody that targets receptor activator of nuclear factor kappa-b ligand (RANKL), a key molecule involved in the formation and activity of osteoclast-like giant cells found in GCTB [8]. By inhibiting RANKL, denosumab effectively reduces bone resorption and tumor progression, making it a valuable treatment option, especially for patients with unresectable tumors or those for whom surgery would cause significant morbidity. Its use has been shown to decrease tumor size and alleviate symptoms, facilitating less extensive surgery or, in some cases, serving as a standalone therapy [9]. In our case, we opted for treatment with denosumab for local control of the tumor. However, after 6 months of treatment, the tumor showed no signs of regression and its continued growth led to compression of the ulnar nerve, resulting in palsy and necessitating surgical re-excision.
Local recurrence of a GCTB after en bloc resection is associated with more aggressive behavior of the tumor. These tumors show some risk for potential malignant transformation to high-grade sarcomas [10]. Tsukamoto et al. [7] showed a 7% malignant transformation and mortality rate in patients with local recurrence after en bloc resection. In the same case series, there was a 35% distant metastasis rate. The majority had lung metastases and the median time from surgical excision of the recurrent tumor to distant metastasis was 10 months. Although these metastases look histologically as benign as the primary tumor and have a better prognosis than the metastases of frankly malignant lesions, strict adherence to a lifetime follow-up for both primary and recurrent tumors is required [11]. It should be pointed out that despite the benign cytologic characteristics of these tumors, their invasive behavior is more like that of a low-grade malignancy than of an active benign process [11]. Our described case provides good evidence that these tumors may stay dormant for a long time and they can give clinically evident recurrences even after 40 years.
No standard guidelines have been established regarding the frequency of patients’ follow-up visits. Hu et al. [5] recommend follow up every 3 months for the first 2 years, every 6 months for 3 years and every 12 months for 5 years. However, limiting the follow-up within the first 10 years is not safe as recurrences can occur at any time. We would recommend a lifetime follow-up, with more frequent radiographs within the first 5 year, when most of the recurrencies occur, then annually for the next 5 years and every few years thereafter. A simple radiograph of the involved site is an easy and effective diagnostic tool and it can accurately detect a local recurrence. Although late recurrence, as described in our case, is extremely rare, it can be lifesaving given the aggressive nature of these recurrent lesions.
Activation of a previously resected GCTB after a 40-year period of silence is rare and is associated with a more aggressive behavior of the tumor, given the second recurrence that shortly occurred after surgery. Although no standard guidelines exist, we recommend a frequent follow-up for the first 5 years and then every few years for a life-time.
This case report describes an unusual recurrence of a giant cell tumor of the distal ulna, 40 years after en bloc resection and Darrach procedure. It highlights the need for a lifetime follow-up, as these recurrent tumors are more aggressive and can show a potential to malignant transformation, metastasis, and recurrencies. Hence, frequent follow-up with a simple radiograph is recommended every few years.
References
- 1. Mendenhall WM, Zlotecki RA, Scarborough MT, Gibbs CP, Mendenhall NP. Giant cell tumor of bone. Am J Clin Oncol 2006;29:96-9. [Google Scholar] [PubMed]
- 2. Zhou L, Tang J, Shen L, Zhang Z, Yuan T. Giant cell tumors of the distal ulna: Long-term recurrence rate and functional outcomes of en bloc resection versus curettage in a multicenter study. J Orthop Surg Res 2023;18:743. [Google Scholar] [PubMed]
- 3. Pitsilos C, Givissis P, Papadopoulos P, Chalidis B. Treatment of recurrent giant cell tumor of bones: A systematic review. Cancers (Basel) 2023;15:3287. [Google Scholar] [PubMed]
- 4. Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am 1987;69:106-14. [Google Scholar] [PubMed]
- 5. Hu P, Zhao L, Zhang H, Yu X, Wang Z, Ye Z, et al. Recurrence rates and risk factors for primary giant cell tumors around the knee: A multicentre retrospective study in China. Sci Rep 2016;6:36332. [Google Scholar] [PubMed]
- 6. Amelio JM, Rockberg J, Hernandez RK, Sobocki P, Stryker S, Bach BA, et al. Population-based study of giant cell tumor of bone in Sweden (1983-2011). Cancer Epidemiol 2016;42:82-9. [Google Scholar] [PubMed]
- 7. Tsukamoto S, Mavrogenis AF, Hindiskere S, Honoki K, Kido A, Fujii H, et al. Outcome of reoperation for local recurrence following en bloc resection for bone giant cell tumor of the extremity. Curr Oncol 2022;29:6383-99. [Google Scholar] [PubMed]
- 8. Singh AS, Chawla NS, Chawla SP. Giant-cell tumor of bone: Treatment options and role of denosumab. Biologics 2015;14:69-74. [Google Scholar] [PubMed]
- 9. Vaishya R, Agarwal AK, Vijay V. ‘Salvage treatment’ of aggressive giant cell tumor of bones with denosumab. Cureus 2015;7:e291. [Google Scholar] [PubMed]
- 10. Bertoni F, Bacchini P, Staals EL. Malignancy in giant cell tumor of bone. Cancer 2003;97:2520-9. [Google Scholar] [PubMed]
- 11. Enneking WF. A system of staging musculoskeletal neoplasms. Clin Orthop Relat Res 1986;204:9-24. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Clinicoradiological Outcomes after Percutaneous Radiofrequency Ablation of Benign Bone Tumors: A Prospective Observational Study
June 1, 2026 Clinicoradiological Outcomes after Percutaneous Radiofrequency Ablation of Benign Bone Tumors: A Prospective Observational Study June 1, 2026 Acute Calcific Periarthritis of the 1st Metacarpophalangeal Joint: A Rare Diagnostic Challenge
June 1, 2026 Acute Calcific Periarthritis of the 1st Metacarpophalangeal Joint: A Rare Diagnostic Challenge February 1, 2026 A Rare Case: Septic Arthritis of The Wrist
February 1, 2026 A Rare Case: Septic Arthritis of The Wrist January 1, 2026 Combined Approach (Surgery + Systemic Adjuvant Therapy) in a Giant Cell Tumor of Proximal Femur: A Rare Case Report
January 1, 2026 Combined Approach (Surgery + Systemic Adjuvant Therapy) in a Giant Cell Tumor of Proximal Femur: A Rare Case Report