
Asymmetric malaligned ankle osteoarthritis is a post-traumatic complication of malunited tibiotalar joint fractures, requiring a comprehensive approach. This case highlights the importance of restoring adequate fibular length, ensuring balanced joint load distribution, and the potential to avoid joint-sacrificing procedures through corrective osteotomies and proper patient selection. The present approach advocates for joint-preserving surgical treatments, offering insights into optimizing ankle malunion management for future considerations.
Dr. Olivier Cornu, Orthopaedic and Trauma Department – Cliniques universitaires Saint-Luc UCL, av Hippocrate 10 – 1200 – Brussels – Belgium. E-mail: olivier.cornu@uclouvain.be
Introduction: Post-traumatic fibular shortening results in malrotation and lateral talar tilt, disrupting joint congruence and increasing stress. These malunited ankle fractures lead to complications such as chronic pain, reduced mobility, and post-traumatic osteoarthritis. The impact of these malunions highlights the importance of anatomical reconstruction to restore biomechanical balance and prevent complications. This case study provides a detailed insight into the management of complex post-traumatic ankle deformities, highlighting the success of joint-preserving osteotomies and their potential to delay more invasive interventions.
Case Report: This case report illustrates the restoration of joint congruence in a patient presenting with chronic lateral-dorsal pain, limited mobility, and impingement symptoms of the ankle. The valgus deformity of the hindfoot and post-traumatic misaligned tibio-talar osteoarthritis were addressed through fibular Z-lengthening osteotomy with corticocancellous grafting and medializing calcaneal osteotomy.
Conclusion: This case underscores the importance of an early recognition and targeted surgical approach to correct complex post-traumatic deformities. Joint reconstruction, restoring the ankle mortise’s balance, has clinical benefits by reducing pain, improving ankle function, and preventing the development or progression of mechanical joint degeneration.
Keywords: Hindfoot valgus, valgus ankle osteoarthritis, supramalleolar fibular lengthening osteotomy, medializing calcaneal osteotomy, realignment surgery.
Proper ankle function relies on the complex balance of its anatomy, where even minor changes can significantly compromise functionality [1]. The role and importance of the lateral malleolus in talocrural joint function have been demonstrated, and a fibular shortening of 2 mm or an external rotation of 5° increases stress on the joint cartilage, already contributing to wear and pain [2]. Relative shortening of the fibula can occur after any type of ankle fracture involving the lateral malleolus. Hindfoot valgus deformity is caused by secondary abduction and lateral rotation of the talus [3]. Post-traumatic malunions of the ankle can be complex, combining fibular shortening, malposition of the malleoli, and syndesmotic injuries, often complicated by degenerative joint pathologies [4]. A malunion is defined as improper bone healing following a fracture, resulting in deformities such as length changes, misalignment, or angulation. It can result from initial unstable or inadequate reduction, positioning that compromises joint congruence, or abnormal bone rotation. An angular malunion occurs when the healed fracture creates abnormal tilting or curvature at the fracture site. When the biomechanical axes of the ankle joint structures are disrupted, abnormal stress distribution frequently leads to secondary chronic pain, functional instability, and, over time, promotes the development of post-traumatic osteoarthritis [4,5]. A malunited ankle fracture often involves a concomitant syndesmotic widening injury, which may lead surgeons to overlook alterations in fibular rotation or length [4]. Ankle osteoarthritis differs from other lower limb joints due to its predominantly post-traumatic etiology, affecting a demographic 12–15 years younger [6-9]. The time between the causal trauma and the development of osteoarthritis depends on the type and severity of the fracture, complications during the healing process, and patient-related factors, such as age [7]. Rotational ankle fractures, most of which involve significant damage to the lateral malleolus, are the main trauma type resulting in post-traumatic ankle osteoarthritis [8]. Treatment options depend on the severity of the deformity and can be categorized into joint-preserving surgery and joint-sacrificing surgery [10]. Compared to hip and knee arthritis, the clinical understanding and treatment of ankle arthritis are still in their infancy and explored mostly end-stage biomechanics [10,11]. Asymmetric ankle osteoarthritis remains challenging to manage since more than half of the joint surface is usually preserved [12]. This case adds valuable insights to the limited data on asymmetric ankle osteoarthritis, demonstrating the practical impact of joint-preserving surgical techniques.
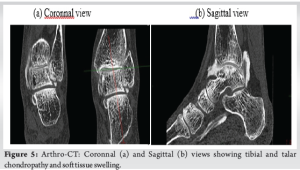
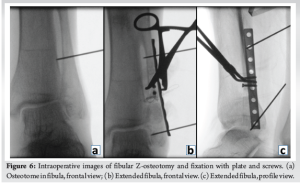
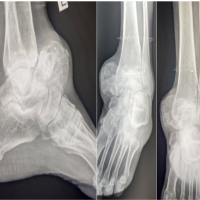
The causative fracture was a left tibia-fibula fracture in early childhood due to a road traffic accident, treated conservatively with casting. The lateral malleolar fracture was insufficiently reduced, resulting in significant fibular shortening. The 57-year-old patient presented with chronic lateral-dorsal pain in the left ankle, clinically accompanied by hindfoot valgus deformity and limited mobility with a submalleolar and anterior ankle impingement. The X-rays show bone remodeling and tibiofibular arthrodesis at the distal third (Fig. 1). Additional imaging included scintigraphy showing progressive tibio-talar osteoarthritis and early-stage Lisfranc joint osteoarthritis (Fig. 2). MRI and CT confirmed post-traumatic fibular shortening, consequent hindfoot valgus, and partially misaligned tibio-talar osteoarthritis in the lateral compartment (Figs. 3-5). Surgical management was indicated for the angular malunion, involving medializing calcaneal osteotomy and fibular lengthening osteotomy on the left ankle. Preoperative planning included standing anteroposterior (AP) and lateral radiographs of the ankle and hindfoot, as well as hindfoot alignment views (Saltzman view) to assess coronal malalignment. Full-length standing radiographs of both lower limbs were obtained to evaluate the mechanical axis. CT scan was used to precisely measure the degree of fibular shortening and tibiofibular joint fusion. MRI allowed for soft tissue and cartilage evaluation, particularly at the tibio-talar joint. Fibular shortening was assessed by comparing the level of the lateral malleolus to the plafond tibial and to the medial malleolus on the contralateral, uninjured side. Correction planning aimed to restore the fibular length to reestablish the normal relationship, targeting the lateral malleolus tip approximately 5–7 mm distal to the talar dome on the mortise view, which corresponds to the physiological fibular station. Angular correction involved planning for a 10° medial translation at the calcaneus level to correct the hindfoot valgus, based on hindfoot alignment measurements. Five weeks later, arthroscopy was performed for osteophyte removal as a second stage. The surgical procedure involved a Z-lengthening osteotomy of the , achieving approximately 9 mm of lengthening, fixed with two compression screws and a neutralization plate, supplemented by a corticocancellous graft harvested from the left anterior iliac crest (Fig. 6). The medializing calcaneal osteotomy required a medial displacement of the large tuberosity by 10 . The 10-mm medial shift was determined based on hindfoot alignment analysis, correcting approximately 1 mm/degree of valgus. This was achieved through lateral cortical osteotomy with the saw and medial completion with an osteotome, then fixed with two partially threaded titanium 7.0 compression screws (FixosR, Stryker, Mahwah, NJ 07430 USA) (Fig. 7). The surgery was performed under scopic guidance. Postoperatively, the non-weight-bearing period extended to 5 weeks, followed by an arthroscopy for osteophyte removal performed after the cast immobilization period. Physiotherapy was initiated 2 weeks later, following suture removal, with full weight-bearing allowed using a stabilizing ankle brace. No intra-operative or early postoperative complications were reported. Postoperative radiographs obtained at 6 weeks and at the final follow-up (24 weeks) illustrate satisfactory healing and a favorable clinical outcome (Fig. 8).




This report, while limited by being a single-case study and lack of long-term follow-up data, demonstrates significant strengths. Its comprehensive, patient-centered approach highlights the potential for long-term benefits, particularly relevant to younger demographics. It advocates for conservative surgical approaches, focusing on joint preservation techniques. Post-traumatic osteoarthritis of the ankle often initially manifests as asymmetric involvement of the tibiotalar joint. This typically leads to valgus or varus deformities of the hindfoot or ankle. Valgus deformity of the tibiotalar joint results from progressive degeneration due to lateral overload, and worsening joint imbalance [13]. Without treatment, this condition advances to end-stage osteoarthritis, characterized by generalized severe, debilitating joint damage [4,13]. In cases of early childhood trauma, failure of fibular consolidation can lead to valgus hindfoot deformity, which can be addressed by bone grafting to restore fibular stability. When growth is complete, osteotomy appears to become the preferred solution [14]. Realignment osteotomies aim to reposition structures to offload stressed regions. Indications include post-traumatic, degenerative, or developmental origins [15]. Our patient underwent a calcaneal osteotomy combined with a fibular osteotomy for three-dimensional correction. Lengthening the fibula is a crucial step in treating a painful ankle with fibular shortening after trauma. The primary clinical outcome determinant seems to be the degree of osteoarthritic involvement at the time of osteotomy. However, positive impacts on pain and function have been observed even in severely affected ankles [3]. Calcaneal osteotomy was initially described for correcting valgus foot deformities. Multiple variations of this method exist, tailored to specific needs, and can be combined in complex cases (e.g., medial sliding osteotomy, lateral column lengthening osteotomy, and Cotton osteotomy) [16]. Diagnosis and indications arise from a combined thorough clinical and weight-bearing radiological evaluation, assessing ankle and foot positioning [15,17,18]. These interventions aim to realign the hindfoot and restore the heel’s normal contact point, extending joint longevity [13]. Surgical planning requires considering osteotomy orientation and localization, syndesmosis involvement, reduction extent, and graft necessity [4]. An important consideration is that when the joint has been properly realigned, any subsequent operation, if needed, will be easier to perform and yield better outcomes [5]. Targeted osteotomy correction represents a conservative approach, avoiding more radical interventions like total ankle arthroplasty or arthrodesis [1,5,18].
This case underscores the importance of a comprehensive approach to managing complex post-traumatic complications, particularly in the context of valgus hindfoot deformities and distal fibula malunions. It highlights the need for accurate diagnosis and targeted surgical management to restore joint alignment and functional ankle anatomy. Understanding deformation mechanisms and indications for various osteotomy techniques is crucial, enabling good clinical and radiological outcomes in cases of asymmetric ankle osteoarthritis. This approach emphasizes the role of joint-preserving conservative surgeries, delaying mechanical degeneration progression and postponing more invasive interventions. This case contributes to the literature on realignment techniques for post-traumatic ankle deformities while emphasizing the importance of early management of childhood fractures to prevent long-term complications.
This case highlights the biomechanical and clinical repercussions of a malunited post-traumatic ankle fracture. It illustrates the importance of early recognition and management of asymmetric tibio-talar joint osteoarthritis. Realignment osteotomies address complex bone deformities, offering an conservative and effective approach to managing valgus hindfoot deformities and delaying the need for joint-sacrificing interventions. This treatment reduces chronic pain, restores mobility, and rebalances mechanical loads on the ankle mortise, improving quality of life and joint function. The case reaffirms the importance of comprehensive and early post-traumatic deformity management and joint-preserving surgeries. It enhances understanding of the relationship between mortise anatomy and biomechanics for improved management of traumatic and degenerative ankle conditions.
References
- 1.Mosca M, Buda R, Ceccarelli F, Fuiano M, Vocale E, Massimi S, et al. Ankle joint re-balancing in the management of ankle fracture malunion using fibular lengthening: prospective clinical-radiological results at mid-term follow-up. Int Orthop 2021;45:411 7. [Google Scholar | PubMed]
- 2.Thordarson DB, Motamed S, Hedman T, Ebramzadeh E, Bakshian S. The effect of fibular malreduction on contact pressures in an ankle fracture malunion model. J Bone Joint Surg Am 1997;79:1809. [Google Scholar | PubMed]
- 3.Weber D, Friederich NF, Müller W. Lengthening osteotomy of the fibula for post-traumatic malunion. Indications, technique and results. Int Orthop 1998;22:149 52. [Google Scholar | PubMed]
- 4.Chu A, Weiner L. Distal fibula malunions. J Am Acad Orthop Surg 2009;17:220 30. [Google Scholar | PubMed]
- 5.Giannini S, Faldini C, Acri F, Leonetti D, Luciani D, Nanni M. Surgical treatment of post-traumatic malalignment of the ankle. Injury 2010;41:1208 11. [Google Scholar | PubMed]
- 6.Valderrabano V, Horisberger M, Russell I, Dougall H, Hintermann B. Etiology of ankle osteoarthritis. Clin Orthop 2009;467:1800 6. [Google Scholar | PubMed]
- 7.Horisberger M, Valderrabano V, Hintermann B. Posttraumatic ankle osteoarthritis after ankle-related fractures. J Orthop Trauma 2009;23:60 7. [Google Scholar | PubMed]
- 8.Saltzman CL, Salamon ML, Blanchard GM, Huff T, Hayes A, Buckwalter JA, et al. Epidemiology of ankle arthritis. Report of a consecutive series of 639 patients from a tertiary orthopaedic center. Iowa Orthop J 2005;25:44 6. [Google Scholar | PubMed]
- 9.Hintermann B, Zwicky L, Schweizer C, Ruiz R, Barg A. The use of supramalleolar osteotomies in posttraumatic deformity and arthritis of the ankle. JBJS Essent Surg Tech 2017;7:e29. [Google Scholar | PubMed]
- 10.Alajlan A, Santini S, Alsayel F, Teoh KH, Alharbi W, Puls L, et al. Joint-preserving surgery in varus ankle osteoarthritis. J Clin Med 2022;11:2194. [Google Scholar | PubMed]
- 11.Li Y, Zhang H. [Ankle arthritis: Joint-preserving surgery and total ankle arthroplasty]. Zhongguo xiu fu chong jian wai ke za zhi zhongguo xiufu chongjian waike zazhi Chin. J Reparative Reconstr Surg 2023;37:769 75. [Google Scholar | PubMed]
- 12.Barg A, Pagenstert GI, Horisberger M, Paul J, Gloyer M, Henninger HB, et al. Supramalleolar osteotomies for degenerative joint disease of the ankle joint: Indication, technique and results. Int Orthop 2013;37:1683 95. [Google Scholar | PubMed]
- 13.Valderrabano V, Paul J, Monika H, Pagenstert GI, Henninger HB, Barg A. Joint-preserving surgery of valgus ankle osteoarthritis. Foot Ankle Clin 2013;18:481 502. [Google Scholar | PubMed]
- 14.Wiltse LL. Valgus deformity of the ankle: A sequel to acquired or congenital abnormalities of the fibula. J Bone Joint Surg Am 1972;54:595 606. [Google Scholar | PubMed]
- 15.Yi Y, Lee W. Peri-talar re-alignment osteotomy for joint preservation in asymmetrical ankle osteoarthritis. EFORT Open Rev 2017;2:324 31. [Google Scholar | PubMed]
- 16.Guha AR, Perera AM. Calcaneal osteotomy in the treatment of adult acquired flatfoot deformity. Foot Ankle Clin 2012;17:247 58. [Google Scholar | PubMed]
- 17.Lamm BM, Paley D. Deformity correction planning for hindfoot, ankle, and lower limb. Clin Podiatr Med Surg 2004;21:305 26, v. [Google Scholar | PubMed]
- 18.Pagenstert GI, Hintermann B, Barg A, Leumann A, Valderrabano V. Realignment surgery as alternative treatment of varus and valgus ankle osteoarthritis. Clin Orthop Relat Res 2007;462:156 68. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2023 Late Presentation of Giant Osteochondroma of Talar Neck in Elderly: A Case Report and Review of Literature
January 10, 2023 Late Presentation of Giant Osteochondroma of Talar Neck in Elderly: A Case Report and Review of Literature October 10, 2021 An Atypical Type of Monteggia Equivalent: A Case Report
October 10, 2021 An Atypical Type of Monteggia Equivalent: A Case Report January 28, 2015 Acute spontaneous atraumatic bilateral anterior dislocation of the shoulder joint with Hill-Sach’s lesions: A rare case
January 28, 2015 Acute spontaneous atraumatic bilateral anterior dislocation of the shoulder joint with Hill-Sach’s lesions: A rare case July 11, 2014 Abnormal Development of the Femoral Head Epiphysis in an Infant with no Developmental Dysplasia of the Hip Apparent on Ultrasonography
July 11, 2014 Abnormal Development of the Femoral Head Epiphysis in an Infant with no Developmental Dysplasia of the Hip Apparent on Ultrasonography