
Using a 16-gauge needle as a percutaneous sleeve for guide wire insertion in scaphoid fixation offers a simple, cost-effective, and reproducible technique. It enhances control over wire trajectory, minimizes soft tissue disruption, and eliminates the need for specialized jigs, making it highly suitable for resource-limited settings.
Dr. Warid Altaf, Department of Hand and Upper Limb Surgeon, Sancheti Advanced Ortho-care Hospital, Pune, Maharashtra, India. E-mail: waridaltaf@gmail.com
Innovation in surgery often lies not in complex technology, but in simple, reproducible techniques that deliver better outcomes with fewer resources. As a hand surgeon deeply involved in trauma and fixation techniques, I have always sought methods prioritizing precision, minimal invasiveness, and affordability. Over the past few years, We have developed and refined a percutaneous technique for Herbert screw fixation using a 16-gauge needle as a guidewire sleeve—a method that has now been successfully performed in 92 consecutive cases in last 5 years.
This technique, born out of a need for precision in confined spaces with minimal access, especially in scaphoid and small joint fractures, offers a new direction for percutaneous internal fixation. It is particularly relevant in the context of achieving a perfect and accurate placement of screw, rising healthcare costs, the need for quicker patient recovery, and the demand for outpatient-friendly and day-care procedures.
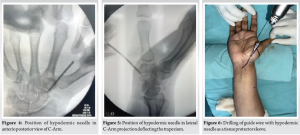
Herbert screw fixation remains a gold standard for treating certain intra-articular and small bone fractures, particularly in the scaphoid and metacarpals [1]. While conventional open methods provide direct visualization, they come with the baggage of soft-tissue trauma, increased operative time, and potential complications associated with larger incisions and hardware placement [2].
Even percutaneous methods using commercial sleeves or targeting jigs pose limitations: Cost, complexity, and difficulty in use, particularly in resource-constrained environments or high-volume trauma settings [3]. Moreover, guiding the wire in a precise trajectory through a small window in the bone, especially in small-sized hands or paediatric cases, can be challenging even for seasoned surgeons. Passing of the guide wire free hand always tends to bend as it is a flimsy 1 mm or 1.2 mm guide wire. The starting point at the distal pole of the scaphoid has to be very precise and accurate to get the best desired trajectory for the Herbert screw. The stout hypodermic needle is the solution to both problems; the bending of the traditional free hand guided wire, and also to get a proper trajectory while protecting the surrounding structures.
The another big advantage of this needle is to deflect the trapezium [Fig 1-5] on the dorsal side to get a better axis of drilling along the length of the scaphoid. Taking advantage of the sturdy nature of the needle, it is used to push the trapezium a little away to get a good central entry point, which is the most important step of the surgery.

The 16-Gauge Needle
Our approach utilizes a standard 16-gauge intravenous hypodermic needle as a sleeve for guidewire placement. This readily available, cost-effective tool allows the surgeon to achieve remarkable precision in placing the guidewire along the desired axis, eliminating the need for specialized jigs or elaborate instrumentation.
The 16G needle acts as a stabilizing cannula. Its narrow lumen snugly accommodates the standard guidewire used for Herbert screws. Once the trajectory is confirmed under fluoroscopy, the guidewire is inserted through the needle, ensuring minimal deviation or wobble. The needle’s sharp, tapered end also facilitates passage through the skin and subcutaneous tissue, reducing trauma and eliminating the need for a skin incision in many cases.
The patient is positioned as per the fracture type – commonly supine with the hand on a radiolucent table[Fig. 1]. Under image intensifier guidance, the fracture is reduced closed or with minimal manipulation. The 16-gauge needle is inserted at the desired entry point and advanced toward the fracture site in the required orientation.[Fig. 1,2]
Once the trajectory is deemed satisfactory, a guidewire is inserted through the needle. The needle is then withdrawn, and a cannulated drill is used to prepare the tract. The Herbert screw is inserted in standard fashion.[Fig. 10]
For a successful scaphoid surgery, a few key technical steps are crucial: achieving a precise entry point, ensuring that the guide wire is placed accurately along the central axis of the scaphoid in both antero-posterior [Fig. 6,7] and Lateral Views [Fig. 8,9] for optimal trajectory, and then carefully drilling over the guide wire followed by the correct placement of the Herbert screw along the same path[Fig. 10]. Each step demands meticulous execution to ensure proper compression, stability, and ultimately, a good functional outcome.
Marking of the long axis of the scaphoid under the image intensifier television in both anterior-posterior and lateral views[Fig. 1,2]. Note a folded sheet over the back of the wrist, causing extension.[Fig. 1]
Insertion of the hypodermic needle along the long axis of the scaphoid, starting at the distal pole of the scaphoid.[Fig. 3,4]
Point of entry in the lateral view. Note the bending of the hypodermic needle while deflecting the trapezium away to get a central trajectory.[Fig. 5]
Insertion of the guide wire following the markings drawn to get a central trajectory. To be confirmed in both anterior–posterior and lateral views.[Fig. 6-9]
Final placement of the screw.[Fig. 10]


Across 92 cases – including acute scaphoid fractures, non-unions, select distal pole injuries, and a few proximal pole fractures – the outcomes have been consistently favorable. The following advantages have been noted:
1. Minimal blood loss: The puncture-based entry results in negligible bleeding, often eliminating the need for even a suture.
2. Precision: The rigid metallic needle ensures that the guidewire follows an exact trajectory, reducing the chances of misplacement and the need for repositioning.[Fig 5]
3. Low morbidity: With no significant incision and minimal soft-tissue disruption, the risk of neurovascular injury, infection, or scarring is dramatically reduced.
4. Simplified technique: The learning curve for this approach is surprisingly gentle. Surgeons familiar with standard percutaneous methods can adapt to this method almost instantly.
5. Affordability: The 16G needle is inexpensive and universally available, making it ideal for both high-income institutions and under-resourced centres.
6. Faster union: The stability provided by the Herbert screw, coupled with less soft-tissue trauma, seems to encourage early fracture healing. In our series, most scaphoid fractures united within 8–10 weeks.
7. Better rehabilitation: Early mobilization was possible in most cases, thanks to the minimally invasive nature of the procedure. This is a game changer, especially for younger, active patients eager to return to work or sports.
This technique, while deceptively simple, may have a wider application. It encourages us to reconsider our fixation strategies and evaluate where expensive tools and systems can be replaced with innovative thinking. The approach aligns well with the principles of value-based care – delivering the best outcomes at the lowest cost.
For resource-limited settings, this method could potentially become a standard technique. In large trauma centres with high volumes, it could reduce operating time and material costs significantly. Its reproducibility also makes it a suitable candidate for training junior surgeons and residents.
Innovation does not always demand new inventions. Sometimes, it requires reimagining what we already have. The use of a 16-gauge needle as a sleeve for guidewire placement in Herbert screw fixation is a testament to this philosophy. It is cost-effective, efficient, and elegant in its simplicity. We believe this technique can significantly impact the way we approach small bone fracture fixation, especially in environments that demand both quality and economy.
References
- 1.Gutow AP. Percutaneous fixation of scaphoid fractures. J Am Acad Orthop Surg 2007;15:474-85. [Google Scholar | PubMed]
- 2.Rettig ME, Kozin SH, Cooney WP. Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-6. [Google Scholar | PubMed]
- 3.Adams BD, Blair WF, Reagan DS, Grundberg AB. Technical factors related to Herbert screw fixation. J Hand Surg Am 1988;13:893-9. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft
January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft December 1, 2024 Robotic-Assisted Total Knee Arthroplasty: Innovations, Precision, and the Future of Joint Reconstruction
December 1, 2024 Robotic-Assisted Total Knee Arthroplasty: Innovations, Precision, and the Future of Joint Reconstruction May 10, 2024 Partners in Precision: Cultivating Trust and Respect in the Surgeon-anesthetist Dynamics
May 10, 2024 Partners in Precision: Cultivating Trust and Respect in the Surgeon-anesthetist Dynamics November 10, 2019 A Case Report of Giant Cell Tumor of the Flexor Tendon Sheath in Index Finger
November 10, 2019 A Case Report of Giant Cell Tumor of the Flexor Tendon Sheath in Index Finger