
Despite the fact that simultaneous bilateral ankle fractures are uncommon, they significantly affect a patient’s quality of life and necessitate effective rehabilitation.
Dr. Thabo Leonard Muhango, Orthopaedic Surgery Registrar, Chris Hani Baragwanath Academic Hospital, Department of Orthopaedic, University of the Witwatersrand, Johannesburg, South Africa. E-mail: thaboleonardmuhango@gmail.com
Introduction: Bilateral simultaneous rotational ankle fractures are an unusual phenomenon that remains unreported in the English literature, and to our knowledge, about 10 cases have been reported. The aim of the study was to evaluate and report clinical outcomes of bilateral simultaneous ankle fractures in our institution.
Case Report We conducted a review of our 2-year experience with patients who had simultaneous bilateral fractures of the ankles and were treated at our institution. The included patients underwent surgical treatment using open reduction and internal fixation. Patients’ functional outcomes were assessed using patient-reported outcome measures (PROMs), namely the Short Form-36 questionnaire and the Olerud and Molander Ankle Outcome Score (OMAS).
Results: Two cases (four ankles) of simultaneous bilateral rotational ankle fractures were identified in our institution’s records. Both cases involved a pedestrian motor vehicle accident. They were both female and had an average age of 22.5 years. Due to an open injury, one ankle underwent a staging procedure, and the other three underwent open reduction and internal fixation with excellent clinical outcomes. Functional outcomes were measured with PROMs.
Conclusion: Simultaneous bilateral ankle fractures, while uncommon, can have a substantial impact on an individual’s mobility and health-related quality of life. Early surgical intervention and effective rehabilitation enhance functional results in this devastating journey.
Keywords: Simultaneous bilateral ankle fractures, bimalleolar fracture, open fracture, rotational ankle injuries.
Ankle fractures remain prevalent, accounting for approximately 14% of all fractures that necessitate inpatient treatment [1]. In the lower limbs, ankle fractures are common, accounting for 3.9–10.2% of fractures in adults [2]. Simultaneous bilateral ankle fractures are uncommon in the English literature, and Alrashedan et al. reported a case series and literature analysis that included 10 cases over 10 years, averaging around one case per year [3]. Various communication classification methods have been developed to categorize ankle fractures based on morphological classification, classification based on distal fibula fracture, and classification based on the foot position and the direction of force during the injury [4,5]. To diagnose simultaneous bilateral ankle fractures, a comprehensive evaluation is necessary, including a thorough history, a complete physical examination, and the use of imaging techniques such as plain radiography, and computed tomography scans for more complex fractures [3,5,6]. An approach to ankle fracture treatment depends on various factors, including patient factors, fracture factors, and surgeon factors, to decide between conservative or surgical treatment. The goal is to achieve anatomical reduction and immediate stability. Non-operative treatment consists of the reduction and immobilization of the ankle joint. The surgical approach includes debridement, external fixation, or open reduction with internal fixation, depending on the aforementioned factors [1,4,5]. Previous studies have reported good to excellent outcomes (52–87%) on ankle fractures. Other studies, however, reported few full recoveries in most patients, affecting psychological status, difficulties with sports activities, and gait impairment [7,8]. In this study, we present our experience with cases who sustained simultaneous bilateral fractures of ankles and report on their functional outcomes following surgical intervention.
We conducted a review of patients diagnosed with bilateral simultaneous ankle fractures that were treated between the period March 2022 and March 2024 at our academic hospital in Johannesburg, South Africa. Ethics approval was obtained from our institution: M240668. Three cases were identified and recalled for participation in the study. This study included two cases (four ankles) and excluded one due to a lack of patient consent. Patients’ functional outcomes were assessed using patient-reported outcome measures, namely the Short Form-36 questionnaire and the OMAS (Olerud and Molander Ankle Outcome Score). The medical outcomes Short-Form Health Survey SF-36 (the RAND 36-item) instrument is a patient-reported questionnaire used to measure health-related quality of life (HRQoL). The score in each domain ranges from 0 to 100, with a higher score representing the excellent HRQoL status. We used the RAND 36-Item Health Survey 1.0 questionnaire [9]. The Olerud Molander Ankle Score (OMAS) is a patient-reported outcome measure for evaluating symptoms after ankle injuries. The OMAS ranges from 0 to 100. A higher score indicates a better functional outcome [10].
Case #1
A 17-year-old African female presented to our trauma emergency department following a pedestrian-vehicle accident with bilateral ankle injuries. She was brought in by a paramedic team with painful ankles and feet, and unable to walk. The patient was otherwise well with no significant past surgical or medical history. The patient was seen and cleared of other life-threatening conditions by the trauma and orthopedic team on a call using Advanced Trauma Life Support (ATLS) principles. The patient was clinically stable with isolated injuries to both ankles. On the left ankle, it was a closed injury, and the patient was neurovascular intact. On the right ankle, there was a laceration on the medial aspect of the ankle, just superior to the medial malleolus, measuring approximately 6 cm × 2 cm (Fig. 1), and the neurovascular status was intact. The ankles were mildly swollen, with tenderness on both the lateral and medial malleoli. She was unable to weight-bear due to significant pain.

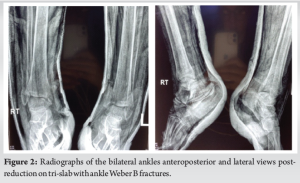
Plain radiographs were done and showed that the patient sustained asymmetrical bimalleolar fractures. On the left, a closed Denis Weber B ankle fracture and Lauge Hansen supination adduction type. On the right, an open Gustilo-Anderson 2, Denis Weber B ankle fracture, and Lauge Hansen supination external rotation type. In the emergency department, the open ankle fracture was irrigated with normal saline, and dressed with wet gauze. Both ankles were reduced under sedation and placed on tri-slabs, and control plain radiographs post-reduction were done (Fig. 2). Stat doses of augmentin 1.2 g intravenous injection and tetanus toxoid 40 IU (0.5 ml) intramuscular and morphine 10 mg were given.
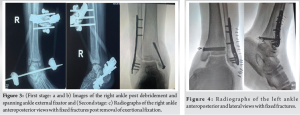
The patient was booked urgently for debridement and external fixation of the open fracture and open reduction and internal fixation of the closed fracture with plate and screws. These procedures were done in the same setting approximately 36 h post the injury. A thorough debridement was performed, and a cross-ankle external fixator was applied for the right ankle utilizing an Ortho-XACT trauma frame (Fig. 3a and b). On the left, a plate and screws were used for fixation of the lateral malleolus, and two cannulated screws were used for fixation of the medial malleolus (Fig. 4). A second stage was performed on the right ankle. The external fixator was converted to a definitive open reduction and internal fixation using a plate and screws approximately 2 weeks (16 days) later (Fig. 3c).
Post open reduction and internal fixation of both ankles, a similar approach was applied. The patient’s surgical wounds were reviewed in our orthopedic specialized outpatient department for at least 2 weeks. Sutures were removed, wounds were dressed with a dry dressing, and both ankles were placed on a below-knee circular plaster of Paris (POP) cast for 4 weeks, during which period the patient remained non-weight-bearing. At 6 weeks, the POP was removed, and the patient was allowed to weight-bear as tolerated and commenced a range of motion exercises with the physiotherapist.
Case #2
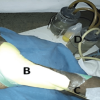
A 28-year-old African female was referred from a local clinic to our trauma emergency department following a pedestrian-vehicle accident with bilateral ankle injuries. The patient was not known to have comorbidities, nor did she have any significant past medical or surgical history. The patient was seen and cleared of other life-threatening injuries by the trauma and orthopedic team on a call using ATLS principles. The patient was hemodynamically stable with normal cardiopulmonary, abdominal, and central nervous system examinations. On focussed musculoskeletal examination, the patient was unable to weight-bear and had bilateral ankle injuries. On inspection of the left ankle, there was a varus deformity noted with associated swelling and a superficial 2 cm × 2 m abrasion over the lateral malleolus. On palpation, there was tenderness over both malleoli, neurovascularly intact, soft compartments, and pain on passive movement. Active movement was limited due to pain (Fig. 5). On inspection of the right ankle, there was mild swelling noted. On palpation, there was tenderness over the medial malleolus, neurovascularly intact, soft compartments, and pain on passive movement. Active movement was limited due to pain (Fig. 5).

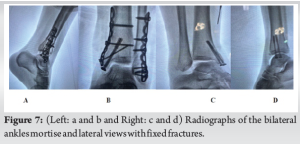
Plain radiographs were done and showed that the patient had sustained asymmetrical ankle fractures. On the left, a closed Weber B2 fracture-dislocation, Lauge Hansen Classification supination external rotation. On the right, a closed Herscovici type D isolated medial malleolus fracture (Fig. 6). In the emergency department, the abrasion on the left ankle was washed with normal saline and dressed. Both ankles were reduced under monitored procedural sedation and placed in plaster of Paris tri-slabs. Post-reduction plain radiographs (Fig. 6) were done and the patient was admitted for analgesia, limb elevation, pre-operative workup, and definitive management. After the settling of soft tissues and consent was completed, the patient was booked for bilateral open reduction and internal fixation with a plate and cannulated screws on the left and cannulated screws on the right (Fig. 7). The procedures were done in the same sitting 6 days after admission without complication. The patient was subsequently discharged 2 days later.
Postoperatively, the patient was seen and reviewed in our orthopedic specialized outpatient department in 2 weeks. Sutures were removed, wounds were dressed with a dry dressing, and both ankles were placed on below circular plaster of Paris (POP) cast for 4 weeks in which period the patient remained non-weight-bearing. At 6 weeks, the POP was removed, and the patient was allowed to weight-bear as tolerated and commenced a range of motion exercises with the physiotherapist.
Patient outcomes
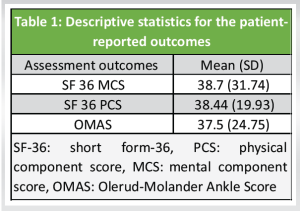
The overall mean follow-up for the two patients included in this study was 5.5 months. Post-operative questionnaires were completed by the two patients (Table 1). The SF-36 revealed a mean physical component summary (PCS) of 38.44 compared to the mental component summary (MCS) mean of 38.7. The Olerud–Molander Ankle Score revealed a mean of 37.5.
A unilateral ankle fracture is one of the most common orthopedic injuries, with an incidence that keeps changing annually [11,12]. Most ankle fractures are malleolar in nature, with approximately 70% involving an isolated malleolus. Open fractures are rare, comprising just 2% of all ankle fractures [11,12]. Bilateral simultaneous ankle fractures are uncommon injuries that could result from high traumatic injuries, most commonly in male patients with a mean age of 30.4 (age range: 13–72) [3]. In this study, all of our cases were female. Both of our cases in this study resulted from high-energy injuries sustained in a passenger vehicle accident, which were associated with bilateral simultaneous rotational injuries. This is uncommon, especially since the energy received resulted in symmetrical rotational injuries rather than axial-type ankle fractures [3]. The clinical appearance of ankle fractures necessitates immediate reduction and immobilization. If plain radiographs would result in an unacceptable delay, they should not be conducted before reduction [1]. Patients who are medically fit to tolerate anesthesia receive surgical treatment for displaced and unstable ankle fractures. These fractures are associated with syndesmotic disruption, displaced fractures, unstable bi-malleolar fractures, unstable tri-malleolar fractures, joint incongruity, or talar subluxation, and open ankle fractures [1,5,6]. Both of our cases underwent surgical management. The indications for surgery in these ankle fractures were open fracture, instability, and displacement. The single open ankle fracture had a staged procedure. There is currently no consensus on whether it is better to mobilize or use a cast to treat ankle fractures post-surgery. Studies have demonstrated that determining the comparative benefits or drawbacks of early mobility versus cast immobilization is challenging [13]. Early mobilization after surgery should be customized to the individual requirements of the patient to optimize healing and enable a return to work. It could also be a safer and more effective course of treatment [13]. In this study, the post-operative care regimen for bilateral simultaneous ankle fractures involved immobilization in a below-knee plaster cast without weight-bearing for a period of 6 weeks. Bilateral simultaneous ankle fractures may also have a significant health-related quality-of-life impact. McKeown et al. conducted a study that evaluated the experiences of 10 unilateral ankle fracture patients through interviews about 4 months post-injury. Their study demonstrated the comprehensive impact of a fractured ankle on an individual’s overall well-being, encompassing aspects such as sleep quality, independence, social interactions, and mental well-being [14]. Ponzer et al. conducted a study comparing the SF-36 with the OMAS and found a significant correlation between these distinct scores as regards of patient function [15]. The most significant enhancement of the Patient-Reported Outcome Measures (PROMs) usually occurs within an interval that ranges from 4 to 10 months following the unilateral ankle surgical procedure [16]. In a larger cohort study, it will be necessary to explore the relationship between PROMs improvement and the duration of follow-up in cases of bilateral simultaneous ankle fractures. In this study, health-related quality of life using the SF-36 scores and OMAS was fair at 5.5 months post-surgery. Patients who have a unilateral ankle fracture are more likely to be unemployed or disabled in the aftermath of the fracture [17].
Bilateral ankle fractures remain a rare, complex orthopedic injury associated with a significant impact on quality of life. Effective post-operative rehabilitation over an extended period is necessary to attain optimal range of motion and return to pre-injury activities. To improve outcomes, we recommend psychotherapy for all patients with simultaneous bilateral ankle fractures.
This study demonstrates the importance of treating simultaneous bilateral ankle fractures in a multidisciplinary approach with patients involved in passenger vehicle accidents, as well as the impact on functional outcomes and the rarity of the orthopedic condition.
References
- 1.Kyriacou H, Mostafa AM, Davies BM, Khan WS. Principles and guidelines in the management of ankle fractures in adults. J Perioper Pract 2021;31:427-34. [Google Scholar | PubMed]
- 2.Zeng J, Xu C, Xu G, Wang D, Zhang W, Li H, et al. The global status of research in ankle fracture: A bibliometric and visualized study. Front Surg 2022;9:853101. [Google Scholar | PubMed]
- 3.Alrashedan B, Alghamdi E, Alromaih N. Bilateral simultaneous rotational ankle fractures: Case series and literature review. Int J Res Orthop 2023;9:572-6. [Google Scholar | PubMed]
- 4.Wire J, Hermena S, Slane VH. Ankle fractures. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. Available from: http://www.ncbi.nlm.nih.gov/books/NBK542324 [Last accessed on 2024 Mar 11]. [Google Scholar | PubMed]
- 5.Singh R, Kamal T, Roulohamin N, Maoharan G, Ahmed B, Theobald P. Ankle fractures: A literature review of current treatment methods. Open J Orthop 2014;4:292. [Google Scholar | PubMed]
- 6.Lampridis V, Gougoulias N, Sakellariou A. Stability in ankle fractures: Diagnosis and treatment. EFORT Open Rev 2018;3:294-303. [Google Scholar | PubMed]
- 7.Mirando M, Conti C, Zeni F, Pedicini F, Nardone A, Pavese C. Gait alterations in adults after ankle fracture: A systematic review. Diagnostics 2022;12:199. [Google Scholar | PubMed]
- 8.McPhail SM, Dunstan J, Canning J, Haines TP. Life impact of ankle fractures: Qualitative analysis of patient and clinician experiences. BMC Musculoskelet Disord 2012;13:224. [Google Scholar | PubMed]
- 9.Hays RD, Sherbourne CD, Mazel RM. The RAND 36-item health survey 1.0. Health Econ 1993;2:217-27. [Google Scholar | PubMed]
- 10.Olerud C, Molander H. A scoring scale for symptom evaluation after ankle fracture. Arch Orthop Trauma Surg 1984;103:190-4. [Google Scholar | PubMed]
- 11.Daly PJ, Fitzgerald RH Jr., Melton LJ, Ilstrup DM. Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand 1987;58:539-44. [Google Scholar | PubMed]
- 12.Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures--an increasing problem? Acta Orthop Scand 1998;69:43-7. [Google Scholar | PubMed]
- 13.Smeeing DP, Houwert RM, Briet JP, Kelder JC, Segers MJ, Verleisdonk EJ, et al. Weight-bearing and mobilization in the postoperative care of ankle fractures: A systematic review and meta-analysis of randomized controlled trials and cohort studies. PLoS One 2015;10: e0118320. [Google Scholar | PubMed]
- 14.McKeown R, Kearney RS, Liew ZH, Ellard DR. Patient experiences of an ankle fracture and the most important factors in their recovery: A qualitative interview study. BMJ Open 2020;10:e033539. [Google Scholar | PubMed]
- 15.Ponzer S, Nåsell H, Bergman B, Törnkvist H. Functional outcome and quality of life in patients with Type B ankle fractures: A two-year follow-up study. J Orthop Trauma 1999;13:363-8. [Google Scholar | PubMed]
- 16.Obremskey WT, Dirschl DR, Crowther JD, Craig WL 3rd, Driver RE, LeCroy CM. Change over time of SF-36 functional outcomes for operatively treated unstable ankle fractures. J Orthop Trauma 2002;16:30-3. [Google Scholar | PubMed]
- 17.Thakore RV, Hooe BS, Considine P, Sathiyakumar V, Onuoha G 2nd, Hinson JK, et al. Ankle fractures and employment: A life-changing event for patients. Disabil Rehabil 2015;37:417-22. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial
January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre
November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient
January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient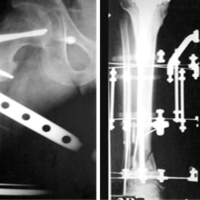 September 10, 2023 Treatment of Bifocal Periprosthetic Fractures above and below a Knee after Tumor using Spanning Ilizarov Device: A Case Report
September 10, 2023 Treatment of Bifocal Periprosthetic Fractures above and below a Knee after Tumor using Spanning Ilizarov Device: A Case Report