
The tarsal bones are a rare location for aneurysmal bone cysts. Plain radiographs and magnetic resonance imaging, followed by a core/incisional biopsy, will help arrive at the diagnosis.
Dr. Purushotham Lingaiah, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: puru@aiimsmangalagiri.edu.in
Abstract
Introduction: Aneurysmal bone cyst (ABC) is a benign, locally aggressive lesion seen in the long bones and vertebrae. The tumour is rarely seen in the tarsal bones. Chronic pain and pathological fracture are often the presenting features. Radiographs and Magnetic Resonance Imaging is usually diagnostic and guides the management.
Case Report: We present a case of a 27-year-old male with chronic midfoot pain diagnosed as avascular necrosis of the lateral cuneiform, managed with biopsy needle decompression and platelet-rich plasma injection. The patient presented with persistent pain, and the workup revealed an ABC with a pathological fracture. The core biopsy report suggested ABC of the lateral cuneiform, which was later managed by excisional curettage and panlateral cuneiform arthrodesis using a tricortical iliac crest graft with a favourable outcome.
Conclusion: ABC in a long bone is a straightforward diagnosis due to its classical radiographic features. The diagnosis is challenging when presented in unusual locations. An incisional biopsy is the easiest way to confirm the histopathological diagnosis and aid in surgical planning.
Keywords: Aneurysmal bone cyst, cuneiform, biopsy, pathological fracture, arthrodesis.
An aneurysmal bone cyst (ABC) is an uncommon benign cystic tumor of bone that presents as a diffuse chronic pain, slow-growing swelling, and often a pathological fracture. It accounts for 1% of all bone tumors [1]. ABC is most commonly seen in long bones around the knee (>60%) and in vertebral bones (33%). Foot bones are rarely affected, accounting up to 5–9% of all lesions [2].
The rarity of ABC in bones of the foot makes it a diagnosis of low suspicion in the early stages [3]. A lytic lesion similar to an ABC-like giant cell tumor, tuberculosis poses diagnostic difficulty. Few case reports and series have documented the natural history of ABC in the foot and have stated that the symptomatology and treatment protocol are no different to ABC elsewhere in the body [4]. However, the benign nature, size, and slow expansion of the tumor lead to a delay in presentation and evaluation. The treatment strategies are standard and are based on size and local aggressiveness of the tumor [5]. These include curettage, curettage and bone grafting/cementation, excision, and extended curettage. We discuss the case of a young male who had presented with a chronic, persistent midfoot pain for 1 year. He was diagnosed with avascular necrosis (AVN) of the lateral cuneiform, treated with decompression and platelet-rich plasma (PRP) injection into the lesion. On re-evaluation, ABC of the lateral cuneiform bone was diagnosed using magnetic resonance imaging (MRI) and confirmed by histopathology. We highlight the radiological findings, surgical management, and expectant follow-up of this disease.
A 27-year-old adult male presented with a history of chronic left foot pain for 2 years and swelling in the dorsal aspect of the hind foot for 15 months. The pain was dull, aching and diffuse at onset, progressing to a more localized sharp pain at the center of the midfoot associated with gradually increasing swelling over the area. There was no history of trauma or constitutional symptoms. The pain had significantly limited the routine activities, including walking a small distance. The patient was diagnosed with AVN of the lateral cuneiform. Decompression with a biopsy needle and PRP were injected into the lesion. The patient was pain-free for 1 month and later developed sharp pain compelling him to use walker-assisted non-weight-bearing ambulation. The patient visited our center 1 year later. On examination, a small tender swelling was present on the dorsal and central aspects of the mid-foot distal to the navicular and proximal to the 3rd metatarsal bone. A crackling was felt at palpation, suggesting a possible pathological fracture. The foot and ankle movements were painful and restricted. There was no regional lymphadenopathy. The patient was evaluated with complete blood count, erythrocyte sedimentation rate, C-reactive protein, and a plain radiograph. The blood reports were within the normal range. The radiograph showed an expansile lytic lesion involving the entire lateral cuneiform bone (Fig. 1).

Figure 1: Plain X-ray anteroposterior and oblique views showing lytic expansile lesion in lateral cuneiform.
MRI was requested, which showed expansion and replacement of the lateral cuneiform bone by T1 heterogenous isointense, T2 short tau inversion recovery, and proton density fat saturation heterogenous hyperintense cystic lesion with internal septations. There are internal hypointense contents within the lesion suggestive of a bleed. Areas of cortical irregularity were noted anterior and posterior to the lesion due to pathological fracture (Figs. 2 and 3).
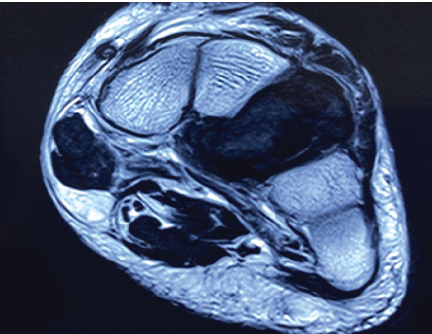
Figure 2: Magnetic resonance imaging axial view showing T1 heterogenous isointense lesion in the lateral cuneiform.
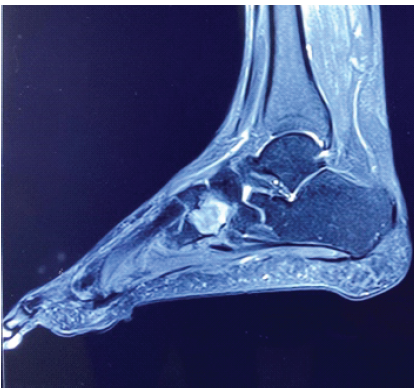
Figure 3: Magnetic resonance imaging sagittal view showing T2 hyperintense lesion with internal septations suggestive of bleed.
Based on these clinico-radiological features, ABC was diagnosed. A core biopsy was performed, which confirmed ABC. Surgical procedure – Under regional anaesthesia, the patient was put in the supine position. A dorsal midline 8 cm incision centering over the tumor was given. After careful dissection of soft tissues, tumor was exposed. The tumor was completely excised and treated with hydrogen peroxide solution. The cartilages of adjacent bones were curetted, and the gap was filled with an exactly measured tricortical iliac crest graft and fixed with a cortical screw from the cuboid to the middle cuneiform (Figs. 4 and 5). The cancellous graft was packed around the edges of the tricortical graft. The wound was closed, and the limb was immobilized in a plaster (Fig. 6). The tissue was sent for histopathology, which confirmed ABC.
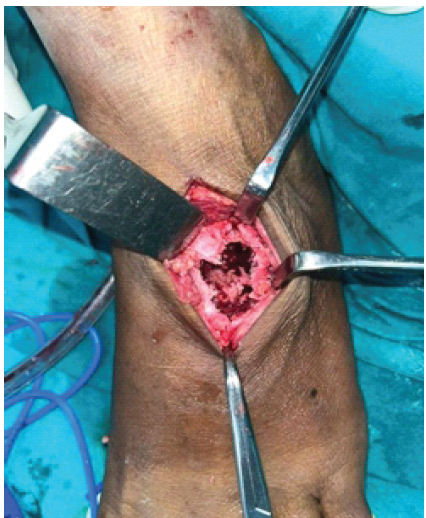
Figure 4: Tumor cavity after extended curettage showing complete loss of cartilage.

Figure 5: Tricortical graft filled in the cavity.
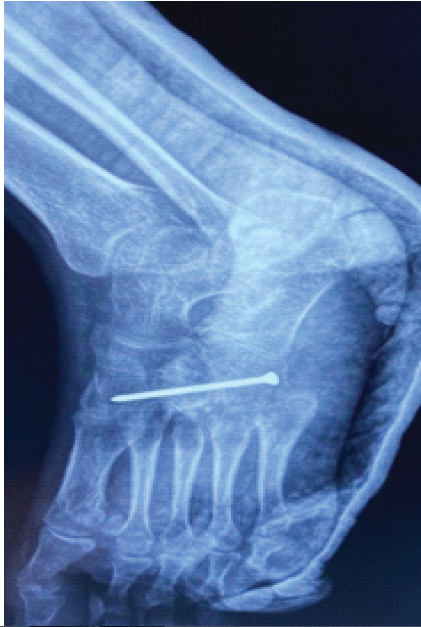
Figure 6: Post-operative X-ray showing arthrodesis.
Follow-up:
Postoperatively, follow-up was done at 2 weeks for suture removal and at 1, 3, 6 months, and 1 year. Weight-bearing was started after the pain and swelling had subsided at 3 months. Serial radiographs taken at each visit showed fused joints around the lateral cuneiform. The patient was able to walk pain-free and comfortably perform routine activities at 6 months. There were no signs of recurrence of symptoms/lesion at 3-year follow-up. The arthrodesis did not cause any functional impairment. The patient returned to his regular job.
ABC is a rare benign tumour-like lesion of bone usually seen in the metaphyseal region of long bones. It is commonly seen in the 2nd and 3rd decades of life with a slight female preponderance. Tibia is the most common affected bone, followed by the femur. The tumour may be seen occurring anywhere in the body, including vertebral bones and the sacrum. The foot is an unusual location for the tumour, and the presence of lytic lesions in the foot attracts a lot of differential diagnoses [1]. The exact mechanism of the pathogenesis of ABC is still not clear. ABC presents with other associated lesions in 50% of cases. The most accepted theory states a circulatory disturbance of the involved site resulting in a high venous pressure and dilated vessels [6]. It is stipulated that the associated lesions may cause these changes. The workup includes plain radiographs and imaging studies like computed tomography (CT) and MRI [7]. These are key to diagnosis and treatment. The radiographic features of ABC are quite distinct and aid in diagnosing the disease [8]. Conventional radiographs show an eccentric radiolucent lesion with expansile remodelling of bone. A thin surrounding rim of the periosteum and subperiosteal bone is usually present. CT delineates fluid levels and cortical breaches in addition. MRI is a better tool in assessing the lesion, as it provides additional information such as a characteristic solitary lucent high T1 or low T1 lesion, fluid-fluid levels, internal septations, eccentric location within the bone, cortical involvement, pathologic fracture, and aggressive periosteal reaction [6]. MRI adds clarity to the diagnosis by defining the size of the lesion, condition of surrounding soft tissue and aggressiveness of the lesion and guides a treatment plan. In cases where the lesion is confined within the margins of bony cortices, curettage with bone grafting/cementation provides a satisfactory result. In cases where the lesion has a cortical breach, as was seen in our case, the treatment plan should include extended curettage/excision. To avoid biomechanical stress to the surrounding bones and attain stability during walking, arthrodesis was done using a tricortical iliac crest bone graft. The diagnosis was a challenge in our case, as after the initial diagnosis of AVN with a surgical treatment done in an outside hospital, the evaluation had to be carefully done to avoid misdiagnosis. Clinico-radiological diagnosis of ABC was established first, followed by a core biopsy. Histopathology is the gold standard confirmation [9]. Minimally invasive techniques can be used to arrive at a diagnosis and accordingly plan the final treatment. Even with the strong suggestion of radiological features toward the presence of ABC, it is wise to perform a biopsy whenever feasible. Histopathology features in our case were consistent with ABC. A biopsy may still be indicated in extensive lesions posing a diagnostic dilemma. Long-term complications of ABC are rare [10]. Pathological fractures, malignant transformation, and local spread are possible. Recurrence is rare after surgery, possibly seen in cases with large lesions with soft-tissue extensions and conservative surgery. Long follow-up and monitoring are required for these cases.
The tarsal bones are a rare location for ABC. The dull aching nature of pain may lead to late presentation and treatment. Although most such lesions can be managed on standard terms of management of ABC, like simple curettage, curettage and bone grafting, and/or cementation, there is a risk of recurrence, especially when there is a pathological fracture. Extended excisional curettage and arthrodesis may be considered as a surgical option in such a case, as it not only offers total elimination of the lesion with no/negligible chance of recurrence but also provides a pain-free and stable locomotion. MRI, surgical option, and long-term follow-up are key features highlighted in this report on the management of ABC of the lateral cuneiform.
An aneurysmal bone cyst is rare in tarsal bones. The diagnosis, although made with radiographs and MRI, must be confirmed by biopsy before any surgical intervention. When completely excised, the recurrence rate is almost negligible.
References
- 1. Stevens KJ, Stevens JA. Aneurysmal bone cysts. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546654 [Google Scholar] [PubMed]
- 2. Shang J, Guo R, Zhan P, Chen C, Kan J, Liu H, et al. Aneurysmal bone cyst of the metatarsal: A case report. Oncol Lett 2016;12:2769-71. [Google Scholar] [PubMed]
- 3. Krishna M, Dayal S. Aneurysmal bone cyst: With uncommon location and presentation – a case series with review of literature. Clin Cancer Investig J 2020;9:267-70. [Google Scholar] [PubMed]
- 4. Shanmuganathan S, Singh SV, Vijayan S, Kulkarni MS. Solid aneurysmal bone cyst of cuboid: Rare location and diagnostic conundrum. BMJ Case Rep 2024;17:e258844. [Google Scholar] [PubMed]
- 5. Deventer N, Toporowski G, Gosheger G, De Vaal M, Luebben T, Budny T, et al. Aneurysmal bone cyst of the foot: A series of 10 cases. Foot Ankle Surg 2022;28:276-80. [Google Scholar] [PubMed]
- 6. Restrepo R, Zahrah D, Pelaez L, Temple HT, Murakami JW. Update on aneurysmal bone cyst: Pathophysiology, histology, imaging and treatment. Pediatr Radiol 2022;52:1601-14. [Google Scholar] [PubMed]
- 7. Gaillard F, Prasittimet K, Rasuli B, et al. Aneurysmal bone cyst. Available from: https://www.radiopaedia.org [Last accessed on 2025 Sep 18]. [Google Scholar] [PubMed]
- 8. Iltar S, Alemdaroğlu KB, Karalezli N, Irgit K, Caydere M, Aydoğan NH. A case of an aneurysmal bone cyst of a metatarsal: Review of the differential diagnosis and treatment options. J Foot Ankle Surg 2009;48:74-9. [Google Scholar] [PubMed]
- 9. Costa DD, Gabrielli E, Cerrone M, Di Gialleonardo E, Maccauro G, Vitiello R. Pathological fractures in aneurysmal bone cysts: A systematic review. J Clin Med 2024;13:2485. [Google Scholar] [PubMed]
- 10. Barnhart MD. Malignant transformation of an aneurysmal bone cyst in a dog. Vet Surg 2002;31:519-24. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes
June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes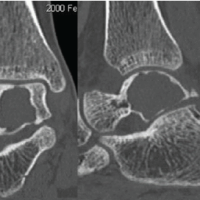 September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report November 1, 2024 Ipsilateral Fibula Grafting in a Case of Aneurysmal Bone Cyst in Tibia Diaphysis: A Case Report
November 1, 2024 Ipsilateral Fibula Grafting in a Case of Aneurysmal Bone Cyst in Tibia Diaphysis: A Case Report February 10, 2023 An Uncommon Case Report: Pathologic Fracture in a Proximal Femur Aneurysmal Bone Cyst in a Child
February 10, 2023 An Uncommon Case Report: Pathologic Fracture in a Proximal Femur Aneurysmal Bone Cyst in a Child