
The article shows that “no dressing” strategy in post-operative orthopedic cases allows faster discharge, reduces financial burden, and achieves similar surgical and functional outcomes as compared to the conventional dressing strategy.
Manish R Shah, Smt. B. K. Shah Medical Institute and Research Centre, Sumandeep Vidyapeeth Deemed to be University, Vadodara, Gujarat, India.. E-mail: manishshah2001in@yahoo.co.in
Abstract
Introduction: A wound is defined as any disruption in the continuity of the skin or the mucosal epithelial lining resulting from physical or thermal injury. Dressings play a crucial role in post-operative wound care, as they help clinicians establish an optimal environment for healing. Despite a comprehensive search, we could not find the guideline for the frequency of dressing change before the suture removal. Hence, we intend to study the result of the frequency of dressing change on wound healing. We hypothesized that there is no need to change dressing before suture removal. We aimed to study the results of the “no dressing” strategy for post-operative orthopedic cases and assess the surgical (healing by objective scale) and functional (satisfaction of the patient by subjective scales) outcomes of the study associated with the patients’ quality of life and financial burden.
Materials and Methods: A prospective and observational study was conducted over 18 months, involving 150 patients. Patients were randomly divided into two groups (75 each): Group A was the “no dressing” group, and Group B was the routine dressing group. Patients were assessed based on visual analogue scale (VAS), satisfaction score, and Stony Brook Scar Evaluation Scale. The final follow-up for this study was limited to 1 month after suture removal. However, all patients were on regular follow-up for the primary problem as required.
Results: We found a statistically significant improvement in functional VAS score (P = 0.0145) in the “no dressing” group. Hospitalization duration was significantly less with the “no dressing” strategy (P < 0.001). We found reduced financial burden for patients and hospitals by following the “no dressing” strategy. Other outcomes were similar to those of the routine dressing strategy.
Conclusion: We conclude that the “NO DRESSING” strategy is helpful in post-operative orthopedic cases. It allows faster discharge, similar surgical and functional outcomes, similar complication rates, and reduces financial burden for the patient and hospital. There is no difference in the time for suture removal and wound healing by following either strategy. However, a multi-centric study with larger groups may help to conclude better. Level of evidence: 3.
Keywords: Dressing materials, no-dressing strategy, stony brook scar evaluation scale, visual analogue scale, wound dressings.
Dressings act as a protective barrier, safeguarding the wound while the skin’s natural barrier is re-established. Furthermore, dressings aid in absorbing wound exudate, helping keep the area clean and dry and preventing bacterial contamination from the external environment [1]. Excessive exudate can undermine wound integrity, foster bacterial growth, and impede healing. This increases the risk of superficial wound infections and raises the likelihood of developing surgical site infections (SSIs), including deeper infections around implanted prosthetic devices.
Effective post-operative care is essential for optimal wound healing and successful surgical outcomes [2]. Certain dressings are specifically designed to create an optimal wound environment to enhance healing. For example, hydrogels provide moisture for dry wounds, hydrocolloids help to maintain hydration, and materials like alginates and foams are effective in absorbing excess exudate. We typically use sterile gauze, pads, and adhesive tape (such as Elastoplast) [3].
Surgical wound dressings applied at the time of surgery may be removed early, changed regularly, or retained until sutures or adhesive strips are taken out. However, frequent changes can be inconvenient for patients and burden the nursing staff, leading to increased overall healthcare costs. The operating theatre environment is the most sterile. In its comparison, the ward or dressing room environment may not be so sterile. In simulated wound environments, prolonged dressing use may trap moisture by promoting localized sweating and reducing evaporation. This moist environment can act as a nidus-a potential entry point for microorganisms-thereby heightening the risk of infection. Consequently, while delaying dressing removal has its benefits, there are also notable drawbacks. Despite these concerns, a comprehensive systematic review comparing early dressing removal (within 48 h post-surgery) with delayed dressing removal (after 48 h with interim dressing changes) in the realm of surgical wound care has yet to be conducted [4]. The 19th century marked a turning point with the introduction of antiseptic techniques and, later, antibiotics, drastically reducing wound infection rates and post-operative mortality. These changes laid the groundwork for modern aseptic surgical practices [4,5]. Boateng et al., 2008 believed that wounds should be exposed to air to “breathe” [6].
Post-surgical dressings protect the wound, reduce mechanical stress, absorb exudate, and provide a barrier against infection. Common post-operative dressing materials include adhesive films, absorbent pads, and semi-permeable membranes. Transparent dressings allow for visual monitoring without removal, reducing the risk of contamination during inspection [4,5,7]. Despite a comprehensive search, we were unable to find guidelines for the frequency of dressing changes before suture removal in post-operative orthopedic cases. Hence, we intend to study the result of the frequency of dressing change on wound healing. We hypothesized that there is no need to change dressing before suture removal. We studied the results of the “NO DRESSING” strategy in our series for post-operative orthopedic cases. Our objectives were to study the surgical and functional outcomes after the “NO DRESSING” strategy in post-operative orthopedic cases, complications of “NO DRESSING” in post-operative orthopedic cases, the improvement in the quality of life in patients, and to assess financial savings by the hospital and the patient.
After getting approval from the ethical committee, we conducted a prospective observational study on 150 patients (after obtaining written and informed consent) admitted to our tertiary care medical college from September 2023 to May 2025. The following formula was used to determine the sample size.
(S = Sample size, Z = Z score 95% (1.96), P = Population proportion (assumed as 50% or 0.5), n = Population (considered as 500), and M = Margin of error [0.05]).
All post-operative orthopedic cases involving patients aged 18 years or older were included in the study. Patients with open injuries, infectious conditions, revision surgeries, associated skin diseases (generalized and localized), aged <18 years, and those who refused to participate in this program were excluded. Patients were selected as per the above inclusion and exclusion criteria. Patients were randomly distributed into Group A, consisting of patients with the “NO DRESSING” strategy (75 cases), and Group B, consisting of the routine dressing strategy (75 cases). Randomization was done by patient enrolment for surgery on an odd and even basis with reference to the unique identification number (Indoor Patient Department number) that was randomly given by the computer (Hospital Management Software). It means the patient with an odd number was enrolled in group A and vice versa. This was changed on a daily basis (means on day 2, odd numbered patient goes to Group B and an even-numbered patient goes to group A). Indoor case window caters admissions from all the departments of the hospital. In all the patients, the wound was dressed with povidone iodine ointment and commercially available sterile gauze pieces and a sterile pad (5 mm). The study was done under the supervision of a senior professor in the department. All photographs were recorded.
In the “NO DRESSING” group (Group A), the dressing was done in the operating theatre under aseptic precautions, and patients were given intravenous antibiotics (Ceftriaxone + Amikacin for non-arthroplasty cases and Piparacillin and Tazobactam combination + Amikacin for arthroplasty cases) for 48 h. In total knee arthroplasty operated cases, the wound was covered with sterile gauze pieces and adhesive plaster. A compression bandage was applied for 48 h (Fig. 1).
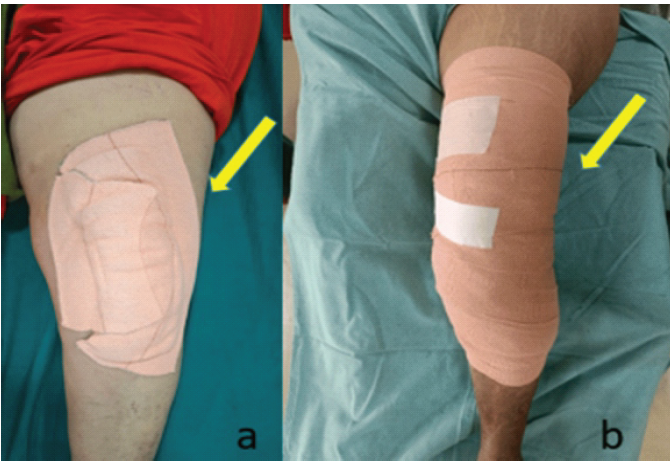
Figure 1: Dressing protocol after total knee replacement. (a) Showing coverage of the dressing with elastoplast (yellow arrow), (b) showing compressing bandage (yellow arrow).
The patient was mobilized as per the standard protocol. Tranexamic acid was used in total hip replacement and total knee replacement (TKR) cases. It was given 1 g preoperatively, 500 mg after closure of the wound, and 500 mg after 8 h on the day of surgery. Patients were usually discharged on post-operative day 3 or 4 (day of surgery considered post-operative day 0) with oral antibiotics (Cefixime 200 mg) for 10 days. Patients were monitored by mobile photos of the dressed area for soakage of the dressing as per the need. The dressing was changed if the dressing area (adhesive plaster) is soaked more than 50%, if the dressing is peeled off, if the dressing is contaminated by water, urine, or stool, or patient complained of fever and discharge. If the soakage was <50% (Fig. 2) of the dressing adhesive plast area, only that portion was covered with a sterile gauze piece (dressing was not opened).

Figure 2: The protocol if the soakage area is less. (a) soakage <25% of the dressing’s adhesive plast area after total knee replacement (yellow arrow), (b) area covered with a sterile gauze (yellow arrow).
The patients were called for suture removal between the 12th and 15th post-operative day, and suture removal was done as per wound healing. The wound healing was assessed by the surgical and functional outcome criteria by two different senior professors to ensure blinding 1 month after suture removal. No drains were inserted in any of the cases.
In Group B (routine dressing group), the dressing was changed on post-operative days 2 and 6. The rest of the post-operative protocol was the same as Group A. Time of suture removal, remarks about any future dressing requirements, and any complications (wound gaping or infection) were recorded at the time of suture removal. Surgical outcomes were measured by the Stony Brook Scar Evaluation Scale (SBSES) [8]. Functional outcomes measured by satisfaction score and Visual Analog Score (VAS) (Fig. 3) [9,10].
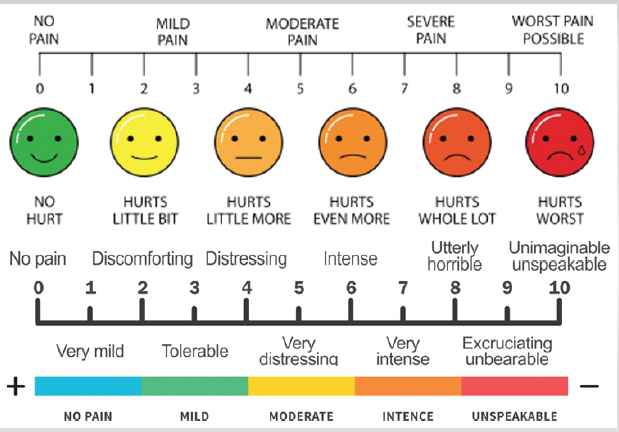
Figure 3: Visual Analog Score.
All data were recorded at each follow-up. The final follow-up for this study was limited to 1 month after suture removal. However, all patients were on regular follow-up for the primary problem as required. All participants were instructed to report immediately to the study team for any wound-related complications.
Statistical analysis
The statistical analysis in this study involving prospective data summarizes patient demographics and clinical parameters. All data were entered in Microsoft Excel and used for further analysis using the Statistical Package for the Social Sciences version 23. We presented the data in numbers and percentages. For Qualitative data generated during the study, we used the Chi-square test to find the association between the variables. The P < 0.05 was considered a statistically significant value.
We studied 150 post-operative orthopedic patients. We divided the patients into two groups: Group A, under the “NO DRESSING” strategy after the operation, and Group B, under the routine dressing study group. No patients were lost to follow-up. We found female predominance 41 (54.66%) in Group A and male predominance 50 (66.66%) in Group B. The 51–70 age group was the most common, 35 (46.66%) in Group A. Whereas in Group B, the 31–50 age group was common. Arthroplasty was more common in Group A, 31 (41.33%), compared with Group B, which had Lower limb trauma involving the majority of the patients, 28 (37.33%). Alcohol addiction was most common in both groups. We found a 50% reduction in the hospital stay (Mean + standard deviation = 3.91+1.2 days) in the “NO DRESSING” Group, as shown in (Table 1).
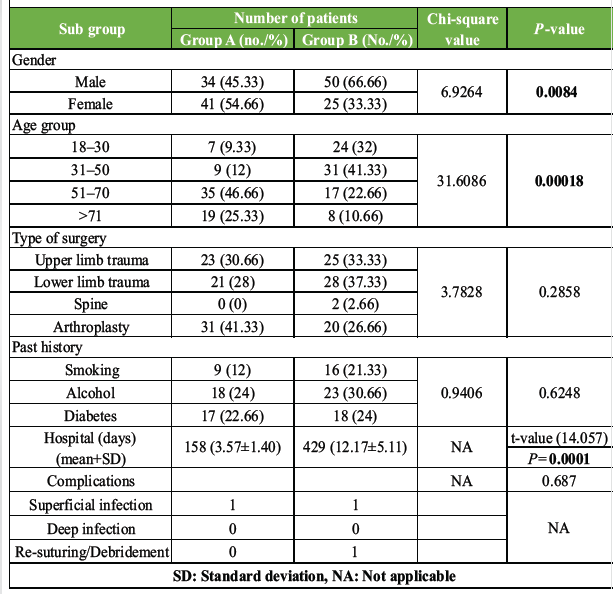
Table 1: Characteristics of the study population (statistical tests used: Chi-square test, t-test)
The SBSES, proposed by Singer et al., is a wound evaluation scale designed to measure the cosmetic effect of a wound, including the width, height, color, remaining suture marks, and an overall view of the scar [8]. Each index has a score of 0 or 1; the total is calculated, ranging from 0 (worst) to 5 (best). In our study, we found that the majority of patients, 110 (73.33%), had moderate results, as shown in (Table 2). Scores of 5 and 4 were considered excellent results, scores of 3 were considered good results, scores of 2 were considered fair results, and scores of 1 and 0 were considered poor results.
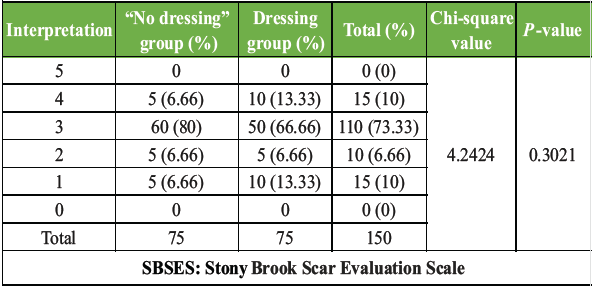
Table 2: SBSES (statistical test used: Chi-square test)
According to the SBSES score, the width of the scar (<2 mm), the color of the scar, and the suture mark were the criteria for assessment. In the majority of our cases, the width of the scar was >2 mm, the color was darker than the surrounding skin, and the suture marks were present. So, we found moderate results, 110 (73.33%), in the SBSES score. We evaluated the patients based on satisfaction scoring. We found a majority of patients with excellent results, 110 (73.33%), and only two patients with poor results (1.33%), as shown in (Table 3).
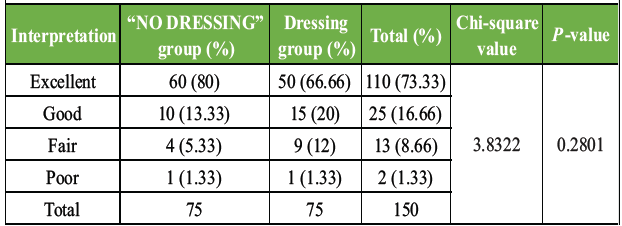
Table 3: Satisfaction score (statistical test used: Chi-square test)
Functional outcome was assessed by the VAS score. Excellent results, 120 (80%), were found in the majority of cases, as shown in (Table 4). Considering reduced hospital stay and dressing costs, the financial burden on the patient and the hospital is less in group A.
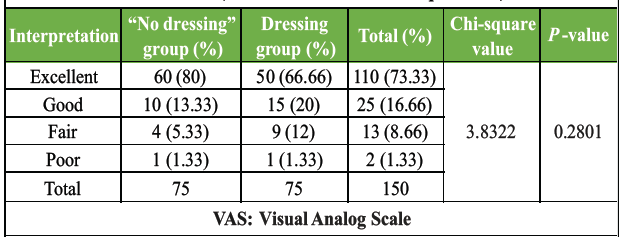
Table 4: VAS (statistical test used: Chi-square test)
We had one patient with a poor outcome in our study, who was operated on for TKR in the “NO DRESSING” group. She got a superficial stitch infection. However, the wound culture was negative. She was treated with dressings and antibiotics. She was cured in 3 weeks. We had one patient with a poor outcome in the routine dressing group who was operated on for TKR. She got a superficial stitch infection, and later she was treated with debridement. Her deep culture was found to be negative for microorganisms. She recovered with broad-spectrum antibiotics and dressings within 3 weeks.
The optimal frequency of dressing changes after surgical procedures, before suture removal, has been a subject of debate in clinical practice. While there is no universally accepted guideline, several studies investigated different types of dressing materials to determine their impact on wound healing and the patient. The overall purpose of these studies was to reduce the frequency of dressing, thereby reducing hospitalization duration and financial savings. As per our research, there are no studies that guide regarding the frequency of dressing or advocate for no dressing before suture removal.
Toon et al. compared delayed versus early dressing removal in their randomized controlled trial (RCT) [4]. They showed no complications even after the dressing was removed after 48 h. They studied clean, contaminated, and clean primary closures of the surgical wounds. They showed similar results in the early dressing removal group and the delayed dressing removal group. The hospital stay and total cost were less in the early dressing group. They commented regarding the need for low-risk bias RCTs for different types of surgery and levels of contamination.
Su et al. studied a new dressing system tailored for Total Knee Arthroplasty (TKA) surgical wounds [9]. This system aims to address the limitations of traditional gauze dressings, which often fail to provide adequate fixation and protection, leading to increased dressing changes and potential complications. They reported the VAS score of 0.92 + 0.67 at 1 month after the surgery. The SBSES score of their study at 1 month after surgery was 4.35 + 0.73. In their RCT, they showed better SBSES score with less number of dressings. However, there was no difference in the costs. The patient satisfaction was higher in the control group, which required less number of dressings.
Su et al. assessed newer dressings, including their flexibility, water resistance, and skin-friendliness, which facilitate early patient mobilization and reduce the risk of skin blistering [11]. These features contribute to enhanced patient comfort and potentially lower the risk of SSIs. They studied the VAS score and SBSES to evaluate the wound. They also reported better outcomes with less frequency of dressings and reduced hospitalization with their dressing material.
Lei et al. in their study of wound healing compared a conventional and a new dressing system for primary knee arthroplasty cases [12]. They showed 1.09 + 0.38 as the average number of changes of dressing. The average number of hospital stays in their study was 3.72 + 0.98 days. They reported no wound-related complications and a satisfaction score of 91.85 + 4.99% 1 month after surgery. They concluded that a smaller number of dressings do not have any adverse outcomes. Herndon et al. in their retrospective cohort study of 431 patients, compared polyester mesh adhesive dressing with silver-impregnated occlusive dressing in hip arthroplasty cases [13]. They reported better outcomes in relation to wound healing using mesh dressing, which was removed later, in comparison to the conventional dressing group.
Yuan et al. assessed the effect of different wound dressing materials used in the post-operative treatment of wounds after total hip arthroplasty and TKA [14]. They showed that active and interactive dressings had a significantly lower number of dressing changes (P < 0.001). They proved better results with a lower dressing frequency. Bredow et al. assessed the effect of absorbent versus conventional wound dressing in post-operative cases [15]. As per their study, patients in the intervention group (Mepilex-Border Post-operative) reported higher satisfaction levels (P < 0.001). They reported better VAS scores in the intervention group in comparison with the control group (routine dressing group), regardless of the type of surgery (hip, knee, or spine). Their purpose was to prove a lower frequency of dressing leading to similar outcomes with a special type of dressing.
Ubbink et al. assessed the effect of wound by occlusive versus conventional gauze dressing [16]. As per their study, the patients’ dressing costs 700 INR per dressing in occlusive dressing compared with the traditional gauze dressing costs 300 INR per dressing, but number of frequency of dressing is reduced in occlusive dressing compared to gauze dressing. They reported similar results with a gauze dressing, which is cheaper. Zhang et al. assessed the early and delayed removal of dressing in primary closure of clean and contaminated surgical wounds [17]. As per their study, there was no difference in the delayed removal of dressing in primary closure of clean wounds. So, the satisfaction score is higher in the early removal of the dressing group. Zarghooni et al. assessed modern versus conventional wound dressings in primary total knee and hip arthroplasty [18]. As per their study, there was a significant reduction in the total cost for dressing changes with the Mepilex dressings (P = 0.006) than the conventional dressing group. They kept the Mepilex dressing for 7 days. Their purpose was to prove that a lower frequency of dressing leads to similar outcomes.
Gromov et al. assessed that tissue adhesive for wound closure reduces immediate post-operative wound dressing changes after primary knee arthroplasty [19]. As per the study, the use of tissue adhesive as an adjunct to standard wound closure after primary TKA reduced the number of dressing changes after surgery, but did not change the appearance or healing of the wound. They showed that a lower dressing frequency does not affect wound healing and reduces costs. Liang et al. assessed the Impact of moist wound dressing on wound healing time [20]. As per their study, costs as well as dressing frequency were lower in moist wound dressing compared to traditional gauze dressing groups. They underscored the importance of a lower dressing change frequency with lower overall treatment cost.
In our study, we used conventional gauze dressing and an adhesive tape. We have not used any specialized dressing materials. We included all varieties of post-operative orthopedic cases, such as upper limb and lower limb trauma, arthroplasty, and spine surgery. Despite a thorough search in the database, we could not find a similar study. We compared our study with studies having similar parameters. Our results are comparable with the above studies in terms of reduced hospital stay, better SBSES score, VAS score, and reduced financial burden [9,11,12]. Our results are comparable with the above studies in terms of reduced hospital stay and reduced financial burden [4,13,16]. Other studies also demonstrate reduced financial burden with less frequent dressing [17,18,19,20].
Prospective nature of the study, randomized selection of patients, a large number, inclusion of all common varieties of orthopedic cases, and use of conventional gauze dressing can be considered strengths of our study. Single-center study can be considered a weakness of our study. Multi-center study with a larger number of patients may be more helpful.
We conclude that the “NO DRESSING” strategy is helpful in post-operative orthopedic cases in which we expect minimal chances of infection. It allows faster discharge, similar surgical and functional outcomes (in comparison with conventional dressing protocol), similar complication rates, and reduces financial burden for the patient and hospital. There is no difference in the time for suture removal and wound healing by following either strategy. However, a multi-centric study with larger groups may help to conclude better.
`No-dressing` strategy can be considered in post-operative orthopedic cases to reduce hospital stay and financial burden for the patient and the hospital. It gives similar results in terms of time for suture removal and wound healing.
References
- 1. Dhivya S, Padma VV, Santhini E. Wound dressings – a review. Biomedicine (Taipei) 2015;5:22. [Google Scholar] [PubMed]
- 2. Pickles S, McAllister E, McCullagh G, Nieroba TJ. Quality improvement evaluation of postoperative wound dressings in orthopaedic patients. Int J Orthop Trauma Nurs 2022;45:100922. [Google Scholar] [PubMed]
- 3. Dumville JC, Gray TA, Walter CJ, Sharp CA, Page T, Macefield R, et al. Dressings for the prevention of surgical site infection. Cochrane Database Syst Rev 2016;20:CD003091. [Google Scholar] [PubMed]
- 4. Toon CD, Lusuku C, Ramamoorthy R, Davidson BR, Gurusamy KS. Early versus delayed dressing removal after primary closure of clean and clean-contaminated surgical wounds. Cochrane Database Syst Rev 2015;2015:CD010259. [Google Scholar] [PubMed]
- 5. Queen D, Orsted H, Sanada H, Sussman G. A dressing history. Int Wound J 2004;1:59-77. [Google Scholar] [PubMed]
- 6. Boateng JS, Matthews KH, Stevens HN, Eccleston GM. Wound healing dressings and drug delivery systems: A review. J Pharm Sci 2008;97:2892-923. [Google Scholar] [PubMed]
- 7. Bhoyar SD, Malhotra K, Madke B. Dressing materials: A comprehensive review. J Cutan Aesthet Surg 2023;16:81-9. [Google Scholar] [PubMed]
- 8. Singer A, Arora B, Dagum A, Valentine S, Hollander JE. Development and validation of a novel scar evaluation scale. Plast Reconstr Surg 2007;120:1892-7. [Google Scholar] [PubMed]
- 9. Su S, He J, Wang C, Gao F, Zhong D, Lei P. A new dressing system reduces the number of dressing changes in the primary total knee arthroplasty: A randomized controlled trial. Front Surg 2022;9:800850. [Google Scholar] [PubMed]
- 10. Aun C, Lam YM, Collett B. Evaluation of the use of visual analogue scale in Chinese patients. Pain 1986;25:215-21. [Google Scholar] [PubMed]
- 11. Su S, Wang C, Gao F, Hu Y, Zhong D, Lei P. A waterproof, low-cost dressing system reduces postoperative wound dressing changes in primary total hip arthroplasty: An efficacy study. Front Surg 2022;9:966874. [Google Scholar] [PubMed]
- 12. Lei P, Gao F, Qi J, Li Z, Zhong D, Su S. A new dressing system for accelerating wound recovery after primary total knee arthroplasty: A feasibility study. BMC Surg 2024;15:112. [Google Scholar] [PubMed]
- 13. Herndon CL, Coury JR, Sarpong NO, Geller JA, Shah RP, Cooper HJ. Polyester mesh dressings reduce delayed wound healing rates after total hip arthroplasty compared with silver-impregnated occlusive dressings. Arthroplast Today 2020;6:158-62. [Google Scholar] [PubMed]
- 14. Yuan Y, Li J, Wang K, Zheng G, Chai S. The effect of different wound dressing materials used in postoperative treatment of wounds after total hip arthroplasty and total knee arthroplasty: A meta-analysis. Int Wound J 2022;19:2107-14. [Google Scholar] [PubMed]
- 15. Bredow J, Hoffmann K, Oppermann J, Hellmich M, Eysel P, Zarghooni K. Evaluation of absorbent versus conventional wound dressing. Dtsch Arztebl Int 2018;30:213-9. [Google Scholar] [PubMed]
- 16. Ubbink DT, Vermeulen H, Goossens A, Kelner RB, Schreuder SM, Lubbers MJ. Occlusive vs gauze dressings for local wound care in surgical patients: A randomized clinical trial. Arch Surg 2008;143:950-5. [Google Scholar] [PubMed]
- 17. Zhang T, Zhang F, Chen Z, Cheng X. Comparison of early and delayed removal of dressing following primary closure of clean and contaminated surgical wounds: A systematic review and meta-analysis of randomized controlled trials. Exp Ther Med 2020;19:3219-26. [Google Scholar] [PubMed]
- 18. Zarghooni K, Bredow J, Siewe J, Deutloff N, Meyer HS, Lohmann C. Is the use of modern versus conventional wound dressings warranted after primary knee and hip arthroplasty? Results of a prospective comparative study. Acta Orthop Belg 2015;81:768-75. [Google Scholar] [PubMed]
- 19. Gromov K, Troelsen A, Raaschou S, Sandhold H, Nielsen CS, Kehlet H, et al. Tissue adhesive for wound closure reduces immediate postoperative wound dressing changes after primary TKA: A randomized controlled study in simultaneous bilateral TKA. Clin Orthop Relat Res 2019;477:2032-8. [Google Scholar] [PubMed]
- 20. Liang Z, Lai P, Zhang J, Lai Q, He L. Impact of moist wound dressing on wound healing time: A meta-analysis. Int Wound J 2023;20:4410-21. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty
June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty May 1, 2026 Optimizing Post-operative Pain Management in Knee Arthroscopy: A Double-Blinded Randomized Controlled Trial of Regional Anesthesia with and without Local Infiltration
May 1, 2026 Optimizing Post-operative Pain Management in Knee Arthroscopy: A Double-Blinded Randomized Controlled Trial of Regional Anesthesia with and without Local Infiltration April 1, 2026 Functional and Radiological Outcome of Osteoporotic Vertebral Fracture Managed with Balloon Kyphoplasty – A Prospective Study
April 1, 2026 Functional and Radiological Outcome of Osteoporotic Vertebral Fracture Managed with Balloon Kyphoplasty – A Prospective Study August 6, 2024 Unilateral Traumatic Testicular Dislocation in a Patient of Pelvic Diastasis and Spine Fracture in an Adult: A Case Report and Review of Literature
August 6, 2024 Unilateral Traumatic Testicular Dislocation in a Patient of Pelvic Diastasis and Spine Fracture in an Adult: A Case Report and Review of Literature