
Osteoblastoma is a rare primary benign tumor that can affect the spine and cause painful scoliosis.
Dr. Mantu Jain, Department of Orthopedic, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. E-mail: montu_jn@yahoo.com
Introduction: Osteoblastoma constitutes 1% of all bone tumors and is more commonly localized to the spine.
Case Report: We present a case of a 12-year-old boy with painful scoliosis who was investigated further radiologically with computed tomogram and magnetic resonance imaging. The findings suggested D7-D8 osteoblastoma. The patient was operated under neuromonitoring with excision of the mass and later histopathologically confirmed. At 1 year follow-up, he is doing well. Osteoblastoma needs suspicion and early diagnosis and complete excision are important for treatment.
Conclusion: Osteoblastoma is a rare primary benign tumor that predominantly affects the spine. Young males with prolonged nonspecific back pain need prompt through radiological investigation. Surgical resection is the key with a good prognosis and low recurrence rates.
Keywords: Osteoblastoma, scoliosis, painful, dorsal spine.
Osteoblastoma originally described by Lichtenstein in 1950s as “osteogenic fibroma of bone” constitutes 1% of all bone tumors and is more commonly localized to the spine [1]. Osteoblastoma typically presents in the younger population mostly in the second decade with male preponderance [1,2]. Osteoblastoma is commonly located in the long bones and spine and is a rare presentation which can be further classified as conventional type or aggressive ones [3]. Children with painful scoliosis or night cries need further evaluation. Mild scoliosis that can be associated with compressive features can be seen in 30–50% of the patients with an aggressive variant of osteoblastoma [4]. Here, we present a case of destructive osteoblastoma of the dorsal spine in a male child who underwent excision with instrumentation with complete correction of his deformity and relief of pain.
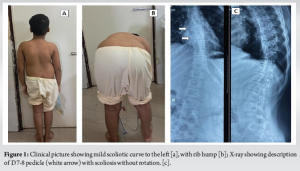
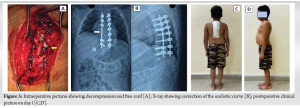
A 12-year-old male patient, student, presented to our outpatient department with complaints of pain in the middle back for the past 6 months which was insidious in onset, gradually progressive, mild to moderate in intensity, non-radiating but associated with night cries. The patient also complained of deformity in the back for a similar duration. On examination, there was tenderness over the dorsal spine, and a scoliotic deformity with convexity toward the left side with a small left-sided rib hump (Fig. 1a and b). Neurological examination was normal except that he had slight upper motor neuron features like extensor plantar response. The power in the bilateral lower limb was 5/5 as per the medical research council grade and sensory was also normal (2/2). Plain radiograph of the whole spine which revealed a scoliotic deformity of dorsal spine with convexity toward the left side with non-visualization of right-sided pedicles of D7 and D8 vertebrae (Fig. 1c). Further, a magnetic resonance imaging (MRI) was done which revealed a destructive lesion (3 × 4 cm) at D7 and D8 vertebra involving the central canal with surrounding soft-tissue extension (Enneking stage 3). It involves zones 10–12 with an extension to layer D as per Weinstein-Boriani-Biagini classification system [5], as illustrated in Fig. 2a-c. Non-contrast computed tomogram (NCCT) of the focal area revealed an expansile lytic lesion of size 3 × 4 cm with calcification involving spinous process, lamina, and pedicles of the right side of D7 and D8 vertebrae suggestive of osteoblastoma (Fig. 2d-f). Blood examinations were normal except for slightly elevated alkaline phosphatase values. The parents were counseled for surgical excision of the tumor and stabilization of segments using pedicle screw fixation. Under neuromonitoring guidance, using a standard posterior midline approach pedicle screw was inserted from D4 to D10 levels in a staggered arrangement. A connecting rod was given on one side for stabilization and open surgical resection of the tumor along with laminectomy and right-sided pedicles were removed at D7 and D8 vertebrae (Fig. 3a). Following excision and decompression, deformity was corrected by cantilever technique. Samples were taken for gross and histopathological examination and the wounds were closed in layers over a drain. The post-operative period was uneventful and the check x-ray was satisfactory (Fig. 3b). He was mobilized the 1st day after surgery (Fig. 3c). Histological report came to be consistent with the pre-operative diagnosis i.e. osteoblastoma (Fig. 4). The patient was followed up at, 4 weeks, 6 months, and 12 months after the surgery. He was doing well with fully active in school and sports activity.

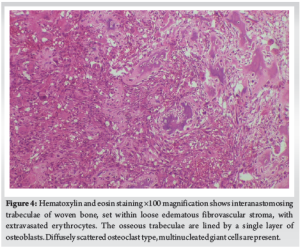
Osteoblastomas are rare benign bone tumors, accounting for about 1% of all primary bone tumors[1]. About 40–50% of them are located in the spine with the majority in the Dorsolumbar site followed by a cervical spine (20%) and another 17% in sacrum [3]. Precisely in the spine, the posterior elements – the spinous and transverse processes, pedicles, and the lamina are the preferred site affection and the vertebral body is are rare. Males within their second decade of life have higher preponderance with a ratio of M:F = 2–3:1. Osteoblastomas can vary in size between 2 and 6.5 cm. The literature describes two types of osteoblastomas: Conventional and aggressive forms. Nonspecific pain is the common complaint, but the presentation can be in the form of torticollis, scoliosis, or neurological deficit (in the aggressive type) [6]. This may result in a diagnostic delay, with an average lag period of 6–18 months following the initial symptom presentation [7]. The pathological hallmark of the tumors is the ability to produce osteoid and primitive woven bone amidst fibrovascular connective tissue similar to osteoid osteoma [4,8]. The lesion differs in the size (osteoid osteoma <2 cm, whereas osteoblastomas >2 cm). The aggressive variant of osteoblastomas is characterized by prominent nucleoli, larger and more irregular trabeculae, eosinophilic cytoplasm, and an increased frequency of osteoclast-like cells [4]. Approximately 10–15% of osteoblastoma cases exhibit components characteristic of aneurysmal bone cysts [9]. Other differential diagnosis osteosarcomas, or bone metastases [4]. Beta-catenin staining helps to differentiate. A positive staining of the nucleus suggests osteoblastoma, whereas cytoplasmic/membranous structures staining reflects osteosarcoma [10]. The classical radiological finding on an X-ray is a radiolucent nidus and surrounding sclerotic changes. The nidus may be calcified on the NCCT scan. The aggressive variant may present as an expansile lesion characterized by numerous small calcifications and a distinctly sclerotic margin (Enneking stage 2). The higher Enneking (stage 3) will have surrounded soft tissue extension with bony destruction [4]. On MRI, they display an intermediate to low signal on T1-weighted and an intermediate to high signal on T2-weighted scans [11]. However, bone scintigraphy remains the most sensitive investigation where lesions show increased uptake [12]. Treatment options for osteoblastomas can be considered based on the oncological grading of the tumor. There is an ongoing debate between intralesional marginal resection and en block resection, but there is no significant difference in the rate of recurrence in both [6]. Overall recurrence rates have been reported to be 10% [13]. Complete spondylectomy may be necessary in cases involving pan-vertebral structures, including both posterior elements and vertebral bodies [4]. Large osteoblastoma may benefit pre-operative embolization [6]. Radiotherapy and chemotherapy have been used for patients with unresectable lesions or in cases of recurrent disease [14].
Osteoblastoma is a rare primary benign tumor that predominantly affects the spine. Young males with prolonged nonspecific back pain need prompt through radiological investigation Surgical resection is the key with a good prognosis and low recurrence rates.
Osteoblastoma is a rare primary benign tumor that can affect the spine and cause painful scoliosis. Excision of the tumor is necessary to correct the deformity and relieve the symptoms of the patient.
References
- 1.Saccomanni B. Osteoid osteoma and osteoblastoma of the spine: A review of the literature. Curr Rev Musculoskelet Med 2009;2:65-7. [Google Scholar | PubMed]
- 2.Kan P, Schmidt MH. Osteoid osteoma and osteoblastoma of the spine. Neurosurg Clin N Am 2008;19:65-70. [Google Scholar | PubMed]
- 3.Argyriou AA, Panagiotopoulos V, Masmanidis A, Tzortzidis F, Konstantinou D. Destructive cervical spine osteoblastoma at C5 in a young patient initially presenting with quadriparesis: Case report and review of the literature. J Emerg Med 2013;44:e1–4. [Google Scholar | PubMed]
- 4.Galgano MA, Goulart CR, Iwenofu H, Chin LS, Lavelle W, Mendel E. Osteoblastomas of the spine: A comprehensive review. Neurosurg Focus 2016;41:E4. [Google Scholar | PubMed]
- 5.Boriani S, Weinstein JN, Biagini R. Primary bone tumors of the spine. Terminology and surgical staging. Spine (Phila Pa 1976) 1997;22:1036-44. [Google Scholar | PubMed]
- 6.Yin H, Zhou W, Yu H, Li B, Zhang D, Wu Z, et al. Clinical characteristics and treatment options for two types of osteoblastoma in the mobile spine: A retrospective study of 32 cases and outcomes. Eur Spine J 2014;23:411-6. [Google Scholar | PubMed]
- 7.Wan Y, Zhao W, Jiang Y, Liu D, Meng G, Cai Y. Β-catenin is a valuable marker for differential diagnosis of osteoblastoma and osteosarcoma. Hum Pathol 2014;45:1459-65. [Google Scholar | PubMed]
- 8.Jain M, Doki S, Gantaguru A, Mohakud S, Jha S. Osteoid osteoma of the body of the vertebrae causing painful scoliosis. Asian J Neurosurg 2020;15:1037-40. [Google Scholar | PubMed]
- 9.Hu H, Wu J, Ren L, Sun X, Li F, Ye X. Destructive osteoblastoma with secondary aneurysmal bone cyst of cervical vertebra in an 11-year-old boy: Case report. Int J Clin Exp Med 2014;7:290-5. [Google Scholar | PubMed]
- 10.Wu M, Xu K, Xie Y, Yan F, Deng Z, Lei J, et al. Diagnostic and management options of osteoblastoma in the spine. Med Sci Monit 2019;25:1362-72. [Google Scholar | PubMed]
- 11.Liu J, Han S, Li J, Yuan Y, Guo W, Yuan H. Spinal osteoblastoma: A retrospective study of 35 patients’ imaging findings with an emphasis on MRI. Insights Imaging 2020;11:122. [Google Scholar | PubMed]
- 12.Papanicolaou N, Treves S. Bone scintigraphy in the preoperative evaluation of osteoid osteoma and osteoblastoma of the spine. Ann Radiol (Paris) 1984;27:104-10. [Google Scholar | PubMed]
- 13.Singh DK, Das KK, Mehrotra A, Srivastava AK, Jaiswal AK, Gupta P, et al. Aggressive osteoblastoma involving the craniovertebral junction: A case report and review of literature. J Craniovertebr Junction Spine 2013;4:69-72. [Google Scholar | PubMed]
- 14.Berberoglu S, Oguz A, Aribal E, Ataoglu O. Osteoblastoma response to radiotherapy and chemotherapy. Med Pediatr Oncol 1997;28:304-9. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Osteochondroma Arising from Dorsal Pedicle Causing Compressive Myelopathy
January 1, 2026 Osteochondroma Arising from Dorsal Pedicle Causing Compressive Myelopathy November 1, 2025 Management of Solitary Osteochondroma Arising from Mammillary Process of D12 Vertebra in an 11-Year-Old Female: A Rare Case Report and Literature Review
November 1, 2025 Management of Solitary Osteochondroma Arising from Mammillary Process of D12 Vertebra in an 11-Year-Old Female: A Rare Case Report and Literature Review April 1, 2025 Transient Brachial Plexus Traction Palsy Following Scoliosis Deformity Correction Surgery – A Case Report
April 1, 2025 Transient Brachial Plexus Traction Palsy Following Scoliosis Deformity Correction Surgery – A Case Report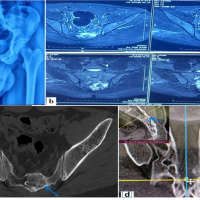 June 10, 2024 Sacral Osteoblastoma in a Young Male Presenting as Radicular Pain: A Rare Case Report
June 10, 2024 Sacral Osteoblastoma in a Young Male Presenting as Radicular Pain: A Rare Case Report