
Fracture neck femur can occur in a healthy child without any significant injury and without any underlying secondary cause.
Dr. Lakshay Garg, Department of Orthopaedics, All India Institute of Medical Sciences, Patna, Bihar, India. E-mail: lakshay.garg0710@gmail.com
Introduction: Bilateral femoral neck fracture in children is uncommon and is extremely rare in the absence of significant injury or any underlying systemic and local bone disease. Diagnosis in these healthy children is usually delayed due to the presence of mild symptoms and lack of suspicion for a fracture.
Case Report: We report a case of 13-year-old girl with a bilateral neck of femur fracture without any history of trauma or any underlying systemic or local disease. The child presented to us 6 months after the onset of symptoms and was managed by osteosynthesis and valgus intertrochanteric osteotomy. The fractures on both sides healed satisfactorily without any evidence of avascular necrosis of the femoral head. However, nonunion of the intertrochanteric osteotomy was observed on the left side. It was subsequently managed by open reduction and bone grafting and healed satisfactorily thereafter. The relevant literature about this rare case has been discussed.
Conclusion: Management of late presenting fractured neck femur is more complex and often needs more invasive procedures. Besides, it is known to increase the risk of complications and compromise the treatment outcome. Hence, it is important to realize the possibility of a fracture neck femur in an otherwise normal child and such children should be evaluated and treated at the earliest for a better outcome.
Keywords: Bilateral, children, femoral neck fracture, pediatric, non-union, valgus osteotomy.
Fracture neck femur is less common in adolescents and is usually associated with high-energy trauma [1]. Association with a low-velocity injury is extremely rare and has been reported occasionally in military personals and those involved in sports activities [2]. Few cases of spontaneous fracture neck femur at a younger age have been reported due to underlying pathological conditions of bone or as a result of underlying metabolic disorder [3]. A bilateral, non-traumatic fracture neck femur in an adolescent without any underlying cause is extremely rare with only a few cases reported in the literature [4,5]. Hereby, we report a case of a 13-year-old girl who did not sustain any significant injury but presented to us with bilateral hip pain for 6 months. On further evaluation, a bilateral fracture neck femur was diagnosed without any underlying cause. Furthermore, the management of this case and relevant literature has been discussed.
A 13-year-old girl presented to the outpatient department with intermittent pain in both hip joints for 6 months. Pain aggravated on prolonged walking and got relieved with rest and occasionally radiated to the inner thighs and knee. She had consulted a physician for hip pain and was prescribed symptomatic treatment without any further investigations. Since then, she was on intermittent painkillers but was able to do all the routine activities of daily life. The patient neither gave a history of any significant trauma nor of any underlying comorbidity that can affect bone metabolism. There were no obvious risk factors for the fracture too. Except for intermittent use of pain-relieving medications, she was not on any other medications and was not actively involved in any sports. Medical history, family history, and personal history were unremarkable. The build was normal for her age with a body mass index of 23.4 (normal range: 18.5–24.9). On clinical evaluation, the patient had a bilateral Trendelenburg gait with mild discomfort. The movements of both hips were painless and normal in range (flexion: 0–120°, extension: 0–10°, adduction: 0–30°, abduction: 0–40°, internal rotation: 0–30°, and external rotation: 0–30°) with no tenderness. There was no fixed deformity or limb length discrepancy and both limbs had normal neurovascular status. The laboratory tests that were conducted in the hospital did not reveal any significant abnormality except for a mild Vitamin D deficiency (Table 1).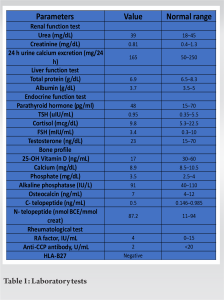 The patient had normal rheumatological, metabolic, and endocrine workup. A radiograph of the pelvis with both hips showed a Delbet type II fracture neck of the femur with preserved neck length on both sides (Fig. 1).
The patient had normal rheumatological, metabolic, and endocrine workup. A radiograph of the pelvis with both hips showed a Delbet type II fracture neck of the femur with preserved neck length on both sides (Fig. 1).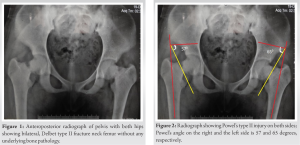 There was varus angulation on both sides but no significant translation of the fragments. Neck shaft angles on the right and left sides were 98° and 99°, respectively; while Powel’s angles on the right and left sides were 57° and 65°, respectively (Fig. 2).
There was varus angulation on both sides but no significant translation of the fragments. Neck shaft angles on the right and left sides were 98° and 99°, respectively; while Powel’s angles on the right and left sides were 57° and 65°, respectively (Fig. 2). 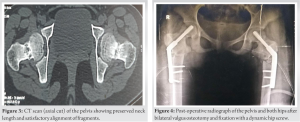 Computed tomogram (CT) scan of both hips confirmed a preserved neck length and alignment of fragments (Fig. 3). A diagnosis of bilateral stress fracture of the neck femur was made. Magnetic resonance imaging of both hips was done and the presence of osteonecrosis of the femoral head was ruled out. Under combined spinal and epidural anesthesia, the patient was taken on a traction table on both sides and both sides were operated in the same sitting, left followed by right. The fracture was reduced satisfactorily by a closed maneuver. However, as Powel’s angle was high on both sides, valgus osteotomy was planned at the sub-trochanteric level with an aim of getting 30° corrections in Powel’s angle on both sides. A guide wire was passed across the fracture from the lateral cortex of the trochanter at an angle of 100° to the long axis of the femur. Fixation of the fracture was done with a 9.5 mm dynamic hip screw (DHS). Thereafter, valgus sub-trochanteric osteotomy was performed on both sides and fixation was done with a 130° side plate (Fig. 4).
Computed tomogram (CT) scan of both hips confirmed a preserved neck length and alignment of fragments (Fig. 3). A diagnosis of bilateral stress fracture of the neck femur was made. Magnetic resonance imaging of both hips was done and the presence of osteonecrosis of the femoral head was ruled out. Under combined spinal and epidural anesthesia, the patient was taken on a traction table on both sides and both sides were operated in the same sitting, left followed by right. The fracture was reduced satisfactorily by a closed maneuver. However, as Powel’s angle was high on both sides, valgus osteotomy was planned at the sub-trochanteric level with an aim of getting 30° corrections in Powel’s angle on both sides. A guide wire was passed across the fracture from the lateral cortex of the trochanter at an angle of 100° to the long axis of the femur. Fixation of the fracture was done with a 9.5 mm dynamic hip screw (DHS). Thereafter, valgus sub-trochanteric osteotomy was performed on both sides and fixation was done with a 130° side plate (Fig. 4).  She remained non-weight bearing for 12 weeks. However, range of movement and strengthening exercises was started as soon as the patient was pain-free after surgery. The neck fractures on both sides as well as osteotomy on the right side healed satisfactorily. However, the osteotomy site on the left side revealed signs of nonunion at 10 months follow-up (Fig. 5).
She remained non-weight bearing for 12 weeks. However, range of movement and strengthening exercises was started as soon as the patient was pain-free after surgery. The neck fractures on both sides as well as osteotomy on the right side healed satisfactorily. However, the osteotomy site on the left side revealed signs of nonunion at 10 months follow-up (Fig. 5).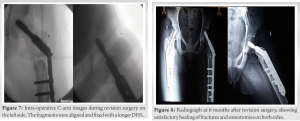 Parents were counseled for revision surgery but they did not agree and presented at 12 months after surgery with implant failure (Fig. 6). Patient underwent revision surgery and intraoperatively, the proximal fragment was found to be completely displaced and rotated in flexion. The previous implant was removed, the nonunion was reduced, fixation was done with a longer DHS, and an autologous bone graft was added (Fig. 7). Further post-operative period was uneventful and the nonunion healed satisfactorily within 6 months of revision surgery (Fig. 8).
Parents were counseled for revision surgery but they did not agree and presented at 12 months after surgery with implant failure (Fig. 6). Patient underwent revision surgery and intraoperatively, the proximal fragment was found to be completely displaced and rotated in flexion. The previous implant was removed, the nonunion was reduced, fixation was done with a longer DHS, and an autologous bone graft was added (Fig. 7). Further post-operative period was uneventful and the nonunion healed satisfactorily within 6 months of revision surgery (Fig. 8).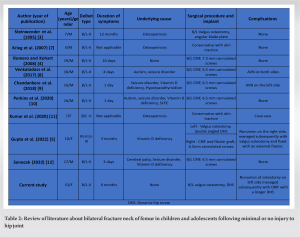
Simultaneous bilateral fracture neck of the femur in children and adolescents is rare and it usually results from a high-energy trauma like a fall from height or road traffic accident [6]. The current patient did not have any history of significant injury around the hip. The only complaint was mild pain in both hips and a limp while walking for 6 months. Due to this, a medical consult was not sought and diagnosis was delayed. Simultaneous bilateral femur neck fracture in the absence of significant trauma is extremely rare in children. Unlike the elderly population where osteoporosis is a common cause, children usually have an underlying metabolic bone disease rendering them vulnerable to break with trivial trauma (Table 2) [3,4,5,7,8,9,10,11,12]. Steinwender et al. reported a case of benign osteopetrosis in a 7-year-old boy who was asymptomatic till a bilateral femoral neck fracture occurred [3]. An association has also been reported with seizure disorders secondary to hypocalcemia, autism, cerebral palsy, and electroconvulsive therapy [8,9,10,12]. The muscle contractions during an epileptic episode can produce excessive rotational stress, thereby producing bilateral neck femur fractures. In addition, long-term use of certain antiepileptic drugs can lead to hypocalcemia and a resultant osteopenia. Severe Vitamin D deficiency and hyperparathyroidism were observed as a cause in other case reports [9,10]. Moreover, resultant hypocalcemia secondary to severe Vitamin D deficiency is known to initiate epileptic episodes in otherwise normal children [9,10]. Thus, a bilateral femoral neck fracture in children can be secondary to a wide range of underlying disorders and it is highly recommended to evaluate them thoroughly if there is no history of significant trauma. However, few cases of bilateral femoral neck fracture in an otherwise healthy adolescent without any underlying cause have been reported [4,13]. Gupta et al. reported only a subclinical Vitamin D deficiency in his case report [5]. The patient in the present study did not have any medical comorbidity and was not on any medication. She was not involved in any sport or high-demand activity as well. Her relevant laboratory investigations did not reveal any significant abnormality except a subclinical Vitamin D deficiency. Thus, the occurrence of femoral neck fracture in a healthy child is a fair possibility and hence all children presenting with hip pain should be evaluated thoroughly even if there is no history of substantial trauma or a medical comorbidity. This will ensure an early diagnosis and treatment, thereby a good treatment outcome. Treatment of femoral neck fracture in children is controversial in many aspects [14]. Due to the rare incidence, there is a scarcity of literature about the management of atraumatic bilateral femoral neck fractures in children. Most of the studies have suggested treatment for a traumatic injury in an acute setting. Overall, closed reduction and percutaneous fixation with cancellous cannulated screws are preferred for an injury presenting within 1 month [6,8,9,10]. Open reduction has been recommended where closed reduction fails and the addition of primary intertrochanteric valgus osteotomy has been suggested for Powel’s type II and type III injuries. For those presenting after 1 month of injury, the intertrochanteric valgus osteotomy is recommended after the fracture has been reduced and fixed satisfactorily [5,14]. It converts the shear forces across the fracture site into compressive forces, thereby enhancing union. This is especially advised for cases with a concomitant coxa vara deformity and those having a higher Powel’s angle. Addition of a fibular strut graft is advised in cases of neck resorption or comminution. The present case had Powel’s type II injury on both sides and even though the exact time of occurrence of the fracture was not known, she had symptoms for 6 months before diagnosis. Furthermore, the radiographs and CT scan images did not reveal neck resorption or comminution. Hence, close reduction and osteosynthesis along with a valgus osteotomy were preferred over osteosynthesis alone. This was in agreement with the reports of Steinwender et al. and Gupta et al. Complications after surgical management of such fractures have been reported. Bilateral avascular necrosis of the femoral head was observed by Venkatadass et al., 6 months after the closed reduction and screw fixation [8]. Similarly, Chandankere et al. reported avascular necrosis on the left side after surgical intervention [9]. Both cases had displaced Delbet type II fracture and were operated after a delay of more than 24 h. Nonunion of fracture was reported on the right side by Gupta et al. after closed reduction, screw fixation, and fibular strut grafting [5]. This also was a displaced type II fracture and was operated 3 months after the onset of symptoms. The left-sided fracture of the same patient which was managed by valgus osteotomy healed without any complication. In the current case, nonunion of the intertrochanteric osteotomy was observed on the left side. On further analysis, the proximal fragment was found to be flexed, without any contact with the distal fragment. This could have occurred while putting the DHS on the left side and was missed intraoperatively. In the left proximal femur, the clockwise movement of a screw in the proximal fragment can displace the proximal fragment into flexion. One needs to be aware of this possibility and should confirm good alignment and contact of fragments in both the coronal and sagittal plane during surgery. The current case underwent revision on the left side. The fragments were reduced and bone graft was added and the nonunion healed satisfactorily thereafter.
Pediatric bilateral fracture neck femur in the absence of significant injury or any underlying cause is extremely rare. However, this possibility cannot be denied and such children complaining of pain in the groin or thigh should be evaluated properly to have an early diagnosis. Significant delay in treatment can lead to complications and may compromise the treatment outcome. Neglected fractures and nonunions are effectively managed by valgus intertrochanteric osteotomy and osteosynthesis. Care should be taken to properly align the fragments during fixation as the proximal fragment is vulnerable to displacement while putting the lag screw.
A fracture neck femur remains a rare possibility in children presenting with hip pain without a history of significant trauma or any underlying cause. Such children should be thoroughly evaluated to reach an early diagnosis and to obtain good functional outcomes after surgical intervention.
References
- 1.Ratliff AH. Fractures of the neck of the femur in children. J Bone Joint Surg Br 1962;44-B:528-42. [Google Scholar | PubMed]
- 2.Pongsamakthai W, Sangkomkamhang T. Bilateral displaced femoral neck stress fractures treated with valgus subtrochanteric osteotomy: A case report and two-year follow-up. J Clin Orthop Trauma 2021;22:101575. [Google Scholar | PubMed]
- 3.Steinwender G, Hosny GA, Koch S, Grill F. Bilateral nonunited femoral neck fracture in a child with osteopetrosis. J Pediatr Orthop B 1995;4:213-5. [Google Scholar | PubMed]
- 4.Romero AN, Kohart SR. 19-year-old male adolescent with bilateral femoral neck stress fractures: A case report. Mil Med 2008;173:711-3. [Google Scholar | PubMed]
- 5.Gupta AK, Narang A, Gupta S, Kanojia RK. Bilateral neck of femur fracture in a child with underlying Vitamin D deficiency: A case report on management and 10-year follow-up. Cureus 2022;14:e22953. [Google Scholar | PubMed]
- 6.Naik P, Mantri N, Tank P, Bhesaniya R. Bilateral fracture neck femur in child with bilateral delayed union and bilateral AVN: A rare occurrence and literature review. Indian J Orthop 2021;55:501-7. [Google Scholar | PubMed]
- 7.Krieg AH, Speth BM, Won HY, Brook PD. Conservative management of bilateral femoral neck fractures in a child with autosomal dominant osteopetrosis. Arch Orthop Trauma Surg 2007;127:967-70. [Google Scholar | PubMed]
- 8.Venkatadass K, Avinash M, Rajasekaran S. Bilateral avascular necrosis of the femoral head following asynchronous postictal femoral neck fractures: A case report and review of the literature. J Pediatr Orthop B 2018;27:274-8. [Google Scholar | PubMed]
- 9.Chandankere V, Mulpur P, Maryada VR, Pendyala SR, Annapareddy GV. Simultaneous bilateral neck of femur fractures in an adolescent secondary to hypocalcaemic seizure. J Pediatr Orthop B 2019;28:491-4. [Google Scholar | PubMed]
- 10.Perkins CA, Alexeev M, Schrader T. Bilateral femoral neck fractures in the setting of bilateral slipped capital femoral epiphysis: A case report. JBJS Case Connect 2020;10:e1900561. [Google Scholar | PubMed]
- 11.Kumar S, Dhammi IK, Shahi P, Zafar A. Paediatric bilateral femoral neck fractures in osteopetrosis treated conservatively. BMJ Case Rep 2020;13:e236891. [Google Scholar | PubMed]
- 12.Senocak E. Spontaneous bilateral femur neck fracture secondary to grand mal seizure: A case report. World J Clin Cases 2022;10:11111-5. [Google Scholar | PubMed]
- 13.Khadabadi NA, Patil KS. Simultaneous bilateral femoral neck stress fracture in a young stone mason. Case Rep Orthop 2015;2015:306246. [Google Scholar | PubMed]
- 14.Pandey RA, John B. Current controversies in management of fracture neck femur in children: A review. J Clin Orthop Trauma 2020;11(Suppl 5):S799-806. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2024 Femoral Neck Fracture Non-Union: Treatment with Bone Marrow Concentrate, Demineralized Bone Matrix, and Morselized Allograft and Angular Stable Fixation. Report of 2 Cases
November 1, 2024 Femoral Neck Fracture Non-Union: Treatment with Bone Marrow Concentrate, Demineralized Bone Matrix, and Morselized Allograft and Angular Stable Fixation. Report of 2 Cases July 10, 2024 Bilateral Anterior Cruciate Ligament Reconstruction with All-Inside Technique for Adolescent: A Review of the Literature and Case Report
July 10, 2024 Bilateral Anterior Cruciate Ligament Reconstruction with All-Inside Technique for Adolescent: A Review of the Literature and Case Report May 10, 2019 Hybrid Fixation in Pediatric Forearm Fractures, does it Predispose to Non-union? A Case Report and Literature Review
May 10, 2019 Hybrid Fixation in Pediatric Forearm Fractures, does it Predispose to Non-union? A Case Report and Literature Review February 1, 2026 Proximal Hamate Autograft in Non-union Proximal Scaphoid Fractures, A Novel Technique – A Case Report
February 1, 2026 Proximal Hamate Autograft in Non-union Proximal Scaphoid Fractures, A Novel Technique – A Case Report