
Idiopathic or primary congenital pseudoarthrosis can involve the femur as well as other long bones. It may or may not be associated with hip dysplasia. Idiopathic or primary congenital pseudoarthrosis of the femur can be managed adequately with a masquelet procedure.
Dr. Aakarsh Aggarwal, Department of Orthopaedics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India. E-mail: aakarshaggarwal1@gmail.com
Abstract
Introduction: Congenital pseudoarthrosis is a rare disorder, and mostly occurs in the radius, ulna, tibia, and fibula, but is not reported in the femur. Congenital cases that were reported in the literature, most were associated with neurofibromatosis, cleidocranial dysostosis, congenital constriction band syndrome and fibrous dysplasia, and the acquired cases followed fractures of bones or tuberculosis. Since the life span of the patient is affected rarely, clinical examination of these patients and serial radiographs can give us plenty of information about the limb abnormality, its clinical course, and the nature of the underlying disturbance of growth.
Case Report: A 3-year-old female child presents to the outpatient department of a tertiary care hospital with complaints of pain, swelling, and deformity thigh region right side for 5 months. On examination, swelling was present (2 × 2 cm) at the junction of the mid and distal thigh, smooth surface, ill-defined edges, soft and non-tender. There was abnormal mobility which was noted at the right thigh at the junction of the middle and distal 1/3 right femur. Magnetic resonance imaging reported circumferential periosteal reaction with cortical surface irregularity of the right femoral shaft was also noted. The findings were reported to be concerning for chronic osteomyelitis with non-united fracture and cortical resorption/chronic bone loss. Histopathological sections showed multiple bits of viable bony trabeculae with surrounding fibrocollagenous tissue displaying significant proliferation of fibroblasts, slit-like blood vessels, arterioles and moderate mixed inflammatory infiltrate of plasma cells, few neutrophils, lymphocytes, histiocytes and few multinucleated histiocytes. She was managed with resection of pseudoarthrosis and masquelet procedure stage 1 and later masquelet stage 2 (cement spacer removal and ipsilateral ileac crest bone grafting with fixation with 7-hole distal fibular anatomical plate and bone graft substitute placement [ChronOs]).
Conclusion: Idiopathic or primary congenital pseudoarthrosis can involve the femur as well as other long bones. It may or may not be associated with hip dysplasia and the outcome may not be as bad as previously reported in the pseudoarthrosis of other long bones.
Keywords: Congenital pseudoarthrosis femur, masquelet procedure, congenital disorder, pseudoarthrosis.
Different types of congenital defects of the femur are reported in literature ranging from simple hypoplasia of the bone to complete absence. It includes congenital coxa vara, femoral hypoplasia with coxa vara, hypoplasia of the lower femoral epiphysis, and pseudoarthrosis of the femur [1]. Congenital pseudoarthrosis is a rare disorder, and mostly occurs in the radius, ulna, tibia, and fibula, but is not commonly reported in the femur. Congenital cases which were reported in the literature, most were associated with neurofibromatosis, cleidocranial dysostosis [2], congenital constriction band syndrome [3], and fibrous dysplasia and the acquired cases followed fractures of bones [4] or tuberculosis [5]. Primary congenital pseudoarthrosis is reported in literature uncommonly and vaguely and this condition has poor outcomes even after surgical intervention [6]. Although other skeletal defects may be commonly seen in these patients, the major congenital abnormalities affecting the nervous system, thorax, or abdomen are uncommon. Thus life span of the patient is affected rarely, and detailed autopsy or histopathological examination is not done commonly. Therefore, clinical examination of these patients and serial radiographs can give us plenty of information about the limb abnormality, its clinical course, and the nature of the underlying disturbance of growth [1]. Here, we report a case of congenital pseudoarthrosis of the femur, which was managed with resection of pseudoarthrosis and masquelet procedure stage 1 and later masquelet stage 2 (cement spacer removal and ipsilateral ileac crest bone grafting with fixation with 7-hole distal fibular anatomical plate and bone graft substitute placement [ChronOs]) [7-10].
A 3-year-old female child presents to the outpatient department of a tertiary care hospital with complaints of pain, swelling, and deformity of the thigh region on the right side for 5 months. Pain increased on passive range of motion and weight bearing. There was a past history of slab application done for 3 months at a private hospital. No history of significant trauma was reported. No other past illness or any medications were taken. Detailed interviews of parents have revealed no evidence of familial disorder, and other congenital disorders within the immediate family. The antenatal, peri and post-natal history has failed to indicate any significant abnormality or infection. The patient had a normal birth history with normal vaginal delivery at full term and cried at birth. No ICU admission/jaundice/seizure was reported. She had no signs of neurocutaneous diseases or any anomalies. The skeletal survey of the patient was normal. Five months back parents noted sudden onset swelling over the right thigh region and took her to a nearby private hospital. The patient was admitted for 25 days and treated conservatively with a crepe bandage and traction with 1 kg during the hospital stay thereafter the child complained of minimal pain and no swelling and the patient was discharged. After 2 months, parents again noticed the appearance of swelling over the same thigh region and the child was treated with an above-knee slab for the next 3 months. With no relief and increasing swelling child was referred to the higher tertiary care center. On examination, during the inspection, there was swelling and deformity of the right thigh with no scar mark, dilated vein, or any discoloration. On palpation, there was no tenderness or rise of temperature noted. The swelling was 2 × 2 cm at the junction of the mid and distal thigh, smooth surface, ill-defined edges, soft- and non-tender. There was abnormal mobility which was noted at the right thigh at the junction of the middle and distal 1/3 right femur. Hip, knee, ankle, and toe range of movements were full. Dorsalis pedis and posterior tibial artery pulsation were intact. The tone of the limb was normal. Sensation was intact, motor power was 5/5, and reflexes were intact (Fig. 1).

Abdominal ultrasound and computed tomography scan of the brain were normal. Hematological indices, liver function tests, and renal function tests were normal. Chromosomal study was also normal in this patient. Radiographic images of the affected thigh showed bone loss of the shaft femur at the junction of the middle and distal third with tapering of both proximal and distal segments (Fig. 2).

Magnetic resonance imaging was done and reported a chronic non-united fracture with bone loss and angulation deformity at the lower right femoral shaft. Abnormal T2W bright granulation tissue/chronic infective phlegmon at the site of bone defect with STIR hyperintense and TIW hypointense marrow edema of the femoral shaft and the lower femoral metaphysis seen. Circumferential periosteal reaction with cortical surface irregularity of the right femoral shaft was also noted. Reticulated non-focal sheetlike edema signals in the (atrophic) deep anterior compartment lower thigh muscle were seen. They reported the findings are concerning for chronic osteomyelitis with non-united fracture and cortical resorption/chronic bone loss. Medial and lateral femoral condyles were normal. The lower femoral growth plate was intact. The evaluation of the right knee joint and right hip joints was normal with no articular involvement.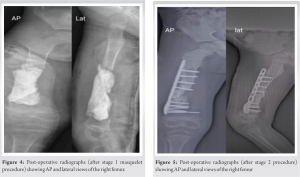
Before the surgical intervention, it was noted that she had an antalgic gait with a short limb component and a limb length discrepancy of 3 cm. The patient underwent the resection of pseudoarthrosis with bone cement application stage 1 masquelet procedure in November 2023 (Fig. 3). The second surgery was done in December 2023 where stage 2 masquelet procedure (cement spacer removal and ipsilateral ileac crest bone grafting with fixation with 7-hole distal fibular anatomical plate and bone graft substitute placement [ChronOs]) was done [7-10] (Fig. 4-7). Intraoperatively, a biopsy sample was collected. Histopathological sections showed multiple bits of viable bony trabeculae with surrounding fibro-collagenous tissue displaying significant proliferation of fibroblasts, slit-like blood vessels, arterioles, and moderate mixed inflammatory infiltrate of plasma cells, few neutrophils, lymphocytes, histiocytes, and few multinucleated histiocytes. An occasional aggregate of neutrophils bordered by multinucleated histiocytes and giant cells was seen. The bony trabeculae also showed intertrabecular cellular bone marrow with an occasional reactive lymphoid follicle, lymphoid aggregates, and increased eosinophils. Focal reactive bone formation was seen. Focal synovial lining epithelium with palisaded synoviocytes was noted within the tissue. No fungal profile or well-formed epithelioid cell granuloma was noted. No definite evidence of neoplastic pathology in the sections examined (Fig. 8).
Intraoperative samples were taken and sent for Grams stain, culture sensitivity, and KOH mounts which showed no growth.
True congenital pseudoarthrosis is a rare disorder, although the term has been loosely used by authors in previous reports. Some of those cases followed pathological fractures secondary to fibrous dysplasia or neurofibromatosis [6]. In neurofibromatosis, there is a skeletal involvement with a predilection for the tibia, but less commonly for the radius and the ulna and rarely for the femur. In our patient, the diagnosis was made late after 3 years of age, until the child began to walk, the possible reason may be the slight inequality of leg length. The abnormality is confined to the skeleton. No evidence of muscular or nervous abnormality was seen in this patient, although muscle attachments may be bizarre in the presence of gross skeletal defects. The pseudoarthrosis in our case appears to be primary and not secondary to local pathology, as post-surgery follow-up did not reveal non-union or recurrence. Since the pseudoarthrosis in this case was situated in the junction of the middle and distal third of the shaft of the femur bone, the case does not fall in any of the four groups of Aitken’s classification for proximal focal femoral deficiency, hence, it is a case of pseudoarthrosis of the femur. The extent of the limb length inequality is the sole cause of disability in these patients. The externally rotated position of the limb does not give rise to any functional disability. In the individual child, the outlook depends primarily upon the extent of the femoral defect. By relating the length of the two femora the shortening of the limb may be predicted with fair accuracy at any age. To the best of our knowledge, congenital pseudoarthrosis of the femur is described in very few cases in the literature and even if they are described, most were associated with neurofibromatosis, cleidocranial dysostosis [2], congenital constriction band syndrome [3], and fibrous dysplasia and the acquired cases followed fractures of bones [4], or tuberculosis [5]. Following the spontaneous healing of the pseudoarthrosis, surgical intervention using Masquelet’s induced membrane technique straightened the femoral shaft and lengthened the femur. Since very few studies are done on these types of patients and very little available literature, it is difficult to predict the course of this disorder and to draw specific guidelines for its management and more such studies are required in future.
Idiopathic or primary congenital pseudoarthrosis can involve the femur as well as other long bones. It may or may not be associated with hip dysplasia and the outcome may not be as bad as previously reported in the pseudoarthrosis of other long bones. Masquelet procedure can be used to treat idiopathic or primary congenital pseudoarthrosis of the femur.
Idiopathic or primary congenital pseudoarthrosis can involve the femur as well as other long bones such as radius, ulna, tibia, and fibula. The masquelet’s induced membrane technique is capable of managing idiopathic or primary congenital pseudoarthrosis of the femur with decent outcomes.
References
- 1.Ring PA. Congenital abnormalities of the femur. Arch Dis Child 1961;36:410-7. [Google Scholar | PubMed]
- 2.Lemperg R. Kleidokranial dysostos med pseudarthrosis femoris congenita [Cleidocranial dysostosis with congenital pseudarthrosis of the femur]. Nord Med 1963;70:986-7. [Google Scholar | PubMed]
- 3.Naik P, Patel P, Shah N, Suthar R. Congenital pseudarthrosis of femur and sciatic nerve palsy with congenital constriction band syndrome: Report of the first case in literature. Indian J Orthop 2021;55:1050-5. [Google Scholar | PubMed]
- 4.Song HR, Cho SH, Koo KH, Jeong ST. Spontaneous healing of an atrophic pseudoarthrosis during femoral lengthening. A case report with six-year follow-up. Int Orthop 1999;23:126-7. [Google Scholar | PubMed]
- 5.Ranjan R, Kumar R, Jeyaraman M, Jeyaraman N, Yadav S. Pseudoarthrosis of the femur secondary to tuberculosis: A rare and first report. Cureus 2023;15:e50841. [Google Scholar | PubMed]
- 6.Al-Hathal MM, Al-Tawil KI, Ghaffar TA, Almohrij S, Ahmed GS, Al Summan AA. Primary congenital pseudoarthrosis of the femur. Ann Saudi Med 2000;20:291-3. [Google Scholar | PubMed]
- 7.Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am 2010;41:27-37. [Google Scholar | PubMed]
- 8.Masquelet A, Kanakaris NK, Obert L, Stafford P, Giannoudis PV. Bone repair using the masquelet technique. J Bone Joint Surg Am 2019;101:1024-36. [Google Scholar | PubMed]
- 9.Masquelet AC, Fitoussi F, Begue T, Muller GP. Reconstruction des os longs par membrane induite et autogreffe spongieuse [Reconstruction of the long bones by the induced membrane and spongy autograft]. Ann Chir Plast Esthet 2000;45:346-53. [Google Scholar | PubMed]
- 10.Gouron R. Surgical technique and indications of the induced membrane procedure in children. Orthop Traumatol Surg Res 2016;102 1 Suppl:S133-9. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report
January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report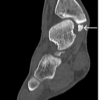 April 1, 2026 Symptomatic Accessory Ossicle Near the Medial Malleolus Simulating Fracture Non-union: A Case Report and Literature Review
April 1, 2026 Symptomatic Accessory Ossicle Near the Medial Malleolus Simulating Fracture Non-union: A Case Report and Literature Review December 1, 2025 Delayed Sacral Insufficiency Fracture Following Oncologic Resection of a Chondrosarcoma: Emphasizing the Role of Biomechanical Risk Assessment
December 1, 2025 Delayed Sacral Insufficiency Fracture Following Oncologic Resection of a Chondrosarcoma: Emphasizing the Role of Biomechanical Risk Assessment October 1, 2025 Pediatric Patient with Septic Arthritis and Necrotising Fascitis: A Case Report
October 1, 2025 Pediatric Patient with Septic Arthritis and Necrotising Fascitis: A Case Report