
To identify carpal instability following post traumatic wrist injury. Follow up of patient at regular intervals in the post-operative period to promptly identify and treat carpal instability to prevent morbidity.
Dr. Vishnu Senthil,
Department of Orthopaedics, No. 112, NBQ AC Hostel, Kasturba Medical College, Manipal – 576 104, Karnataka, India.
E-mail: vishsnake@gmail.com
Introduction: Carpal instability is broad category consisting of various patterns of injury, with dissociative type more common.
Case Report: A 13-year-old boy presented at 6 months following a fall with restriction of wrist movements. Patient had sustained a closed distal one-third both bones fracture forearm fixed with K-wire, and volar lunate instability was found during sequential follow-up.
Conclusion: Posttraumatic carpal instability should be identified at the earliest to avoid poor hand function and morbidity associated with it.
Keywords: Volar intercalated segment instability, posttraumatic, distal radius fracture.
Carpal instability and its biomechanics have always been evolving due to the advancement in the field of radiology and arthroscopy. Lunate plays a pivotal role and acts like an intercalated segment in carpal stability, loss of anchorage of this key structure cause intercalated segment instability. Volar intercalated segment instability is a less common manifestation of dissociative carpal instability. We report of a case of post traumatic acute static volar instability.
13‑year‑boy had sustained distal one‑third radius and ulna fracture after fall on an outstretched hand. Open reduction and K‑wire fixation was performed for both bone fracture forearm (Fig. 1). Implants were removed after 4 weeks (Fig. 2).

He noticed restriction of dorsiflexion of wrist, while other movements normal. Serial X‑rays showed a loss of normal alignment of radio‑lunate in comparison with the opposite (Fig. 3, 4).
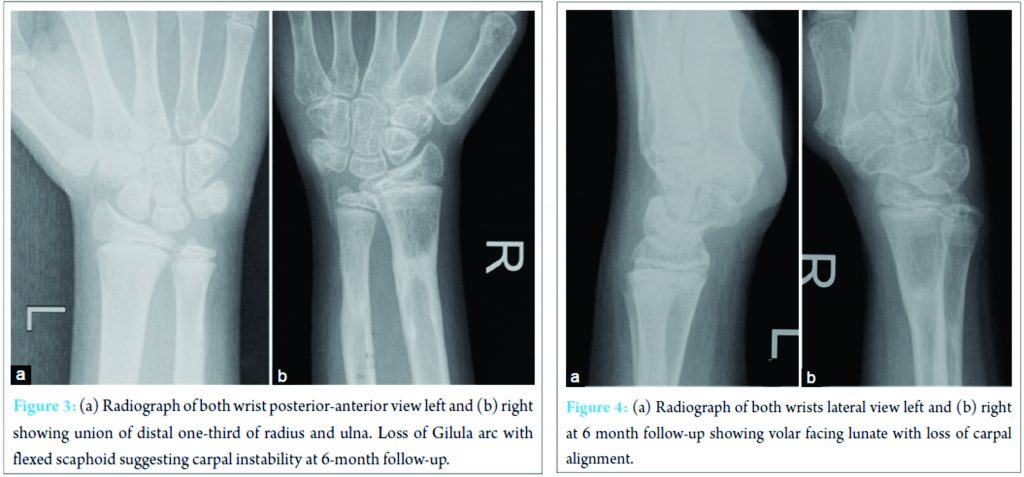
Initial X‑ray showed normal alignment of carpus before reduction. Serial radiographs during follow‑up showed a volar facing lunate with alteration of scapholunate and lunatocapitate angle and was diagnosed with a volar intercalated lunate instability (Fig. 5). The patient was put on strict rehabilitation protocol and the dorsiflexion improved from 0‑10° to 0‑40°. At 1 year follow‑up patient is still having restriction of dorsiflexion (Fig. 6) with volar lunate instability (Fig. 5). The patient is being planned for further procedure.

Carpal instability should be considered as a differential in patients presenting with chronic wrist pain and restricted movements following trauma. Reagan et al. classified carpal instability into four categories and lunato‑triquetral ligament is involved in stage three which leads to volar lunate instability [1]. Lunate instability is further divided into static or dynamic and acute or chronic. VISI is a condition in which there is pathologic volar flexion of the lunate, with or without a similar posture of the other proximal row carpal bones. Palmar flexion instability is less commonly recognized [1]. VISI is commonly seen in rheumatoid arthritis. Lunato‑triquetral ligament attrition due to congenital ligamentous laxity causes VISI. Posttraumatic volar lunate instability is an entity that can be missed during the initial traumatic event because of its subtle nature [2]. Posttraumatic carpal stability diagnosed at the earliest avoids advanced surgical procedures such as reconstruction and fusion of joint [3]. Earlier management prevents functional morbidity of wrist. Lunate instability in plain radiograph can be diagnosed with the alteration of various angles namely the loss of scapholunate angle, loss of alignment between the lunate, capitate and radius and increase in the capitolunate angle. Treatment options include from closed reduction and K‑wire fixation, dorsal capsulodesis, tenodesis, arthroscopic or open repair with reconstruction and finally arthrodesis [4]. Few cases have been reported in literature [5]. VISI is a missed injury in our case associated distal radius and ulna fracture [6]. This injury could be subtle in nature before reduction and fixation that led to delay in diagnosis or iatrogenic in nature after reduction of the fracture.
Wrist function is a complex interaction of various biomechanics involving the carpal bones, ligaments and the distal radio-ulnar complex. Awareness of carpal instability associated with fractures or injuries around the wrist is needed by the treating surgeon to avoid delay in diagnosis and treatment.
To suspect volar intercalated segment instability following a wrist injury and also following reduction with k wire fixation. Follow up of patient at regular intervals to prevent morbidity due to this deformity.
References
- 1. Reagan DS, Linscheid RL, Dobyns JH. Lunotriquetral sprains. J Hand Surg Am 1984;9(4):502‑514. [Google Scholar] [PubMed]
- 2. Chantelot C. Post‑traumatic carpal instability. Orthop Traumatol Surg Res 2014;100 1 Suppl:S45‑S53. [Google Scholar] [PubMed]
- 3. Garcia‑Elias M. The treatment of wrist instability. J Bone Joint Surg Br 1997;79(4):684‑690. [Google Scholar] [PubMed]
- 4. Muminagic S, Kapidzic T. Wrist instability after injury. Mater Sociomed 2012;24(2):121‑124. [Google Scholar] [PubMed]
- 5. Panagopoulous A, Allom R, Compson J. Acute static volar intercalated segment instability (VISI) of the wrist: A case report. J Med Diagn Methods 2013;2(3):1‑3. [Google Scholar] [PubMed]
- 6. Brown IW. Volar intercalary carpal instability following a seemingly innocent wrist fracture. J Hand Surg Br 1987;12(1):54‑56. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2023 Rare Case of Chronic Unreduced Shoulder Dislocation: A Case Report and Literature Review
July 10, 2023 Rare Case of Chronic Unreduced Shoulder Dislocation: A Case Report and Literature Review November 1, 2025 Enchondroma of Hands: A Surgical Dilemma and Our Experience
November 1, 2025 Enchondroma of Hands: A Surgical Dilemma and Our Experience March 1, 2025 Femoral Shortening Osteotomy in Managing Congenital Patellar Dislocation: A Case Report and Review of Literature
March 1, 2025 Femoral Shortening Osteotomy in Managing Congenital Patellar Dislocation: A Case Report and Review of Literature August 1, 2025 Acute Carpal Tunnel Syndrome: Is It Only Wrist Fractures? A Case Series Report and Literature Review
August 1, 2025 Acute Carpal Tunnel Syndrome: Is It Only Wrist Fractures? A Case Series Report and Literature Review