
Kirschner wires and bone allograft can provide rigid fixation constructs to salvage finger motion in pathologic middle phalangeal fracture
Dr. Jeffrey A Marchessault, Department of Orthopaedic Surgery, James H. Quillen College of Medicine, East Tennessee State University, Johnson City, Tennessee. E-mail: jeffrey_marchess@hotmail.com
Introduction: Pathologic phalangeal fracture is a common initial presentation of solitary enchondroma of the finger. Enchondromas of the middle phalanx are most frequently associated with post-operative range of motion deficits. This report describes a case in which the use of Kirschner wires (K-wires) and allograft bone were used to salvage finger motion following surgical fixation of pathologic fracture of a middle phalanx enchondroma with extensor tendon injury.
Case Report: A 37-year-old right hand dominant woman presents with pathologic fracture of the left index finger middle phalanx. The patient elected for surgical intervention to stabilize fracture and enable early motion at the proximal interphalangeal joint (PIP). Surgical fixation involved tumor curettage, fracture stabilization and length preservation with longitudinal K-wires, allograft bone with hardening properties to fill the bony defect, and dorsal K-wires for securing the extensor tendon. At follow-up 11 months postoperatively, the allograft had almost completely resolved, and the patient had regained PIP flexion of 90° and full extension.
Conclusion: Pathologic fracture of middle phalanx enchondroma is prone to complication by extensor tendon injury and associated post-operative loss of motion. Bone grafting and Kirschner wire fixation allowed for early mobilization of finger motion and thus may be a useful technique for use in treatment of other pathologic fractures.
Keywords: Enchondroma, pathologic fracture, Boutonnière deformity.
Enchondromas are the most common primary bone tumor of the hand [1]. These lesions are slow growing, benign tumors of hyaline cartilage derived from abnormal intramedullary cartilaginous cell proliferation. It is estimated that one-third of all enchondromas occur in the hand, most frequently affecting the proximal phalanges, followed by the middle phalanges, metacarpals, and distal phalanges [2]. Because there are no definitive clinical symptoms of hand enchondromas, pathologic fracture is a common initial presentation. To ensure appropriate diagnosis, it is recommended that all tumors should be evaluated with radiographs and ultrasound imaging to locate and characterize the tumor [3]. While most patients who undergo surgical intervention for hand enchondroma recover adequate function and range of motion postoperatively, it is suggested that patients presenting with pathologic fracture are at increased risk for range of motion deficits, specifically those with lesions of the middle phalanx [4].
There are numerous approaches to surgical fixation of hand enchondroma with pathologic fracture. Here, we discuss the case of a 37-year-old woman with pathologic fracture of a middle phalanx enchondroma with extensor tendon injury who achieved full range of motion following surgical fixation with Kirschner wires (K-wires) and bone allograft.
A 37-year-old right hand dominant woman inadvertently bumped her left index finger while reaching for her money at an automated teller machine. Radiographs (Fig. 1a and b) revealed a comminuted intra-articular middle phalanx fracture. Surgery was offered to stabilize the fracture and allow early range of motion of the proximal interphalangeal joint (PIP).
A dorsal skin incision was curved around the PIP extensor creases to reduce scar contracture. The intralesional curettage was sent for pathology, which confirmed enchondroma. The remaining shell of cortical bone was stabilized with longitudinal K-wires to preserve length. Allograft bone with hardening properties (Montage allograft, Abyrx, Stamford, Connecticut), was used to fill the defect. Dorsal K-wires were used to secure the proximal fragment with the central slip attachment (Fig. 2a and b).
Post-operative hand therapy was started within the 1st week of therapy to allow protected active range of motion of the PIP joint. A dorsal blocking forearm-based orthosis was fabricated to protect the pins in the post-operative period. The patient’s finger pins were removed 6 weeks after surgery. At 11 months after surgery, the allograft had almost completely resolved (Fig. 3a and b) and the patient had regained PIP flexion of 90° and full extension (Fig. 4a and b).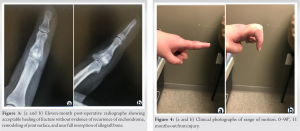
It is estimated that 90% of primary hand tumors are enchondromas [2]. While enchondromas are typically painless and slow growing in nature, they may progress with eventual destruction of the phalanges, hence the frequency of pathologic fracture.
There is no standard approach to timing or technique for surgical fixation of finger enchondroma. General aims of surgical intervention for fixation of middle phalangeal fracture include gentle dissection to minimize tissue disruption, preservation of vascular supply to promote union, minimizing tendon manipulation to decrease adhesion formation, careful repair of the periosteum to protect gliding surfaces, and repair of extensor tendon mechanism to ensure adequate regain of function [5]. A review of enchondroma fixation identified several broad management categories, including curettage alone, curettage followed by augmentation with cancellous autograft, curettage followed by augmentation with bioactive and osteoconductive materials other than autograft, and curettage followed by augmentation with bone cements [6]. This review reported low rates of complication for all categories and concluded that simple curettage was a simple and effective management technique for treating most hand enchondromas. It is important to note that in this review, enchondromas presenting with pathologic fractures were treated with a two-stage management approach in which the fracture was allowed to heal prior to curettage. This two-stage approach has traditionally been the mainstay of treatment with the idea that allowing time for fracture union would enable future application of simple curettage without the need for internal fixation [7]. However, a more recent study by Zhou et al. compared early versus delayed surgical intervention in hand enchondromas [8]. Their results indicate that patients with pathologic fracture treated with early, one-stage management had no difference in outcome to patients without pathologic fracture, and they achieved significantly faster return to activity than those treated by delayed surgery [8]. This is logical, as delayed intervention results in increased length of immobilization that prolongs time to functional recovery. Similar results are demonstrated by Sassoon et al [9]. This data suggests that early intervention for pathologic fractures is recommended as evidenced by no difference in surgical outcome compared to the non-fracture group and overall faster return to activity compared to the delayed intervention group evidenced in both studies [8,9]. A common thread among existing literature is a focus on complications from an oncological standpoint (i.e., tumor recurrence, progression to malignancy) as opposed to functional complications, specifically regarding recovery of finger motion. This is likely due in part to the gravity of potential oncological complications; however, it is important to consider functional recovery postoperatively as motion deficits can significantly impact a patient’s quality of life. A recent study looking to characterize the effects of patient and tumor characteristics on post-operative motion recovery in hand enchondroma found that pre-operative pathologic fracture lends greater risk of post-operative extension deficit compared to those without, specifically in those with middle phalangeal involvement [4]. Range of motion deficits observed with middle phalangeal injury were most often those of extensor lag, which authors proposed to be related to extensor mechanism adhesions and involvement of the central slip or triangular ligament [4]. Deficit of the central slip action and subsequent volar subluxation of the lateral bands may induce a Boutonnière deformity in the weeks following initial trauma [10]. Boutonnière deformity is characterized by flexed posture of the PIP with hyperextension of the distal interphalangeal joint due to volar migration of the lateral bands. Decreased thickness of the extensor tendon in the distal segment contributes to the difficulty of surgical repair and can lead to significant deficits in range of motion after tendon repair. Thus, pathologic fracture of the middle phalanx with extensor tendon injury as exhibited by our patient poses a challenging surgical endeavor to achieve adequate curettage, extensor tendon repair, and fracture union in a manner which also allows for recovery of finger motion. Ultimately, there is no standard surgical approach for the management of finger enchondroma. While it is suggested that finger enchondromas presenting with pathologic fracture may be best approached with early as opposed to delayed intervention, there are no other accepted guidelines to direct preservation of finger motion in pathologic fracture. Furthermore, middle phalangeal involvement presents a unique challenge with respect to potential extensor mechanism impairment. Therefore, K-wires and allograft bone that provide structural support are a viable option for consideration to salvage finger motion in treatment of pathologic fracture.
While complications are generally uncommon in curettage of finger enchondroma, presentation with pathologic fracture warrants additional consideration as to appropriate surgical approach. Pathologic fracture of the middle phalanx is privy to complication by extensor tendon injury and associated loss of motion. Early intervention with bone allograft and K-wire fixation enabled restoration of finger motion in this patient and thus may be a useful technique for use in treatment of other pathologic fractures of finger enchondromas.
Fractures of the middle phalanx are susceptible to complication by extensor tendon injury and associated loss of finger motion. This presentation is increasingly complicated in the case of pathologic fracture. As return to function is a chief goal for most patients, this case demonstrates that early surgical intervention with K-wires and bone allograft can provide rigid fixation constructs to salvage finger motion when treating pathologic fracture of finger enchondroma.
References
- 1.Lubahn JD, Bachoura A. Enchondroma of the hand: Evaluation and management. J Am Acad Orthop Surg 2016;24:625-33. [Google Scholar | PubMed]
- 2.Yue KL, Lans J, Castelein RM, Suster DI, Nielsen GP, Chen NC, et al. Benign hand tumors (Part I): Cartilaginous and bone tumors. Hand (NY) 2022;17:346-53. [Google Scholar | PubMed]
- 3.Lazerges C, Degeorge B, Coulet B, Chammas M. Diagnosis and treatment of hand tumors. Orthop Traumatol Surg Res 2022;108(1S):103153. [Google Scholar | PubMed]
- 4.Wessel LE, Christ AB, Athanasian EA. Impact of patient and tumor characteristics on range of motion and recurrence following treatment of enchondromas of the hand. J Hand Surg Am 2023;48:512.e1-7. [Google Scholar | PubMed]
- 5.Carpenter S, Rohde RS. Treatment of phalangeal fractures. Hand Clin 2013;29:519-34. [Google Scholar | PubMed]
- 6.Bachoura A, Rice IS, Lubahn AR, Lubahn JD. The surgical management of hand enchondroma without postcurettage void augmentation: Authors’ experience and a systematic review. Hand (N Y) 2015;10:461-71. [Google Scholar | PubMed]
- 7.Pianta TJ, Baldwin PS, Obopilwe E, Mazzocca AD, Rodner CM, Silverstein EA. A biomechanical analysis of treatment options for enchondromas of the hand. Hand (N Y) 2013;8:86-91. [Google Scholar | PubMed]
- 8.Zhou X, Zhao B, Keshav P, Chen X, Gao W, Yan H. The management and surgical intervention timing of enchondromas: A 10-year experience. Medicine (Baltimore) 2017;96:e6678. [Google Scholar | PubMed]
- 9.Sassoon AA, Fitz-Gibbon PD, Harmsen WS, Moran SL. Enchondromas of the hand: factors affecting recurrence, healing, motion, and malignant transformation. J Hand Surg Am 2012;37:1229-34. [Google Scholar | PubMed]
- 10.Colzani G, Tos P, Battiston B, Merolla G, Porcellini G, Artiaco S. Traumatic extensor tendon injuries to the hand: Clinical anatomy, biomechanics, and surgical procedure review. J Hand Microsurg 2016;8:2-12. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Enchondroma of Hands: A Surgical Dilemma and Our Experience
November 1, 2025 Enchondroma of Hands: A Surgical Dilemma and Our Experience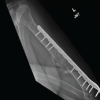 October 1, 2025 Use of the IlluminOss Implant for Treating a Pathologic Humeral Fracture in a Patient with Renal Cell Carcinoma Metastasis: A Case Report
October 1, 2025 Use of the IlluminOss Implant for Treating a Pathologic Humeral Fracture in a Patient with Renal Cell Carcinoma Metastasis: A Case Report July 1, 2025 Twenty-Four-Year Follow-up of Successful Total Hip Arthroplasty for Recurrent Proximal Femoral Aneurysmal Bone Cyst with a Pathologic Fracture Following Extended Curettage and Bone Grafting: A Case Report
July 1, 2025 Twenty-Four-Year Follow-up of Successful Total Hip Arthroplasty for Recurrent Proximal Femoral Aneurysmal Bone Cyst with a Pathologic Fracture Following Extended Curettage and Bone Grafting: A Case Report May 1, 2025 Case of Enchondroma of Left 4th Metacarpal of Hand Treated with Excision and Bone Grafting with Left 2nd Metatarsal of Foot: A Rare Case Report
May 1, 2025 Case of Enchondroma of Left 4th Metacarpal of Hand Treated with Excision and Bone Grafting with Left 2nd Metatarsal of Foot: A Rare Case Report