
Cementation performed after screw placement provides superior screw–cement interface strength compared to cementation before screw insertion.
Dr. Anirudh Dwajan, Department of Orthopaedics, AIIMS-Bilaspur, Himachal Pradesh, India. E-mail: anirudhdwajan@gmail.com
Abstract
Introduction: Cement augmentation is widely used in orthopedic trauma and reconstructive surgery to enhance fixation stability in compromised bone quality, including metastatic lesions, osteoporotic fractures, and segmental bone defects. However, the influence of cementation sequence on screw–cement interface mechanics remains unclear. The objective of this study was to evaluate and compare the effect of cementation sequence on the axial pull-out strength of cancellous screws in a standardized in vitro biomechanical model.
Materials and Methods: This in vitro biomechanical study compared the pull-out strength of 4-mm cancellous screws using two cementation techniques: Cementation after screw placement (Group 1) and cementation before screw placement (Group 2). Thirty-two samples were prepared using standardized wooden blocks, polymethylmethacrylate bone cement, and cancellous screws. Axial pull-out strength was measured using a universal testing machine.
Results: The mean pull-out strength was significantly higher in Group 1 (1700 N; standard deviation [SD] ± 282.84 N) compared with Group 2 (1450 N; SD ± 305.51 N) (P = 0.023).
Conclusion: Under controlled experimental conditions, cementation performed after screw placement demonstrated significantly higher pull-out strength compared with cementation before screw placement. These findings provide biomechanical insight into screw–cement interface behavior and may assist surgeons in optimizing cement augmentation techniques when stabilizing implants in structurally compromised bone. The results should not be directly extrapolated to complete in vivo fixation constructs.
Keywords: Bone cement, polymethylmethacrylate, cement augmentation, implant fixation, trauma reconstruction, biomechanics.
Cement augmentation is routinely employed in orthopedic practice to improve fixation stability in osseous defects arising from tumor surgery, trauma, or compromised bone quality. In bone tumor surgery, giant cell tumor (GCT) represents one of the most common indications for cement augmentation. Although classified as a benign lesion, GCT is locally aggressive and demonstrates a high recurrence potential, particularly in young adults between the second and 4th decades of life
Extended intralesional curettage remains the standard surgical treatment for most GCTs, with the dual objectives of achieving adequate tumor clearance and preserving joint function [2,3]. This procedure results in a residual bone cavity that requires structural reconstruction. While cancellous bone grafting remains biologically favorable, its limited availability in large defects has led to widespread use of polymethylmethacrylate (PMMA) bone cement [3,4]. PMMA provides immediate mechanical stability, facilitates early mobilization, and may contribute to local tumor control through thermal cytotoxic effects generated during polymerization [3,5].
In cases involving weight-bearing regions or substantial cortical deficiency, cement filling is frequently combined with internal fixation using plates and screws to enhance construct stability and reduce the risk of fracture or implant failure [5,6]. Despite the widespread adoption of cement-augmented fixation, variation exists in surgical technique, particularly regarding the timing of cement application relative to screw insertion. Some surgeons insert screws before cementation, whereas others place screws after cement has been introduced during its working phase [7,8,9,10]. These variations may influence screw–cement interface mechanics and overall fixation strength.
Cement augmentation is also widely applied in orthopedic trauma and reconstructive surgery, including fixation in metastatic bone disease, osteoporotic fractures, and large segmental bone defects. Understanding the biomechanical influence of cementation sequence may therefore have important clinical implications in optimizing implant stability in compromised bone.
The present study was designed as a controlled biomechanical experiment to isolate screw–cement interface behavior. The objective was to evaluate and compare the axial pull-out strength of cancellous screws when cementation was performed before versus after screw placement under in vitro conditions. Pull-out strength was selected as a reproducible biomechanical parameter representing resistance to axial tensile loading at the screw–cement interface. The findings are intended to provide objective mechanical insight into the cementation sequence while acknowledging the limitations of an experimental laboratory model.
This in vitro biomechanical study was conducted at a tertiary care hospital between June 2023 and June 2024. The study protocol was reviewed and approved by the Institute Ethics and Scientific Committee (IEC) (IEC No.: JIP/IEC/2022/0261; Approval Date: July 07, 2022), and a waiver of informed consent was granted, as this was a laboratory-based biomechanical study without the use of human or animal tissue.
Study design and sample preparation
A total of 32 samples were prepared and divided into two groups of 16 specimens each:
Group 1: Cementation after screw placement
Group 2: Cementation before screw placement.
Uniform wooden blocks measuring 5 × 3 × 3 cm were used as the base material to provide a reproducible testing substrate. All blocks were obtained from the same batch and prepared with uniform grain orientation to minimize variability in internal density and structural anisotropy. Specimens were randomly allocated to the two experimental groups to distribute any residual material variability evenly between groups. The use of wooden blocks allowed standardized screw placement while minimizing variability related to bone density and trabecular microarchitecture, thereby enabling controlled comparison of cementation sequence effects on screw–cement interface mechanics (Fig. 1).
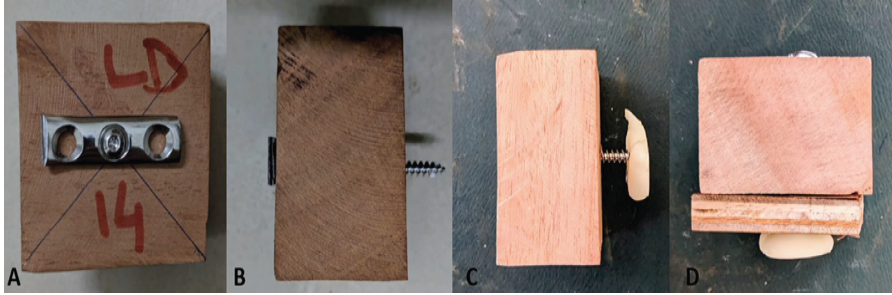
Figure 1: Preparation of the experimental construct showing (a) wooden block–screw construct, (b) block–screw construct without screw guide before bone cement placement, (c) block–screw construct after cementation, and (d) block–screw construct with screw guide used for centering the 4-mm cancellous screw.
Pilot holes were created using a 2.7-mm drill bit. To ensure an identical screw entry point and alignment across all specimens, a 3.5-mm locking plate with a drill sleeve was used as a centering guide. The holes were subsequently tapped using a 3.5-mm cortical tap to create standardized threads capable of engaging the screw. A 4-mm × 50-mm fully threaded, non-cannulated cancellous screw was inserted into each block using a calibrated torque-limiting screwdriver set to an identical torque value for all specimens. Screw insertion depth was standardized by advancing each screw until 4–5 threads were uniformly visible beyond the block surface, which served as a consistent visual endpoint and ensured comparable thread engagement length across all samples.
For Group 1, the wooden block–screw construct was placed within a cylindrical mold with a 4-cm internal diameter. PMMA bone cement (Subiton Quirurgico ) was prepared according to the manufacturer’s instructions and injected into the mold using a cement gun, ensuring controlled and consistent circumferential cement application around the screw.
For Group 2, bone cement was first introduced into the mold during its working phase, following which the wooden block–screw construct was centrally inserted into the cement mass, simulating cementation before screw placement. In both groups, care was taken to maintain consistent positioning of the construct within the mold.
Biomechanical testing
After preparation, all samples were allowed to set for 48 h at room temperature to permit complete cement polymerization. Biomechanical testing was then performed using a universal testing machine. A custom-made stainless-steel fixture was employed to ensure consistent specimen positioning, precise alignment of the screw–cement construct with the loading axis, and reproducible application of force. Axial pull-out testing was conducted by applying a purely unidirectional tensile load parallel to the long axis of the screw until failure, thereby measuring maximum pull-out strength under controlled conditions (Fig. 2).

Figure 2: Universal testing machine setup used for axial pull-out testing, showing (a) the overall testing apparatus and (b) the cement–screw construct mounted and aligned for application of axial tensile load.
Outcome measure
The primary outcome measure was pull-out strength, defined as the maximum axial force (N) required to completely extract the screw from the cement–wood construct. Pull-out strength was used as a standardized biomechanical parameter reflecting resistance to axial tensile forces at the screw–cement interface.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences Statistics version 21.0 (IBM Corp., Armonk, NY, USA). Pull-out strength values were expressed as mean ± standard deviation (SD). Data normality was assessed using visual inspection of histograms and the Shapiro–Wilk test. As the data were normally distributed, comparisons between the two groups were performed using the independent samples Student’s t-test. A P < 0.05 was considered statistically significant.
The biomechanical analysis demonstrated a statistically significant difference in axial pull-out strength between the two cementation techniques evaluated.
Specimens in Group 1 (cementation after screw placement) demonstrated higher pull-out strength values compared with Group 2 (cementation before screw placement). The mean pull-out strength in Group 1 was 1700 N (SD ± 282.84 N), with a 95% confidence interval of 1549.28 N–1850.72 N. The median pull-out strength in this group was 1800.00 N, with observed values ranging from 1200.00 N to 2200.00 N.
In contrast, Group 2 showed a lower mean pull-out strength of 1450.00 N (SD ± 305.51 N), with a 95% confidence interval of 1287.21 N–1612.79 N. The median pull-out strength in this group was 1400.00 N, and values ranged from 1000.00 N to 2200.00 N (Table 1).
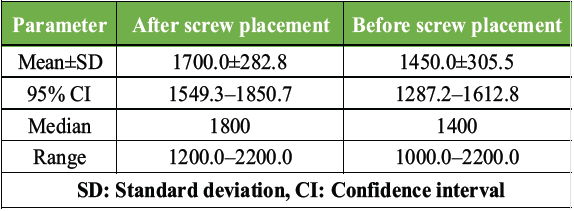
Table 1: Descriptive statistics of pull-out strength in groups
The distribution of pull-out strength values for both groups is illustrated in the box-and-whisker plot (Fig. 3).
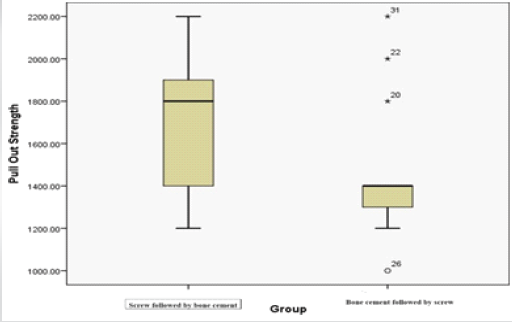
Figure 3: The distribution of pull-out strength values for both groups is illustrated in the Box-and-Whisker plot.
The mean difference in pull-out strength between the two groups was 250.00 N, with a 95% confidence interval of 37.43 N–462.57 N. This difference was statistically significant using an independent samples Student’s t-test (P = 0.023) (Table 2), indicating greater resistance to axial pull-out at the screw–cement interface when cementation was performed after screw placement.
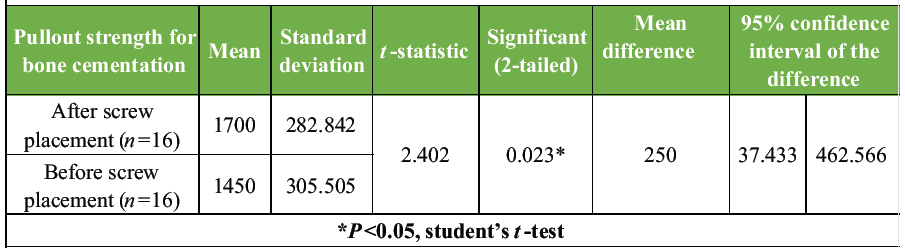
Table 2: Independent samples t-test comparing pull-out strength between groups
Variability within the two groups was comparable, as reflected by similar SD values. No outlier measurements requiring exclusion were identified.
Bone cement augmentation is widely employed to enhance the mechanical performance of screw fixation by improving load transfer at the screw–cement interface. PMMA remains the most commonly used bone cement in orthopedic surgery because of its favorable handling characteristics and ability to provide immediate mechanical stability. The resistance of cement-augmented screws to axial extraction is influenced by multiple factors, including cement viscosity, timing of screw insertion, and the quality of interfacial contact between cement and screw threads. Previous experimental and finite element studies have demonstrated that interface mechanics and loading direction play a critical role in determining failure loads, with reduced resistance observed as applied forces deviate from the longitudinal axis of the screw [1,2,3].
Multiple biomechanical investigations have shown that cement augmentation significantly improves screw pull-out strength compared with unaugmented fixation, particularly in substrates with reduced structural integrity [11,12,13]. In addition to cement presence, prior studies have emphasized that cement handling characteristics, including timing of insertion and degree of polymerization, can influence mechanical performance [14,15,16]. Variations in screw design, such as thread geometry and surface characteristics, have also been shown to affect pull-out behavior in cement-augmented systems. Collectively, these findings highlight that fixation strength in cement-augmented constructs is sensitive to both material properties and surgical technique.
Despite the existing literature on cement-augmented fixation, comparative data specifically evaluating the influence of cementation sequence on screw pull-out strength under standardized conditions remain limited. The present study demonstrated that cementation performed after screw placement resulted in significantly higher axial pull-out strength compared with cementation performed before screw placement in a controlled in vitro model. This finding suggests that allowing cement to polymerize around pre-positioned screw threads may enhance mechanical interlocking at the interface, thereby increasing resistance to axial extraction. Conversely, inserting screws into cement during its working phase may disrupt cement continuity around the threads, potentially reducing effective interfacial contact.
These findings may assist trauma and reconstructive surgeons in optimizing cement augmentation techniques when stabilizing implants in structurally compromised bone, including metastatic lesions, osteoporotic fractures, and large segmental bone defects.
It is important to emphasize that the observed differences reflect isolated screw–cement interface behavior rather than the performance of complete fixation constructs. A standardized substrate was used to ensure uniform mechanical properties across all specimens, minimizing variability related to material heterogeneity. This enabled controlled evaluation of the primary study variable—cementation sequence—by isolating screw–cement interface behavior under reproducible conditions. Such reductionist models are widely used in biomechanical research to facilitate consistent comparison between techniques and generate reliable baseline data.
The experimental design intentionally employed a simplified construct to allow focused comparison while limiting confounding factors inherent to biological tissues. Although factors, such as bone–cement interdigitation, multi-screw interactions, implant configuration, and complex in vivo loading conditions were not incorporated, the model provides valuable insight into interface-level mechanical behavior under axial loading.
Pull-out strength is a reproducible and widely accepted parameter for assessing resistance to axial tensile forces at the screw–cement interface, providing a standardized basis for comparison between fixation techniques. Within this controlled setting, cementation performed after screw placement demonstrated significantly higher pull-out strength, likely due to enhanced mechanical interlocking between cement and screw threads. These findings may have practical relevance in compromised bone conditions, where optimization of the cementation technique can influence fixation stability. Further evaluation in more representative biomechanical and clinical models is warranted.
Limitations
This study utilized a standardized experimental model designed to enable controlled comparison of cementation sequence; therefore, direct extrapolation to clinical scenarios should be interpreted within this context. Biological factors, such as bone heterogeneity, cement–bone interdigitation, and remodeling were not incorporated. The use of a single screw design may limit generalizability across implant types. Testing was confined to static axial pull-out loading, without inclusion of multidirectional or cyclic forces encountered in vivo. In addition, the long-term effects of cement aging were not assessed.
This in vitro biomechanical study demonstrated that cementation performed after screw placement resulted in significantly higher axial pull-out strength compared with cementation performed before screw placement under controlled experimental conditions. The observed difference likely reflects variations in screw–cement interface mechanics related to cementation sequence and suggests that allowing cement to polymerize around pre-positioned screw threads may enhance mechanical interlocking at the interface.
These findings provide biomechanical insight that may assist trauma and reconstructive surgeons in understanding factors influencing cement-augmented screw fixation in structurally compromised bone. However, the results represent isolated interface behavior and should not be directly extrapolated to complete fixation constructs or clinical outcomes. Clinical application must consider additional variables, including bone quality, implant configuration, loading conditions, and overall surgical context. Further investigations incorporating more representative fixation constructs and clinical correlation are necessary to determine the in vivo relevance of these biomechanical observations.
Cementation performed after screw placement may provide superior screw–cement interface strength compared with cementation before screw insertion, and may be considered when optimizing fixation in structurally compromised bone.
References
- 1. Raskin KA, Schwab JH, Mankin HJ, Springfield DS, Hornicek FJ. Giant cell tumor of bone. J Am Acad Orthop Surg 2013;21:118-26. [Google Scholar] [PubMed]
- 2. Saikia KC, Bhattacharyya TD, Bhuyan SK, Bordoloi B, Durgia B, Ahmed F. Treatment of giant cell tumor of bone: Current concepts. Indian J Orthop 2011;45:101-7. [Google Scholar] [PubMed]
- 3. Kivioja AH, Blomqvist C, Hietaniemi K, Trovik C, Walloe A, Bauer HC, et al. Cement is recommended in intralesional surgery of giant cell tumors: A Scandinavian Sarcoma Group study of 294 patients followed for a median time of 5 years. Acta Orthop 2008;79:86-93. [Google Scholar] [PubMed]
- 4. Prosser GH, Baloch KG, Tillman RM, Carter SR, Grimer RJ. Does curettage without adjuvant therapy provide low recurrence rates in giant-cell tumors of bone? Clin Orthop Relat Res 2005;435:211-8. [Google Scholar] [PubMed]
- 5. Persson BM, Ekelund L, Lovdahl R, Gunterberg B. Favourable results of acrylic cementation for giant cell tumors. Acta Orthop Scand 1984;55:209-14. [Google Scholar] [PubMed]
- 6. Wouters HW. Giant cell tumors: Treatment with curettage and acrylic cement. Ned Tijdschr Geneeskd 1974;118:987-93. [Google Scholar] [PubMed]
- 7. Backley P, Dunstan E, Athanasou NA. Pathological fracture through a giant cell tumor of bone treated by curettage, cementation and plate fixation. J Bone Joint Surg Br 1999;81:450-2. [Google Scholar] [PubMed]
- 8. Zheng X, Hu Y, Zhang Y. Effect of bone cement augmentation on screw fixation in uncontained tibial defects – A finite element analysis. Med Imaging (Bellingham) 2024;3:171. [Google Scholar] [PubMed]
- 9. Zhao Y, Zhang Q, Zhao D, Zhang Y, Wang W. Biomechanical comparison of different fixation methods for uncontained tibial plateau defects. J Orthop Surg Res 2020;15:533. [Google Scholar] [PubMed]
- 10. Elder BD, Lo SF, Holmes C, Goodwin CR, Kosztowski TA, Lina IA, et al. The biomechanics of pedicle screw augmentation with cement. Spine J 2015;15:1432-45. [Google Scholar] [PubMed]
- 11. Juvonen T, Nuutinen JP, Koistinen AP, Kroger H, Lappalainen R. Biomechanical evaluation of bone screw fixation with a novel bone cement. Biomed Eng Online 2015;14:74. [Google Scholar] [PubMed]
- 12. Wu ZX, Gao MX, Sang HX, Ma ZS, Cui G, Zhang Y, et al. Surgical treatment of the osteoporotic spine with bone cement-augmented cannulated pedicle screws. Spine J 2015;15:1222-9. [Google Scholar] [PubMed]
- 13. Song Z, Zhou Q, Jin X, Zhang J. Cement-augmented pedicle screw for thoracolumbar degenerative diseases with osteoporosis: A systematic review and meta-analysis. J Orthop Surg Res 2023;18:631. [Google Scholar] [PubMed]
- 14. Iamthanaporn K, Aonsong W, Tuntarattanapong P, Yuenyongviwat V. Screw inserting in different phase of cement affect the pull-out strength of cement augmented screws. Orthop Traumatol Surg Res 2022;108:103060. [Google Scholar] [PubMed]
- 15. Flahiff CM, Gober GA, Nicholas RW. Pullout strength of fixation screws from polymethylmethacrylate bone cement. Biomaterials 1995;16:533-6. [Google Scholar] [PubMed]
- 16. Christodoulou E, Chinthakunta S, Reddy D, Khalil S, Apostolou T, Drees P, et al. Mechanical and geometric analysis of fenestration design for cement-augmented pedicle screws. Int J Spine Surg 2022;16:714-23. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures
May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures September 1, 2025 Total Hip Arthroplasty with Cage Application for Complex Posterior Hip Dislocation and Acetabular Fracture in a Patient with Prior Patellectomy: A Case Report
September 1, 2025 Total Hip Arthroplasty with Cage Application for Complex Posterior Hip Dislocation and Acetabular Fracture in a Patient with Prior Patellectomy: A Case Report August 6, 2024 Hemodynamic Effects of Bone Cement Implantation in Hip Arthroplasty: Insights from a Prospective Study in Eastern India
August 6, 2024 Hemodynamic Effects of Bone Cement Implantation in Hip Arthroplasty: Insights from a Prospective Study in Eastern India June 10, 2023 A Case Report of Giant Aneurysmal Bone Cyst of Distal Tibia with a Non-healing Fungating Mass and its Management in a 30-year-old Male
June 10, 2023 A Case Report of Giant Aneurysmal Bone Cyst of Distal Tibia with a Non-healing Fungating Mass and its Management in a 30-year-old Male