
Scapular pseudo-winging can be caused by ventral osteochondromas, necessitating thorough evaluation and appropriate management.
Dr. Aditya Seth, Department of Orthopaedics, Sunshine Hospitals, Hyderabad, Telangana, India. E-mail: adiseth1702@gmail.com
Introduction: Scapular pseudo-winging caused by ventral osteochondromas is a rare condition that has been reported in only a handful of cases. This case report describes a 21-year-old male patient with scapular pseudo-winging due to ventral osteochondromas of the scapula. This report adds to the limited literature on this topic and highlights the importance of considering ventral osteochondromas as a possible cause of scapular pseudo-winging.
Case Report: A 21-year-old male presented with a swelling on his left upper back that had gradually increased in size over the past 10 years. Physical examination revealed a bony hard swelling arising from the medial border of the scapula, with associated scapular pseudo-winging. Diagnostic imaging confirmed the presence of two ventral osteochondromas located on the body of the scapula. Surgical excision was performed to address the patient’s cosmetic concerns.
Conclusion: This case report highlights the importance of considering ventral osteochondromas as a possible cause of scapular pseudo-winging. It contributes to the existing literature by documenting a rare presentation and providing insights into the clinical course, diagnostic imaging, and surgical management of this condition. By raising awareness among tumor surgeons and orthopedic surgeons, this report may aid in early recognition and appropriate management of scapular pseudo-winging cases caused by ventral osteochondromas. Furthermore, this report expands our understanding of the etiology and treatment options for scapular pseudo-winging, potentially benefiting patients across various clinical specialties.
Keywords: Winging of scapula, ventral osteochondroma, osteochondroma, scapula, pseudo-winging
Osteochondroma is a common benign bone tumor characterized by a swelling originating from the surface of a bone covered by cartilaginous tissue. Within the scapula, osteochondromas are the most frequently encountered benign bone tumors [1,2,3,4,5,6,7]. Patients with osteochondroma typically present with a single swelling or multiple swellings, which can occur in cases of multiple hereditary exostosis [8]. In cases of solitary scapular lesions, a condition known as snapping scapula syndrome may manifest, characterized by a palpable grinding sensation and audible clicking sound [8]. Snapping scapula syndrome is typically painless but can cause discomfort due to the mechanical effects of a ventral scapular mass impinging on the normally smooth, gliding scapulothoracic joint [8]. In certain instances, patients may present with scapular winging, which can be attributed to a swelling located on the anterior surface of the scapula. In such cases, it is crucial to consider the possibility of an osteochondroma [9]. Winging of the scapula refers to a clinical observation where the medial border of the scapula becomes more prominent than normal [10]. This condition is commonly associated with an injury or dysfunction of the long thoracic nerve, resulting in paralysis of the serratus anterior muscle. However, when scapular winging occurs due to causes other than nerve injury, it is referred to as “pseudo-winging” [10]. The literature has documented multiple causes of pseudo-winging, including shoulder girdle instability, displaced fractures, malunions, and bony tumors [11,12]. Osteochondroma of the scapula is a rare underlying cause of scapular pseudo-winging. In this case report, we present the clinical scenario of a patient with an osteochondroma of the scapula who presented with a swelling over the back.
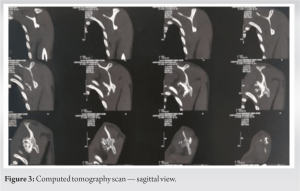
A 21-year-old man reported having a swelling over his left upper back region for the past 10 years, over which period it gradually increased in size. He had no other complaints. On examination, it was found that the overlying integument was normal, bony hard in consistency arising from the medial border of the scapula, non-tender, and approximately 7 × 7 cm in dimension. Moreover, winging of the scapula was observed, which was static as it did not increase with flexion of the arm against resistance. In addition, he had a complete range of motion without neurovascular compromise. Further assessments were conducted using roentgenography, computed tomography scan, and magnetic resonance imaging (Fig. 1, 2, 3, 4), through which two lesions were distinguished; a 70 × 55 mm exophytic tumor arising from the ventral wall of the body of the scapula directed posteromedially, scalloping the adjacent chest wall, and another similar lesion of 30 × 25 mm projecting laterally.


The patient was diagnosed with two ventral osteochondromas located on the body of the left scapula, with one positioned at the posteromedial border and the other proximal to the inferior angle of the scapula. Considering the patient’s cosmetic concerns, a surgical excision was proposed as the treatment approach. The excision procedure was carried out under general anesthesia (Fig. 5).
The surgical technique involved positioning the patient in a prone position. The shoulder was internally rotated to elevate the medial border of the scapula away from the thoracic cage. A parascapular incision was made along the medial and superior border of the scapula. A muscle-splitting approach, involving the trapezius and rhomboid muscles, was employed. No transverse incisions were made in any of the muscles to ensure a quicker post-operative recovery without compromising functional abilities. The osteochondromas were completely excised, and a post-operative X-ray was performed to assess the surgical outcome (Fig. 6). Following the surgery, the patient’s arm was immobilized in an arm pouch splint for a period of 3 weeks to ensure adequate rest. On the day after the surgery, the patient was allowed to engage in pendulum exercises as tolerated. Subsequently, the patient was referred to a rehabilitation program aimed at improving shoulder range of motion. During the course of rehabilitation, it was observed that the functional range of motion of the left shoulder was comparable to that of the unaffected side. The patient reported being free of pain and exhibited no signs of scapular winging. At the 1-year follow-up, the patient remained symptom-free, and there was no evidence of recurrence.
Osteochondroma is a benign tumor characterized by the growth of cartilaginous tissue on the surface of a bone. According to Pongkripetch and Sirikulchayanonta, osteochondromas are the most prevalent type of benign bone tumor, comprising approximately 15% of all bone tumors [13]. In addition, Barbosa et al. reported that osteochondromas account for 45.3% of benign bone tumors [14], and they constitute approximately 3% of tumors in the general population [15]. However, it is worth noting that many cases of osteochondroma are asymptomatic, and affected individuals may not actively seek medical advice. As a result, the true incidence of osteochondromas remains uncertain. Osteochondromas typically occur in the metaphyseal regions of long bones in the lower limb, accounting for approximately 50% of cases. However, they can uncommonly be found in flat bones such as the scapula, representing around 4% of cases [2]. In the scapula, osteochondromas often arise from the anterior part of the bone. As a result, common clinical manifestations on presentation include pain, a grating sensation during movement, and a visible prominence resembling pseudo-winging. It is important to note that in some cases, there may be no palpable lesions or masses, leading to the misinterpretation of these anterior scapular excrescences as scapular winging [16]. In cases of true scapular winging, the swelling or prominence of the scapula increases when the shoulder is flexed against resistance. However, in pseudo-winging, the swelling remains static and does not show an increase with flexion of the arm against resistance. True scapular winging is typically associated with neuromuscular disorders. The most frequent cause of serratus anterior muscle paralysis is nerve injury affecting its innervation [17]. Diagnosis of pseudo-winging due to scapular osteochondroma is often missed [18]. A summary of recent case reports published is presented in Table 1. Pseudo-winging of the scapula is a relatively uncommon diagnosis, as it is rarely encountered in clinical practice. However, clinicians should be aware of the possibility of scapular tumors and tumors in the adjacent thoracic wall, which can lead to pseudo-winging. It is important to consider other differential diagnoses, such as kyphoscoliotic deformity of the upper or mid-thoracic spine, as it can present with a similar clinical picture. Among the various causes of pseudo-winging, osteochondroma located on the anterior surface of the scapula is the most common tumor associated with this condition [24]. Several researchers have reported small case series highlighting the rarity of ventral scapular osteochondromas. For example, Rinaldi reported five cases in 1966 [25], Parsons described three cases, and Fiddian and King reviewed 209 patients with scapular winging, where only one case was attributed to scapular osteochondroma [26,27]. In addition, Scott and Alexander reported a single case of intermittent scapular winging following an initial injury, which was later diagnosed as an osteochondroma [28]. These reports emphasize the importance of maintaining a high index of suspicion and considering further imaging to achieve an early diagnosis in cases of ventral scapular osteochondromas due to their rare presentation. A comprehensive review of the literature on osteochondroma of the scapula indicates that the majority of lesions are typically found along the scapular equator. However, lesions originating from the inferior part of the scapula tend to be larger in size, likely due to the absence of space constraints [29]. Our case aligns with this pattern as the tumors; we observed were also larger in size. It is important to note that the tumor sizes reported in most published studies are generally smaller than what we observed in our case report. In addition, while previous studies often reported solitary lesions, our case involved the presence of two distinct lesions [1,8,29,30,31]. These variations in tumor size and multiplicity highlight the importance of individual patient presentations and the need for comprehensive evaluation in cases of scapular osteochondroma. Surgical resection of scapular osteochondromas can be performed using different techniques, including arthroscopic, mini-open, or open approaches. The patient can be positioned either in the lateral decubitus position or prone position during the surgery. Several excision techniques have been described for scapular lesions. During the resection, it is important to remove the entire lesion, including its stalk if present, to ensure complete excision of the osteochondroma. The choice of surgical technique and approach may depend on the specific characteristics of the lesion and the surgeon’s expertise and preference.
Scapular winging can manifest as either static or dynamic, and the static form can be associated with benign lesions of the scapula. Through thorough investigations, an accurate diagnosis can be achieved. Patients experiencing symptoms that necessitate surgical excision can achieve favorable clinical outcomes with appropriate management.
This case report highlights the importance of considering ventral osteochondromas as a possible cause of scapular pseudo-winging. By raising awareness of this rare condition, clinicians can improve early recognition and appropriate management of patients, potentially leading to better outcomes.
References
- 1.Tittal P, Pawar I, Kapoor SK. Pseudo-winging of scapula due to benign lesions of ventral surface of scapula-two unusual causes. J Clin Orthop Trauma 2015;1:30-5. [Google Scholar | PubMed]
- 2.Calafiore G, Bertone C, Urgelli S, Rivera F, Maniscalco P. Osteochondroma. Report of a case with atypical localization and symptomatology. Acta Biomed Ateneo Parmense 2001;72:91-6. [Google Scholar | PubMed]
- 3.Galate JF, Blue JM, Gaines RW. Osteochondroma of the scapula. Mo Med 1995;92:95-7. [Google Scholar | PubMed]
- 4.Rameez R, Ul-Hassan M, Kotwal HA, Kangoo KA, Nazir A. Painful pseudowinging and snapping of scapula due to subscapular osteochondroma: A case report. J Orthop Case Rep 2016;6:96. [Google Scholar | PubMed]
- 5.Tomo H, Ito Y, Aono M, Takaoka K. Chest wall deformity associated with osteochondroma of the scapula: A case report and review of the literature. J Shoulder Elbow Surg 2005;14:103-6. [Google Scholar | PubMed]
- 6.Sivananda P, Rao BK, Kumar PV, Ram GS. Osteochondroma of the ventral scapula causing scapular static winging and secondary rib erosion. J Clin Diagn Res 2014;8:LD03-5. [Google Scholar | PubMed]
- 7.Bektas YE, Ozmanevra R. An unusual location of osteochondroma: Dorsal scapula. Cureus 2019;11:e64464. [Google Scholar | PubMed]
- 8.Kwon OS, Kelly JI. Delayed presentation of osteochondroma on the ventral surface of the scapula. Int J Shoulder Surg 2012;6:61-3. [Google Scholar | PubMed]
- 9.Aalderink K, Wolf B. Scapular osteochondroma treated with arthroscopic excision using prone positioning. Am J Orthop (Belle Mead NJ) 2010;39:E11-4. [Google Scholar | PubMed]
- 10.Flugstad NA, Sanger JR, Hackbarth DA. Pseudo-winging of the scapula caused by scapular osteochondroma: Review of literature and case report. Hand (NY) 2015;10:353-6. [Google Scholar | PubMed]
- 11.Cooley LH, Torg JS. “Pseudowinging” of the scapula secondary to subscapular osteochondroma. Clin Orthop Rel Res 1982;162:119-24. [Google Scholar | PubMed]
- 12.Martin RM, Fish DE. Scapular winging: Anatomical review, diagnosis, and treatments. Curr Rev Musculoskelet Med 2008;1:1-1. [Google Scholar | PubMed]
- 13.Pongkripetch M, Sirikulchayanonta V. Analysis of bone tumors in Ramathibodi Hospital, Thailand during 1977-1986: Study of 652 cases. J Med Assoc Thai 1989;72:621-8. [Google Scholar | PubMed]
- 14.Barbosa CS, Araujo AB, Miranda D. Incidence of primary benign and malignant neoplasms and bone pseudotumoral lesions. An epidemiologic analysis of 585 cases diagnosed at the Faculdade de Medicina of the Universidade Federal de Minas Gerais. AMB Rev Assoc Med Bras 19911;37:187-92. [Google Scholar | PubMed]
- 15.Fletcher CD, Unni KK, Mertens F, editors: Pathology and Genetics of Tumours of Soft Tissue and Bone. IARC; 2002. Available from: https://publications.iarc.fr/book-and-report-series/who-classification-of-tumours/pathology-and-genetics-of-tumours-o [Google Scholar | PubMed]
- 16.Krieg JC, Buckwalter JA, Peterson KK, El-Khoury GY, Robinson RA. Extensive growth of an osteochondroma in a skeletally mature patient. A case report. J Bone Joint Surg Am 1995;77:269-73. [Google Scholar | PubMed]
- 17.Wiater JM, Flatow EL. Long thoracic nerve injury. Clin Orthop 1999;368:17-27. [Google Scholar | PubMed]
- 18.Pawar E, Modi N, Yadav AK, Mhatre J, Khemkar S, Mishra S. A solitary ventral scapular osteochondroma causing pseudo-winging of scapula: A case report. J Orthop Case Rep 2021;11:82-5. [Google Scholar | PubMed]
- 19.Fageir MM, Edwards MR, Addison AK. The surgical management of osteochondroma on the ventral surface of the scapula. J Pediatr Orthop B 2009;18:304-7. [Google Scholar | PubMed]
- 20.Tungdim PH, Singh II, Mukherjee S, Pertin T. Excision of solitary osteochondroma on the ventral aspect of left scapula presenting as pseudowinging in a 4-year-old boy: A rare case report. J Orthop Case Rep 2017;7:36-40. [Google Scholar | PubMed]
- 21.Chun DI, Cho JH, Choi IH, Yi Y, Kim JY, Kim JH, et al. Osteochondroma of ventral scapula associated with chest pain due to rib cage compression: A case report. Medicine (Baltimore) 2018;97:e0510. [Google Scholar | PubMed]
- 22.Prakash S, Kalra P, Khan Y, Dhal A. Ventral scapular osteochondroma excision through triangle of auscultation: A case series. J Orthop Surgery (Hong Kong) 2020;28:2309499019892848. [Google Scholar | PubMed]
- 23.Barnawal SP, Gandhi BS, Rathod A. Pseudo-winging of scapula due to ventral scapular osteochondroma: A case report and literature review. J Orthop Case Rep 2020;10:69-72. [Google Scholar | PubMed]
- 24.Samilson RL, Morris JM, Thompson RW. Tumors of scapula. J Bone Joint Surg Am 1967;???:2192. [Google Scholar | PubMed]
- 25.Rinaldi E. Acquired winged scapula due to solitary bursal exostosis of the scapula. Arch PuttI Chir Organi Mov 19661;21:127-33. [Google Scholar | PubMed]
- 26.Parsons TA. The snapping scapula and subscapular exostoses. J Bone Joint Surg Br 1973;55:345-9. [Google Scholar | PubMed]
- 27.Fiddian NJ, King RJ. The winged scapula. Clin Orthop Relat Res 1984;185:228-36 [Google Scholar | PubMed]
- 28.Scott DA, Alexander JR. Relapsing and remitting scapular winging in a pediatric patient. Am J Phys Med Rehabil 2010;1:505-8. [Google Scholar | PubMed]
- 29.do Nascimento AT, Claudio GK. Ressalto de escápula. Ressecção artroscópica de osteocondroma subescapular da região superomedial. Relato de caso e revisão da literatura. Rev Bras Ortop 2017;52:220-3. [Google Scholar | PubMed]
- 30.Alatassi R, Koaban S, Almugebel I, Alshehri A. Scapular osteochondroma with winging: A case report. Int J Surg Case Rep 2018;45:138-42. [Google Scholar | PubMed]
- 31.Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report
December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review
August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review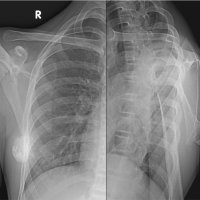 July 10, 2023 Osteochondroma of Dorsal Scapula: A Case Report and Review of Literature
July 10, 2023 Osteochondroma of Dorsal Scapula: A Case Report and Review of Literature