
Learning point of the article know that a elbow dislocation is an emergency requiring rapid reduction to avoid functional disorders.
Dr. Gueye Alioune Badara, Department of Orthopaedics, Order Malta Hospital Center, Malta, Dakar SENEGAL. E-mail: badoufa@live.fr
Introduction: Elbow dislocation is the second most common dislocation after shoulder dislocation in adults. It is said to be pure when it is not associated with a peri-articular bone fracture. Anterior elbow dislocation is rare, it is most often associated with significant trauma to the soft tissues. We report a case of an unusual type of neglected pure anterior elbow dislocation in a 16-year-old adolescent.
Case Report: A 16-year-old Koranic student, with no past medical history, who presented at the outpatient department with a closed injury to the left elbow resulting from a fight 3 months ago, during which his forearm was allegedly twisted. Elbow radiographs revealed an anterior elbow dislocation, with no associated fracture, with ossifications along the triceps brachii tendon. The patient was taken to the operating room, 4 months after injury, for an open reduction using the paratricipital approach. At the past follow-up of 15 months, the elbow regained an active flexion of 120°, extension was limited to 45°, pronation, and supination were complete and the elbow was painless. Assessment of the present state of the elbow was done using the mayo elbow performance score with an excellent score of 95.
Conclusion: Anterior elbow dislocation is an unusual form of acute elbow instability. It is a real trauma emergency that requires rapid and adequate treatment for better functional recovery.
Keywords: Elbow, anterior dislocation, adolescent.
Elbow dislocation is the second most common dislocation after shoulder dislocation in adults. It is said to be pure when it is not associated with a peri-articular bone fracture. Anterior elbow dislocation is rare, it is most often associated with significant trauma to the soft tissues [1-3]. Rupture or tension to the posterior stabilizers of the elbow, namely, the triceps tendon, the olecranon process and the posterior joint capsule, is a pre-requisite for the occurrence of the anterior form, these accounts to its infrequency. We report a case of an unusual type of neglected pure anterior elbow dislocation in a 16-year-old adolescent. Clinical examination revealed a painless elbow, a flexion deformity of 50° with an active flexion of 85°, a supinated forearm, depression on the posterior aspect of the elbow.
A 16-year-old Koranic student, with no past medical history, who presented at the outpatient department with a closed injury to the left elbow resulting from a fight 3 months ago, during which his forearm was allegedly twisted. The exact mechanism was poorly elucidated. Elbow radiographs revealed an anterior elbow dislocation, with no associated fracture, with ossifications along the triceps brachii tendon.
Initial treatment was carried out by a bonesetter by massages and limb traction. Subsequently, he consulted a hospital where a surgical intervention was suggested, which he declined. Faced with the lack of functional recovery, he presented to our health facility for proper management.
Clinical examination revealed a painless elbow, a flexion deformity of 50° with an active flexion of 85°, a supinated forearm, depression on the posterior aspect of the elbow, the bony prominence of the olecranon and other anatomical landmarks of the elbow were not palpable. The neurovascular examination was unremarkable.
Elbow radiographs revealed an anterior elbow dislocation, with no associated fracture, with ossifications along the triceps brachii tendon (Fig. 1).

The patient was taken to the operating room, 4 months after injury, for an open reduction using the paratricipital approach. Intraoperative findings were significant fibrosis filling the joint cavities, peri-articular ossifications, and the absence of fracture.
Removal of the fibrosis and ossifications permitted us to reduce the dislocation, which was maintained by a condylo-radial Kirschner pin with a flexed elbow at 90° (Fig. 2). An intraoperative fluoroscopy control was done using a C arm image intensifier and the vascular examination was normal.

The condylo-radial pin was removed at 4 weeks, and functional recovery was entrusted to the physiotherapist.
At the past follow-up of 15 months, the elbow regained an active flexion of 120°, extension was limited to 45°, pronation and supination were complete and the elbow was painless. Assessment of the present state of the elbow was done using the mayo elbow performance score (MEPS) with an excellent score of 95.
Anterior elbow dislocation is a rare injury [1-6]. It is most often associated with other lesions such as olecranon fracture, vascular and nerve lesions, and compartment syndrome [1-10]. It is a real trauma emergency that requires emergency diagnosis and treatment. The mechanism of injury is most often direct by a fall on the posterior aspect of a flexed elbow [1,2,4,5,9,10]. Cases of indirect mechanism by hyperextension of the elbow have been reported [8]. Our case illustrates an unusual presentation, in that it is a neglected pure anterior dislocation, without associated neurovascular complications. The mechanism of injury was not well elucidated. The initial treatment for a pure dislocation is closed reduction [5,6,10,11]. The indication for an open reduction is only made in the event of skin opening, neurovascular complication, fracture, irreducibility, or instability after reduction [1,2,4-6,8,9]. In this case, the longtime interval between injury and treatment (3 months) led to the development of fibrosis, filling the joint cavities, peri-articular ossifications, and capsular retraction which required open reduction and osteosynthesis using a condylo-radial pin on a flexed elbow at 90°. Many authors recommend early mobilization for better functional recovery [5,9,12]. In our case, pin removal was done at 4 weeks and active-passive mobilization was done at the physiotherapy and functional rehabilitation unit, with an excellent result at 15 months follow-up according to the MEPS.
Open surgical treatment for this case of neglected anterior elbow dislocation without fracture gave good results with minimal complications.
Anterior elbow dislocation is an unusual form of acute elbow instability. It is a real trauma emergency which requires rapid and adequate treatment for better functional recovery.
References
- 1.Kumar M. A rare case of simple anterior dislocation of elbow with brachial artery injury with posterior interosseous nerve palsy. Univ J Surg Surg Spec 2018;4:17-20. [Google Scholar | PubMed]
- 2.Chater L, Atarraf K, Arroud M, Afifi MA. La luxation antérieure du coude associée à une fracture de l’olécrâne : Une forme rare de luxation du coude chez l’enfant. J Traumatol Sport 2014;31:43-5. [Google Scholar | PubMed]
- 3.Hamadi HD. Les Luxations Récentes du Coude Chez L’adulte: Traitement Fonctionnel Versus Immobilisation: A Propos de 60 Cas, in Faculte de Médecine. Dakar: Université Cheikh Anta Diop; 2016. p. 103. [Google Scholar | PubMed]
- 4.Singh SG. A case of elbow dislocation. Med Leg Costa Rica 2019;36:166-70. [Google Scholar | PubMed]
- 5.Gyawali GP, Pokharel B, Pokharel RK. Irreducible anterior dislocation of the elbow without associated fracture. JNMA J Nepal Med Assoc 2013;52:398-401. [Google Scholar | PubMed]
- 6.Neviaser JS, Wickstrom JK. Dislocation of the elbow: A retrospective study of 115 patients. South Med J 1997;70:172-3. [Google Scholar | PubMed]
- 7.Diallo M. Luxations Traumatiques : Profil Epidémio-Clinique et Essai de Classification Intégrale, in Faculté de Médecine. Dakar: Université Cheikh Anta Diop; 2012. p. 113. [Google Scholar | PubMed]
- 8.Wilkerson RD. Anterior elbow dislocation associated with olecranon fractures--review of the literature and case report. Iowa Orthop J 1993;13:223-5. [Google Scholar | PubMed]
- 9.Kailash S, Shanmuganathan S. Anterior dislocation of elbow with neurovascular injury: A rare case report. J Orthop Case Rep 2017;7:91-4. [Google Scholar | PubMed]
- 10.Inoue G, Horii E. Combined shear fractures of the trochlea and capitellum associated with anterior fracture-dislocation of the elbow. J Orthop Trauma 1992;6:373-5. [Google Scholar | PubMed]
- 11.Ivo R, Mader K, Dargel J, Pennig D. Treatment of chronically unreduced complex dislocations of the elbow. Strategies Trauma Limb Reconstr 2009;4:49-55. [Google Scholar | PubMed]
- 12.Robinson PM, Griffiths E, Watts AC. Simple elbow dislocation. Shoulder Elbow 2017;9:195-204. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point
December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point November 1, 2025 Surgical Treatment of Neglected Elbow Dislocation with the Box-loop Technique: A Case Report
November 1, 2025 Surgical Treatment of Neglected Elbow Dislocation with the Box-loop Technique: A Case Report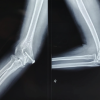 October 1, 2025 A Rare Repair: Trochlear Fracture Fixed With Headless Screws and Medial Epicondyle Osteotomy – A Case Report
October 1, 2025 A Rare Repair: Trochlear Fracture Fixed With Headless Screws and Medial Epicondyle Osteotomy – A Case Report August 1, 2025 Elbow Interpositional Arthroplasty using an Achilles Tendon Allograft: A Case Report
August 1, 2025 Elbow Interpositional Arthroplasty using an Achilles Tendon Allograft: A Case Report